Fever Ankle swelling and Joint pain what can be doffertials
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive breakdown of differentials for fever + ankle swelling + joint pain:
Differential Diagnosis: Fever + Ankle Swelling + Joint Pain
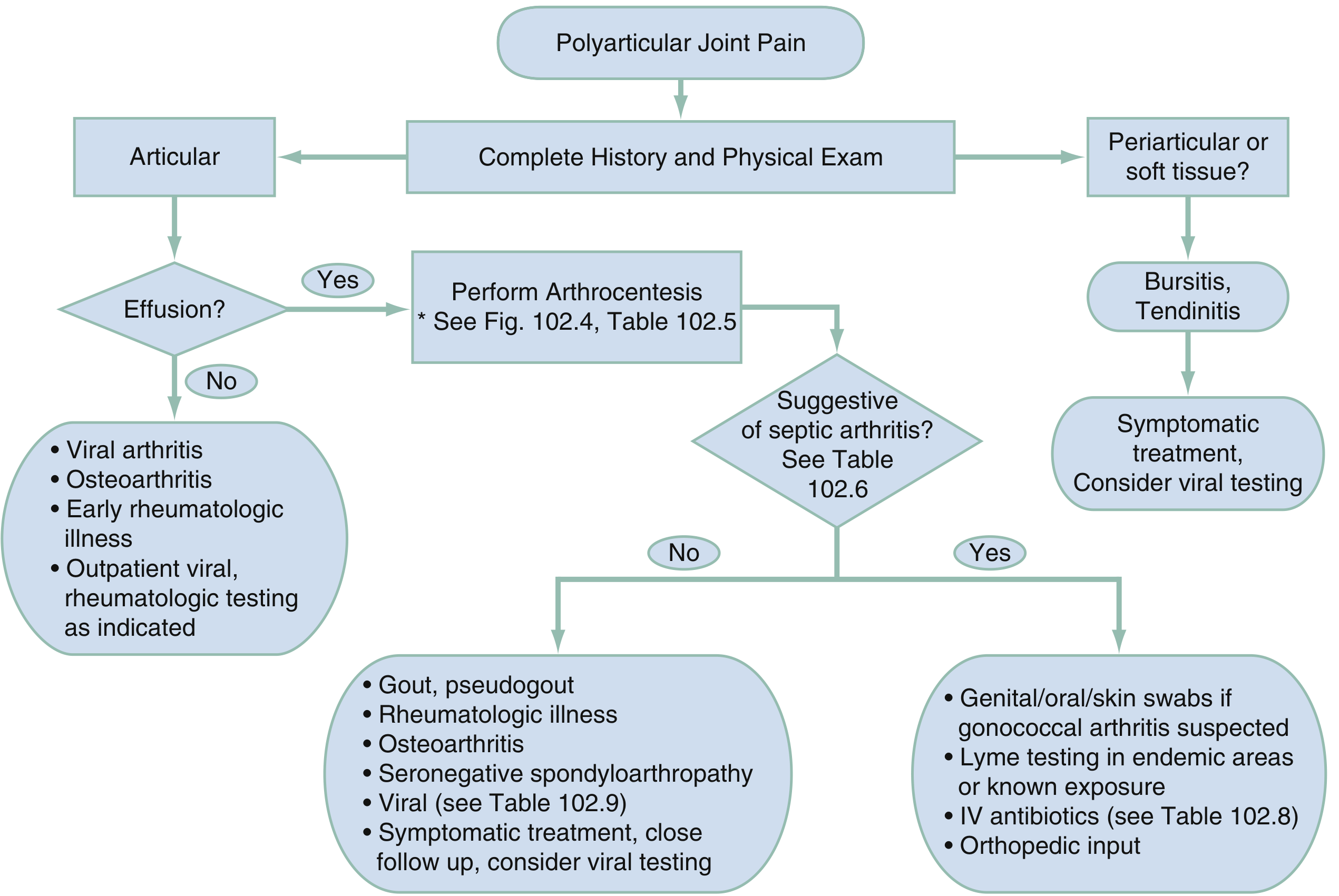
The combination points to an inflammatory or infectious arthropathy. The key initial question is: mono/oligoarticular vs. polyarticular? and is this septic (emergent) or non-septic?
