Parathyroid adenoma in detail
"parathyroid adenoma" AND "primary hyperparathyroidism"
Parathyroid adenoma: detailed overview
1) Epidemiology and importance
- PHPT is a common endocrine disorder and a major cause of hypercalcemia.
- Underlying lesion frequencies in PHPT:
- Adenoma: 85 to 95%
- Hyperplasia: 5 to 10%
- Carcinoma: around 1%
- Typical patient profile: adults, often over 50, female predominance.
2) Pathophysiology
In adenoma: this feedback set point is shifted, so PTH remains inappropriately elevated (or “normal but unsuppressed”) despite hypercalcemia.
- Increased bone resorption
- Increased distal tubular calcium reabsorption
- Increased phosphaturia
- Increased 1,25-dihydroxyvitamin D production
- High calcium
- Low/low-normal phosphate
- Elevated or inappropriately normal PTH
3) Molecular biology and genetics
- Cyclin D1 (CCND1) dysregulation (gene rearrangement/overexpression)
- MEN1 mutations in a subset of sporadic tumors
- CDC73 alterations are more linked to carcinoma/atypical neoplasms, but can occasionally occur in adenoma contexts
- MEN1, MEN2A, MEN4
- Hyperparathyroidism-jaw tumor syndrome (CDC73 related)
4) Pathology (gross and microscopic)
- Solitary, well-circumscribed, encapsulated tan to reddish-brown nodule
- Usually about 0.5 to 5 g
- Remaining glands often normal or shrunken (feedback suppression)
- Predominantly chief cells in sheets/nests
- Reduced stromal fat compared with normal gland
- Can show endocrine atypia (nuclear pleomorphism) without malignancy
- Mitotic figures uncommon
Histology image example
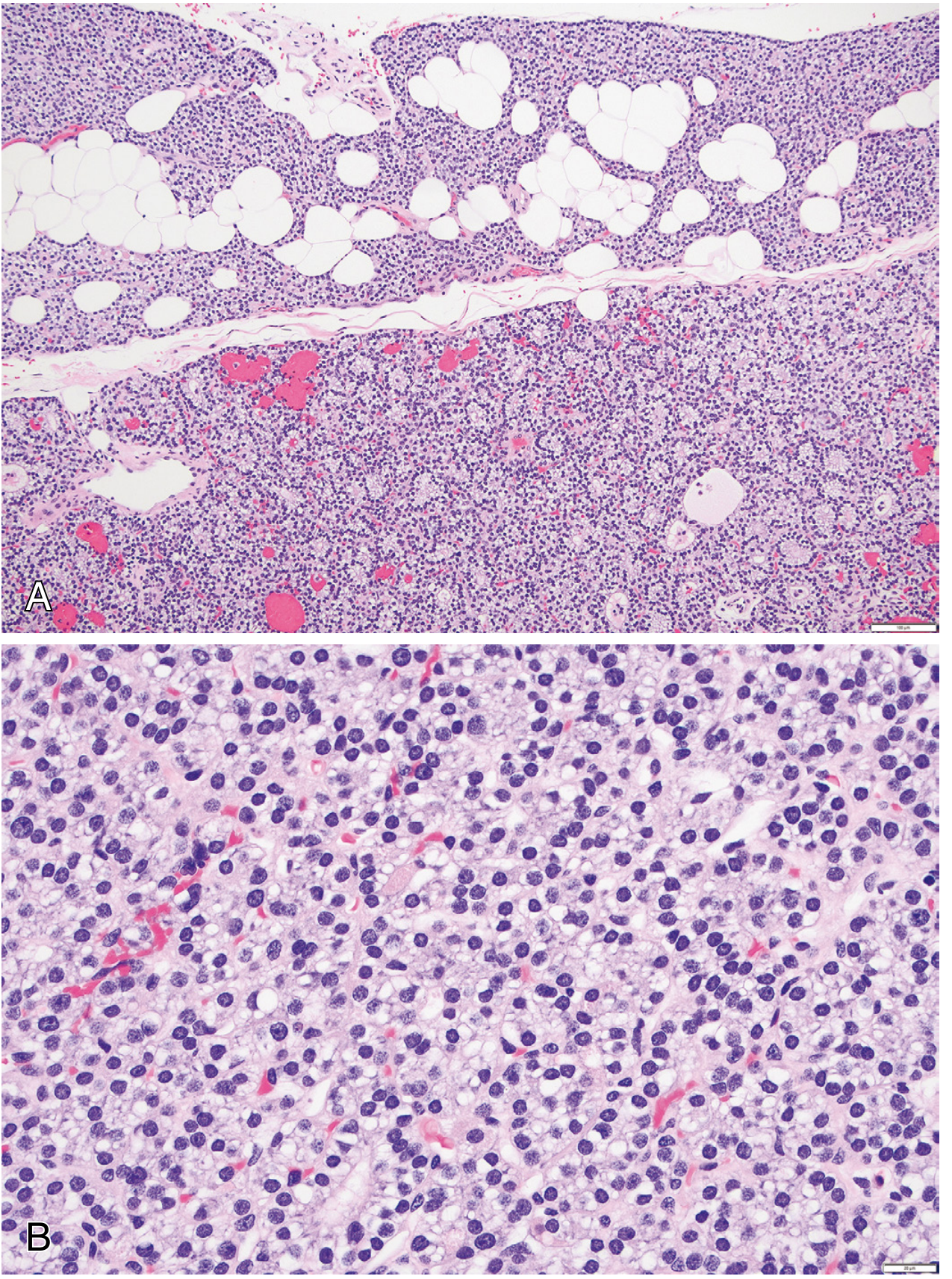
- Panel A shows adenoma tissue demarcated from residual fat-containing non-neoplastic parathyroid.
- Panel B shows monotonous chief-cell proliferation at higher power.
5) Clinical presentation
Classic symptomatic pattern, when present:
- “Bones”: bone pain, osteoporosis, osteitis fibrosa cystica, brown tumors
- “Stones”: nephrolithiasis, nephrocalcinosis
- “Groans”: GI symptoms (constipation, nausea, abdominal complaints, pancreatitis in some cases)
- “Psychic moans”: fatigue, mood/cognitive symptoms, depression, lethargy
6) Diagnosis
- Serum total and/or ionized calcium
- Intact PTH
- Phosphate, creatinine/eGFR
- 25-hydroxyvitamin D
- 24-hour urinary calcium (important to distinguish from familial hypocalciuric hypercalcemia)
- Bone mineral density (DXA), renal imaging in selected cases
- Hypercalcemic PHPT (most common)
