32 years old male, admitted to the center yesterday, associated with vomiting today morning. When he came to hospital, was found to have ST elevation in anterior leads, followed by ST depression in one and AVL. Later on, patient loading was given and after 2-3 hours, the brain, it's settling now and ECG also shows ST elevations deteriorations. Can you see? He is symptomatic as of now. What to be done next?
Reading File
Finding Sources
Finding Sources
Searching PubMed
failed thrombolysis STEMI rescue PCI
Reading File
Reading File
Reading File
Searching PubMed
rescue PCI fibrinolysis STEMI guidelines
Loading Image
Reading File
I now have everything needed for a thorough, well-cited answer. Let me synthesize.
Clinical Situation: STEMI with Failed Fibrinolysis - This is a Rescue PCI indication
This 32-year-old male has an anterior STEMI (ST elevation in anterior leads) with reciprocal ST depression in lead I and aVL, received thrombolytic ("loading") therapy, but after 2-3 hours remains symptomatic with persistent or worsening ST elevations rather than resolution. This is the textbook definition of failed fibrinolysis / failed thrombolysis.
Criteria Confirming Failed Reperfusion
Signs of successful reperfusion would be:
- Chest pain relief
- ≥50% reduction in ST-segment elevation at 60-90 minutes post-fibrinolysis
- Reperfusion arrhythmia (accelerated idioventricular rhythm)
This patient has none of these - he is still symptomatic and ECG shows persistent/worsening ST elevations at 2-3 hours. That is unequivocal failure.
What to Do Next: RESCUE PCI - URGENT
"ST-segment elevations that do not normalize 60-90 minutes following fibrinolysis should undergo rescue PCI."
- Washington Manual of Medical Therapeutics
"In patients treated with a fibrinolytic, urgent coronary angiography should be performed if there is evidence of failure of reperfusion (persistent chest pain and ST-segment elevation >90 min), in which case a rescue PCI should be considered."
- Harrison's Principles of Internal Medicine 22E, p. 2163
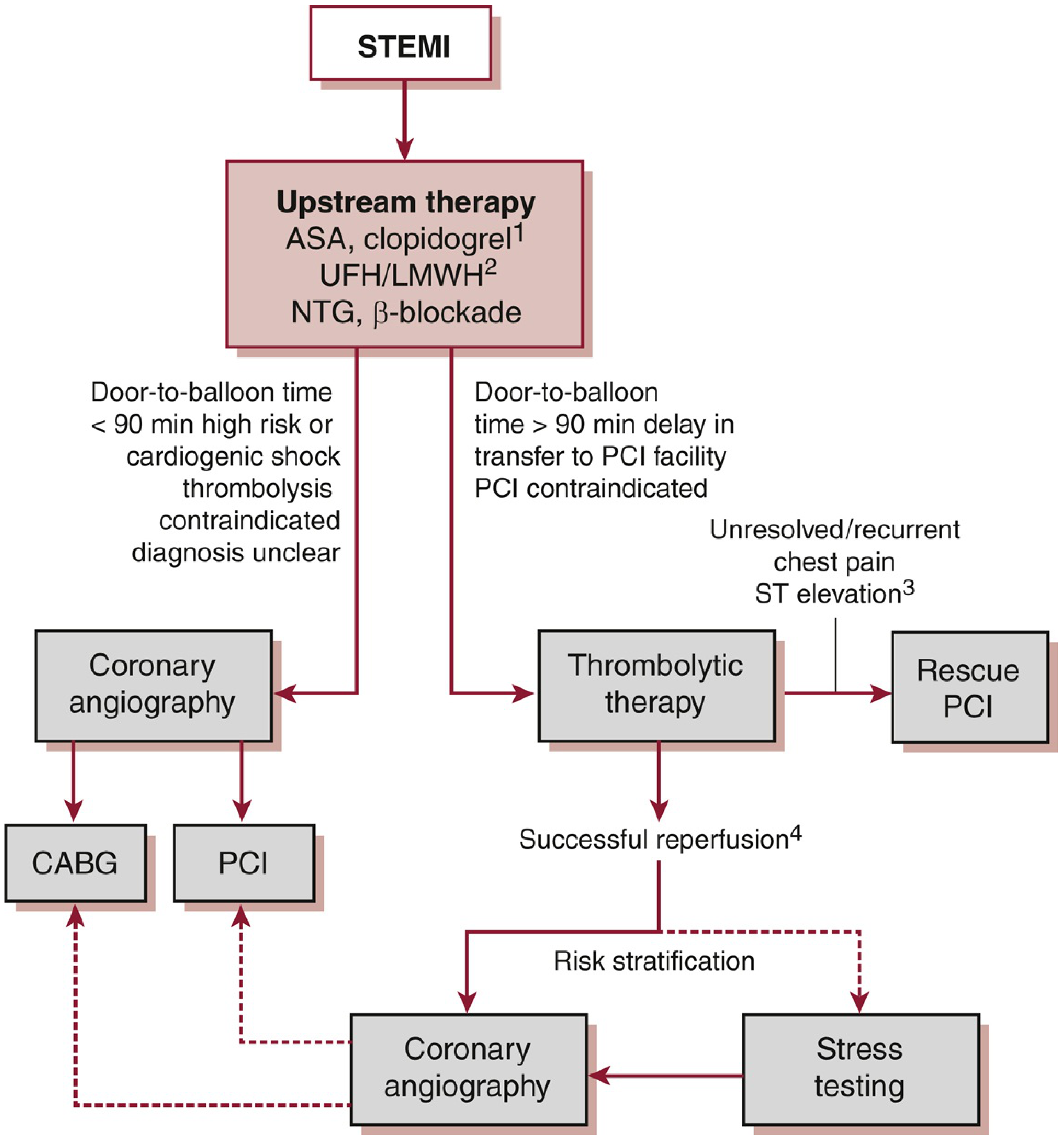
The reperfusion pathway is shown in the flowchart below:
Immediate Action Steps
1. Activate the cath lab NOW - Transfer for emergency coronary angiography + rescue PCI
- Do not wait further. Every minute of delay = more myocardium lost. This is an anterior STEMI (LAD territory) in a 32-year-old - the stakes are very high.
- Transfer to a PCI-capable center immediately if not already there.
2. Antiplatelet therapy