Diagnostic Algorithm
1. INFECTIOUS (Highest Priority — Must Exclude)
Septic Arthritis (Bacterial)
- Fever, acute joint pain, effusion — most often a single large joint (knee > ankle > hip)
- Up to 20% can be polyarticular
- Common organisms: S. aureus, Streptococcus spp. (all ages); N. gonorrhoeae (young, sexually active)
- Fever may be blunted in elderly or immunocompromised patients
- Emergency — joint destruction occurs rapidly if untreated
-
ROSEN's Emergency Medicine, p. 2333–2336
Gonococcal (Disseminated GC) Arthritis
- Most common form of septic arthritis in young, sexually active adults
- Classic triad: migratory polyarthritis → tenosynovitis → dermatitis (pustular rash)
- Ankles, wrists, and knees most commonly involved
-
ROSEN's Emergency Medicine, p. 2336
Lyme Disease
- Tick exposure history; migratory arthritis pattern
- Knee > ankle involvement; associated with erythema migrans rash
-
ROSEN's Emergency Medicine, p. 2407
Viral Arthritis
| Virus | Key Features |
|---|---|
| Parvovirus B19 | Adults: RA-like symmetric polyarthritis |
| Hepatitis B/C | Symmetric migratory joint symptoms |
| HIV | Often monoarticular, feet and ankles |
| Chikungunya / Ross River | Mosquito-borne epidemic febrile polyarthritis, severe |
| Dengue / Zika | Acute joint and bone pain with high fever |
| Rubella | Arthritis in ~30% of adult females |
ROSEN's Emergency Medicine, Table 102.9
Infective Endocarditis
- Joint pain and fever with murmur; embolic phenomena
- Should be considered when fever + arthritis + cardiac risk factors
2. REACTIVE ARTHRITIS (Post-Infectious)
- Arthritis 1–4 weeks after GI infection (Salmonella, Shigella, Campylobacter, Yersinia) or STI (Chlamydia)
- Asymmetric oligoarthritis — lower limb predominant (knee, ankle)
- Classic triad: urethritis + conjunctivitis + arthritis
- Associated with HLA-B27
- Enthesitis (Achilles, plantar fascia) is a hallmark
-
Goldman-Cecil Medicine, p. 2802
3. ACUTE RHEUMATIC FEVER (ARF)
- Occurs 1–5 weeks after Group A Streptococcal pharyngitis
- Arthritis is the most common manifestation — migratory polyarthritis of large joints: knee, ankle, elbow, wrist
- Fever is universally present in the acute phase
- Other features: carditis, Sydenham's chorea, subcutaneous nodules, erythema marginatum
- Diagnosed by Jones Criteria: requires 2 major or 1 major + 2 minor criteria + evidence of streptococcal infection
-
ROSEN's Emergency Medicine, p. 1132
4. CRYSTAL ARTHROPATHIES
Gout
- Hyperuricemia; often monoarticular (first MTP, ankle, knee)
- Presents with acute severe pain, swelling, erythema, and warmth
- Fever can occur during acute flares; may mimic septic arthritis
Pseudogout (CPPD)
- Calcium pyrophosphate crystals; knee and wrist predominate
- Acute flares simulate septic arthritis with fever + hot, swollen joint
5. SERONEGATIVE SPONDYLOARTHROPATHIES
- Ankylosing Spondylitis: peripheral oligoarthritis in 30%, lower limbs, asymmetric; heel pain/enthesitis
- Psoriatic Arthritis: asymmetric, axial + peripheral; associated psoriatic skin/nail changes
- Enteropathic Arthritis: associated with Crohn's disease or ulcerative colitis
- All are HLA-B27 associated; ankle involvement is common
-
Goldman-Cecil Medicine, Table 244-2
6. RHEUMATOID ARTHRITIS (RA)
- Usually symmetric small joint involvement (PIPs, MCPs of hands), but can affect ankles
- ~20% present acutely; constitutional symptoms (fatigue, malaise, low-grade fever, weight loss)
- Morning stiffness >1 hour
-
ROSEN's Emergency Medicine, p. 2340
7. SYSTEMIC RHEUMATOLOGIC DISEASES
| Condition | Key Clues |
|---|---|
| SLE | Young female; malar rash, photosensitivity, multi-organ; arthritis + fever |
| Adult-onset Still's disease | Quotidian fever (evening spikes), salmon-pink rash, arthritis; ferritin markedly elevated |
| Vasculitis | Fever, rash, arthritis + multi-system involvement |
| Sarcoidosis | Löfgren syndrome: bilateral ankle arthritis + erythema nodosum + hilar adenopathy |
8. OTHER CAUSES
- Hyperlipoproteinemia — Self-limited mono/oligoarticular arthritis involving knee or ankle
- Carcinomatous polyarthritis — Paraneoplastic; asymmetric, large joints
- Sickle cell disease — Vaso-occlusive crisis with periarticular pain and swelling; fever from infection
Key Diagnostic Steps
| Test | Purpose |
|---|---|
| Joint aspiration (arthrocentesis) | Mandatory to exclude septic arthritis; crystals, WBC, culture |
| WBC, ESR, CRP | Elevated in inflammation/infection (nonspecific) |
| Blood cultures | If systemic sepsis/endocarditis suspected |
| ASO titre, throat culture | Acute rheumatic fever |
| RF, anti-CCP | Rheumatoid arthritis |
| ANA, dsDNA | SLE |
| HLA-B27 | Spondyloarthropathies |
| Uric acid | Gout |
| Lyme serology | Endemic exposure |
| STI swabs/NAAT | Gonococcal arthritis |
| Ferritin | Adult-onset Still's (often >10,000 µg/L) |
Bottom line: Fever + ankle swelling + joint pain is septic arthritis until proven otherwise. Arthrocentesis (joint aspiration) is the single most important diagnostic step. Once septic arthritis is excluded, work through the infectious, reactive, crystal, and rheumatologic differentials based on clinical pattern.
Sources: ROSEN's Emergency Medicine; Goldman-Cecil Medicine; Textbook of Family Medicine
This is a shared conversation. Sign in to Orris to start your own chat.