- Normohormonal PHPT (high Ca with unsuppressed PTH)
- Normocalcemic PHPT (selected cases, after secondary causes excluded)
7) Imaging/localization modalities
- High-resolution neck ultrasound
- Tc-99m sestamibi scintigraphy (often with SPECT/CT)
- 4D-CT (useful in discordant/negative first-line imaging, ectopic/small lesions)
- MRI or PET/CT for difficult/reoperative cases
8) Treatment
- Focused/minimally invasive parathyroidectomy when localization is concordant
- Bilateral neck exploration when localization unclear, concern for multigland disease, or reoperative complexity
- Avoid unnecessary calcium restriction
- Replete vitamin D as appropriate
- Antiresorptives for bone protection in selected patients
- Calcimimetic therapy (cinacalcet) for calcium lowering in selected cases
9) Complications and postoperative issues
- Untreated disease: fracture risk, kidney stones, renal calcification, chronic hypercalcemia effects
- Post-op:
- Hypocalcemia (including hungry bone syndrome in severe bone disease)
- Persistent/recurrent hyperparathyroidism if multigland disease missed or ectopic tissue remains
- Intraoperative PTH monitoring is often used to confirm adequate excision (rapid PTH half-life supports this strategy)
10) Differential diagnosis
- Primary multigland hyperplasia
- Parathyroid carcinoma
- Familial hypocalciuric hypercalcemia
- Secondary/tertiary hyperparathyroidism (especially CKD context)
- Non-PTH hypercalcemia (malignancy, vitamin D excess, others)
Recent evidence check (last 2 years)
- PMID: 38739762 (skeletal effects of parathyroidectomy in PHPT)
- PMID: 41721481 (anesthesia approach in minimally invasive parathyroidectomy)
- PMID: 37929814 (4D-CT in discordant adenoma scans)
- surgery improves bone outcomes
- 4D-CT has an important role when first-line localization is discordant
Textbook sources
- Robbins, Cotran & Kumar Pathologic Basis of Disease, endocrine/parathyroid sections, histology and clinical features (pp. around 1010-1013 in extracted block context)
- Robbins & Kumar Basic Pathology, hyperparathyroidism morphology/clinical sections (pp. around 741-743 in extracted block context)
- Sabiston Textbook of Surgery, parathyroid surgery/localization/management chapter (pp. around 1541-1545 in extracted block context)
- a concise exam-oriented table (adenoma vs hyperplasia vs carcinoma), or
- a practical clinical algorithm for evaluating hypercalcemia and confirming parathyroid adenoma.