- If the patient received fibrinolysis and only clopidogrel was given as the P2Y12 agent (as per protocol), do not switch to ticagrelor or prasugrel yet (wait until post-PCI if anatomy is defined and no CABG needed).
- Ensure aspirin is on board.
- Ensure heparin (UFH or LMWH) is running - bivalirudin is an alternative in the cath lab.
3. Continue supportive care during transfer
- IV access, continuous ECG monitoring, defibrillator available.
- Oxygen if SpO2 <90%.
- IV morphine 2-4 mg for refractory chest pain.
- Avoid unnecessary arterial/venous punctures (bleeding risk post-fibrinolysis).
4. In the cath lab
- Coronary angiography to identify the culprit artery (almost certainly proximal/mid LAD given anterior STEMI + aVL reciprocal change).
- Rescue PCI with stenting of the infarct-related artery.
- Note: In STEMI without cardiogenic shock, PCI of non-culprit vessels can be done either at the index procedure or within 45 days (PRAMI, COMPLETE trials). Do NOT routinely intervene on non-culprit vessels at the index procedure if in cardiogenic shock.
5. Monitor for complications
- This patient is young and has a large anterior territory at risk - watch for:
- Cardiogenic shock (Killip class assessment)
- VF/VT (have a defibrillator at bedside)
- Complete AV block if RCA involvement (less likely given anterior pattern)
- Pericarditis/mechanical complications (later)
Why Not Re-Thrombolyse?
A second dose of thrombolytic is not recommended - it increases hemorrhagic risk without additional efficacy. Rescue PCI is the correct strategy.
Key Summary Table
| Criterion | This Patient |
|---|---|
| Time window | Still within salvageable window (young patient, 2-3 h post-lysis) |
| Reperfusion success? | No - still symptomatic, persistent ST elevation |
| Correct next step | Urgent rescue PCI |
| Anticoagulation | UFH/bivalirudin in cath lab |
| Antiplatelet | ASA + P2Y12 (clopidogrel if pre-given; escalate post-PCI) |
Bottom line: This is a failed fibrinolysis scenario requiring immediate transfer for rescue PCI. Do not delay further medical therapy while waiting - activate the cath lab, get the patient to the wire. The evidence and all major guidelines (ACC/AHA, ESC, Harrison's, Washington Manual) uniformly support this as the standard of care.
Sources: Harrison's Principles of Internal Medicine 22E, p. 2163; Washington Manual of Medical Therapeutics (Acute Coronary Reperfusion section); Goldman-Cecil Medicine; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.