Measles
Reading File
Finding Sources
Searching PubMed
measles rubeola
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full response.
Measles (Rubeola)
Definition
Measles (rubeola, morbilli) is an extremely contagious systemic viral illness caused by measles virus - a single-stranded RNA virus of the family Paramyxoviridae, genus Morbillivirus. It is characterized by high fever, erythematous maculopapular rash, cough, coryza, and conjunctivitis (the "3 Cs"). At least 24 genotypes exist, but there is only one serotype, so infection or adequate immunization confers broad protection against all strains.
- Goldman-Cecil Medicine, p. 3555
Epidemiology
Measles may be the most contagious pathogen known to humans, with an R₀ of 12-18 (compare: influenza R₀ = 2-3, Ebola R₀ = 2-3). It has no non-human reservoir.
-
Global deaths fell from >500,000/year in 2000 to 109,000 in 2017, then rose to >200,000 in 2019 following vaccine coverage gaps
-
The COVID-19 pandemic disrupted immunization programs globally - by 2022, only 83% of children received a first dose (lowest since 2008)
-
An estimated 24.7 million children did not receive even an initial vaccine dose in 2021
-
Herd immunity requires 89-94% population coverage
-
Goldman-Cecil Medicine, p. 3555-3556; Robbins Pathologic Basis of Disease, p. 1136
Pathogenesis
The virus enters via the respiratory tract or conjunctiva, then:
- Infects CD150/SLAM1-expressing T and B cells in regional lymph nodes
- Spreads to spleen, tonsils, and lymphoid tissues via infected mononuclear cells
- Causes viremia with dissemination to skin, GI tract, kidney, liver, CNS
- Later infects respiratory epithelium through the Nectin-4 receptor, causing sloughing and coughing of infectious droplets
Three receptors for measles hemagglutinin protein have been identified:
- SLAMF1 (CD150) - on activated lymphocytes, dendritic cells, monocytes; initial infection receptor
- Nectin-4 - on basal surface of epithelial cells; important for replication and spread in the respiratory tract
- CD46 (found on all nucleated cells, relevant for vaccine strains)
Immune suppression is a hallmark: measles virus depletes subsets of both T and B cells, erasing immune memory. This immune amnesia leads to increased all-cause mortality for months to years after infection, beyond the acute illness itself.
- Robbins Pathologic Basis of Disease, p. 1141-1143; Goldman-Cecil Medicine, p. 3557
Clinical Features
Timeline
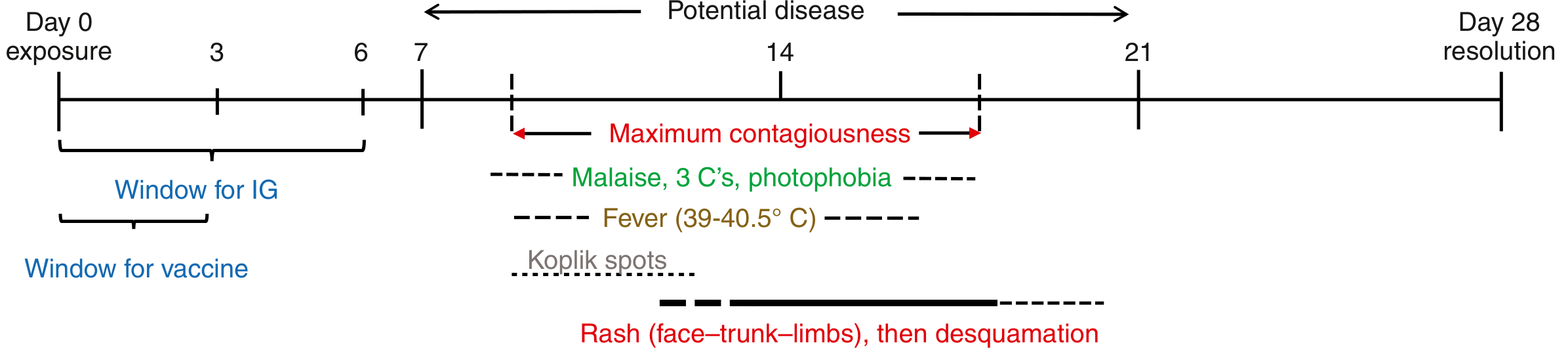
Disease timeline showing incubation, prodrome, Koplik spots, rash, and post-exposure prophylaxis windows
Incubation Period
9-12 days (range up to 21 days).
Prodrome (Days 8-11 post-exposure)
- Fever (39-40.5°C), often the highest of any childhood viral illness
- 3 Cs: Cough, Coryza (nasal congestion/coryza), Conjunctivitis
- Malaise, photophobia
- Koplik spots (pathognomonic) - appear 1-2 days before the rash
Koplik Spots (Enanthem)
Pathognomonic for measles. 1-mm white papules on an erythematous base, appearing first on the buccal mucosa opposite the lower molars, spreading to involve the rest of the buccal mucosa and pharynx.