Yes and in a creative manner
1) Story mnemonic: “The One Rebel Gland”
- Bones: walls are mined for calcium → osteopenia/osteoporosis, bone pain, brown tumors in severe disease
- Kidneys: calcium stones clog river channels → nephrolithiasis/nephrocalcinosis
- Belly: villagers complain of constipation, nausea, abdominal discomfort
- Brain/Mood: fatigue, low mood, cognitive fog
Villain signature (lab pattern)
- Calcium: high
- PTH: high or “inappropriately normal”
- Phosphate: often low
- Urinary calcium: usually not low (helps separate from FHH)
2) Creative comparison table: “The 3 suspects in hyperparathyroidism court”
| Feature | Adenoma (The Lone Rebel) | Hyperplasia (The Four Cousins) | Carcinoma (The Invader) |
|---|---|---|---|
| Gland involvement | Usually single gland | Usually multigland | Usually single, invasive |
| Frequency in PHPT | Most common (85 to 95%) | 5 to 10% | Around 1% |
| Gross pattern | Well-circumscribed nodule | Diffuse/nodular enlargement of multiple glands | Hard/infiltrative mass |
| Histology clue | Chief-cell proliferation, low stromal fat | Hypercellularity in multiple glands, low fat | Diagnosis by invasion/metastasis, not cytology alone |
| Typical context | Sporadic most often | Sporadic or MEN syndromes | Rare, severe hypercalcemia more likely |
| Treatment | Focused excision if localized | Often broader exploration | En bloc oncologic approach |
3) Creative diagnostic algorithm: “Calcium Detective Map”
Step A: Confirm the crime
- High calcium found
- Check intact PTH
- If PTH high or not suppressed → PTH-dependent hypercalcemia (suspect PHPT)
Step B: Identify impostors
- Check 24-hour urinary calcium (or calcium/creatinine clearance ratio)
- Low urinary calcium suggests FHH rather than adenoma
Step C: Check damage report
- Bone: DXA ± fracture risk
- Kidney: creatinine/eGFR, stone screen (US/CT as needed)
Step D: Locate the rebel (only after biochemical diagnosis)
- Ultrasound ± sestamibi/SPECT
- If discordant or negative, consider 4D-CT
- Difficult/reoperative cases: MRI/PET options
Step E: Restore order
- Parathyroidectomy when indicated/suitable
- If not surgical candidate: medical monitoring, bone protection, calcium/vitamin D optimization, selective cinacalcet use
4) Ultra-short viva style memory hooks
- “Single gland, single culprit” = adenoma
- “PTH not suppressed despite high calcium” = primary hyperparathyroidism pattern
- “Diagnosis is biochemical, imaging is localization”
- “Adenoma first, hyperplasia second, carcinoma rare”
- a one-page colorful revision sheet, or
- 15 rapid-fire MCQs with explanations.
Yes
One-page revision sheet: Parathyroid Adenoma
Snapshot
- Definition: Benign neoplasm of parathyroid tissue causing autonomous PTH secretion
- Most common cause of PHPT: 85 to 95%
- Typical pattern: Single-gland disease
Core physiology in one line
Biochemical signature
- Serum calcium: high
- PTH: high or inappropriately normal
- Serum phosphate: often low
- Urinary calcium: usually normal/high (not low like many FHH cases)
Classic clinical picture
- Bones: osteopenia/osteoporosis, bone pain, severe cases with osteitis fibrosa cystica/brown tumors
- Stones: nephrolithiasis, nephrocalcinosis
- GI: constipation, nausea, abdominal discomfort
- Neuropsych: fatigue, mood/cognitive symptoms
Pathology pearls
- Usually solitary, well-circumscribed, soft tan nodule
- Chief-cell predominant, reduced stromal fat
- Endocrine atypia can occur and is not equal to carcinoma
- Other glands are often suppressed/shrunken
Adenoma vs hyperplasia vs carcinoma
- Adenoma: single gland, most common
- Hyperplasia: usually multigland
- Carcinoma: rare, diagnosis hinges on invasion/metastasis
Diagnostic algorithm (exam-safe)
- Confirm hypercalcemia
- Measure intact PTH
- If PTH-dependent pattern, exclude FHH (24-hour urinary calcium or Ca/Cr clearance ratio)
- Assess end-organ effects: bone density, renal status/stones
- Localize only after biochemical diagnosis: US + sestamibi/SPECT, then 4D-CT if needed
Management
- Definitive: parathyroidectomy
- Focused minimally invasive surgery when localization is concordant
- If non-surgical: monitoring, bone-directed therapy as needed, vitamin D optimization, selected cinacalcet use
High-yield pitfalls
- Imaging does not diagnose PHPT; labs do
- “Normal PTH” is abnormal if calcium is high
- Do not miss FHH before surgery decisions
15 rapid-fire MCQs (with answers)
1) Most common cause of primary hyperparathyroidism?
B. Parathyroid adenoma
C. Secondary hyperplasia
D. Vitamin D deficiency
Answer: B
2) Typical gland involvement in parathyroid adenoma?
B. Two glands always involved
C. Single gland in most cases
D. No gland enlargement
Answer: C
3) Typical biochemical pattern in adenoma-related PHPT:
B. High Ca, suppressed PTH
C. High Ca, high or inappropriately normal PTH
D. Low Ca, low PTH
Answer: C
4) Which is usually lower in PHPT?
B. Phosphate
C. Potassium
D. Chloride
Answer: B
5) Before localizing scans, the most important first step is:
B. 4D-CT
C. Biochemical confirmation of PHPT
D. PET-CT
Answer: C
6) Which test helps distinguish PHPT from FHH?
B. 24-hour urinary calcium
C. Serum amylase
D. Troponin
Answer: B
7) Histology most commonly seen in adenoma:
B. Squamous nests
C. Medullary thyroid pattern
D. Granulomatous inflammation
Answer: A
8) A key criterion for parathyroid carcinoma diagnosis:
B. Large size alone
C. Invasion/metastasis
D. High calcium alone
Answer: C
9) Classic symptom cluster includes all except:
B. Bone pain
C. Severe jaundice
D. Neuropsychiatric complaints
Answer: C
10) Definitive treatment for fit patient with symptomatic adenoma:
B. Thyroxine
C. Parathyroidectomy
D. Steroids
Answer: C
11) Which statement is correct?
B. Imaging is for localization after lab diagnosis
C. PTH must be very high in all cases
D. PHPT always causes symptoms
Answer: B
12) Common genetic alteration in sporadic adenomas:
B. CCND1 dysregulation
C. CFTR mutation
D. APC germline only
Answer: B
13) In many modern cases, PHPT is first found by:
B. Incidentally elevated calcium on routine labs
C. Emergency seizure only
D. Thyroid storm
Answer: B
14) Hyperplasia differs from adenoma because hyperplasia is usually:
B. Multigland process
C. Always malignant
D. Never associated with MEN syndromes
Answer: B
15) True regarding PTH in hypercalcemia due to adenoma:
B. It may be inappropriately normal
C. It is always zero
D. It is irrelevant diagnostically
Answer: B
Hyper parathyroidism in detail
Give me whole notes of rhinology parts from basic scince section of scott brown volume 1. Give ne those notes which you think from basic science that belongs to rhinology section
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.18.content.1.tool_result.content.0.image.source.base64: image exceeds 5 MB maximum: 7241544 bytes > 5242880 bytes
We encountered an error while processing your request. Please try again or reach out to us for help.
Give me notes of surgical approach to nasopharyngeal cancer from Scott brown vol 1
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.18.content.1.tool_result.content.0.image.source.base64: image exceeds 5 MB maximum: 7241544 bytes > 5242880 bytes
We encountered an error while processing your request. Please try again or reach out to us for help.
Stewart’s granulomatosis and sluder’s neuralgia in detail according to standard ent textbook
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.18.content.1.tool_result.content.0.image.source.base64: image exceeds 5 MB maximum: 7241544 bytes > 5242880 bytes
We encountered an error while processing your request. Please try again or reach out to us for help.
Principles and Application of MRI in ent according to standard ent textbook
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.18.content.1.tool_result.content.0.image.source.base64: image exceeds 5 MB maximum: 7241544 bytes > 5242880 bytes
We encountered an error while processing your request. Please try again or reach out to us for help.