Koplik spots - small white papules on erythematous buccal mucosa (Andrews' Diseases of the Skin)
Exanthem (Rash)
Appears 1-7 days after prodrome onset. Starts at the anterior hairline and behind the ears as discrete erythematous macules/papules that gradually coalesce and spread craniocaudally: face → trunk → extremities over 2-3 days.
- By day 3, the entire body is involved
- Lesions most confluent in initially involved areas (face)
- Fades after 6-7 days with simultaneous defervescence
- May desquamate in malnourished children

Variable rash of measles: classic rash (A), appearance on dark skin (B), desquamating dermatitis in malnutrition (C) - Goldman-Cecil Medicine

Rubeola (measles) - confluent erythematous rash on face - Andrews' Diseases of the Skin
Contagiousness
Infected persons are contagious from 4 days before to 4 days after rash onset (peak contagiousness days 7-14 post-exposure).
Complications
| Complication | Frequency / Notes |
|---|---|
| Otitis media | Most common complication |
| Pneumonia (primary viral or secondary bacterial) | Leading cause of death in children |
| Encephalitis (acute) | 0.1-0.3% of cases; 20% fatal, >1/3 with permanent sequelae |
| Measles inclusion body encephalitis | In immunocompromised; 1-6 months post-infection; focal seizures |
| Subacute sclerosing panencephalitis (SSPE) | 4-11 per 100,000 survivors; fatal; develops 7-10 years after infection |
| Thrombocytopenic purpura | Rare |
| Keratitis / blindness | In malnourished/vitamin A-deficient |
| Diarrhea + protein-losing enteropathy | In resource-poor settings |
| Fetal loss | Infection in pregnancy |
SSPE is uniformly fatal: patients develop cognitive/behavioral changes, then motor decline, visual loss, and vegetative state. Risk is several-fold higher if measles occurs before age 2. It is caused by a mutant measles virus that accumulates mutations allowing cell-to-cell spread without forming fully infectious viral particles.
- Goldman-Cecil Medicine, p. 3558; Robbins, p. 1143
Diagnosis
Clinical diagnosis is supported by the triad of prodrome + Koplik spots + craniocaudal maculopapular rash. Confirmation is by:
- RT-PCR - from nasopharynx, oropharynx, conjunctiva, or urine (most sensitive; also allows genotyping)
- Serology - measles-specific IgM (detectable from day 1 of rash in unvaccinated); or 4-fold rise in IgG in acute/convalescent samples
Lab findings: leukopenia and lymphopenia are characteristic.
For SSPE: EEG shows classic periodic stereotypic sharp-slow wave discharges, with high measles IgM and IgG titers in both CSF and serum.
Differential diagnosis: Rubella, scarlet fever, roseola, secondary syphilis, enterovirus infections, drug eruptions, Kawasaki disease.
- Goldman-Cecil Medicine, p. 3559
Treatment
Treatment is primarily supportive:
- Fever control, hydration, nutrition
- Monitor closely for pneumonia and encephalitis
- Infection control precautions (airborne)
Vitamin A supplementation (WHO-recommended):
- Reduces mortality and prevents xerophthalmia/corneal scarring/blindness
- Dosing:
- Infants < 6 months: 50,000 IU on days 1 and 2
- Children 6-11 months: 100,000 IU on days 1 and 2
- Patients ≥ 12 months: 200,000 IU on days 1 and 2
- Additional dose 2-6 weeks later if ophthalmic findings of vitamin A deficiency
- Indicated especially for children with malnutrition, vitamin A deficiency, immunodeficiency, or recent immigration from high-mortality areas
No antiviral therapies are proven for uncomplicated measles. Ribavirin, interferon-alpha, and isoprinosine have been used anecdotally for CNS complications (SSPE, inclusion body encephalitis) with limited evidence.
- Goldman-Cecil Medicine, p. 3560; Andrews' Diseases of the Skin, p. 458; Red Book 2021
Prevention
Vaccination
- MMR (or MMRV) live-attenuated vaccine - provides long-lasting antibody and cellular immunity
- Schedule (standard):
- Dose 1: 12-15 months (can give as early as 6 months in outbreaks/high-risk travel)
- Dose 2: 4-6 years (or at least 1 month after dose 1)
- If dose 1 given before 9 months, a third dose is required
- Herd immunity threshold: 89-94% coverage
Post-Exposure Prophylaxis (PEP)
Effective within 6 days of exposure:
| Population | PEP Option | Window |
|---|---|---|
| Unvaccinated / healthy ≥12 months | MMR vaccine | Within 72 hours (3 days) |
| Infants < 6-12 months, pregnant women, immunocompromised | Immunoglobulin (IG) | Within 6 days |
A 2025 systematic review in Vaccine (PMID: 39787800) evaluated post-exposure prophylaxis strategies for measles.
Atypical / Modified Measles
- Modified measles: Milder form in partially immune hosts (prior infection or vaccine); less prominent rash
- Measles in immunocompromised: Rash may be absent or minimal; prolonged course; higher mortality; presentation may be atypical
- "Black measles": Rare, DIC-like hemorrhagic complication; purpura prominent on extremities
Recent Evidence (2025-2026)
Three recent systematic reviews are relevant:
- Post-exposure prophylaxis for measles prevention (Vaccine, 2025) - PMID 39787800
- Adverse events following measles vaccines in infants <12 months (Vaccine, 2025) - PMID 39799850; a meta-analysis evaluating safety of early MMR dosing
- Acute management of measles - therapeutic strategies (Antiviral Res, 2026) - PMID 41638401; a 2026 systematic review on treatment options
Note: The 2026 systematic review on acute measles management (PMID 41638401) postdates the textbooks cited here. It may contain updated evidence on antiviral strategies - consult it if managing a clinical case.
Sources: Goldman-Cecil Medicine (International Ed.); Robbins, Cotran & Kumar Pathologic Basis of Disease; Andrews' Diseases of the Skin; Red Book 2021 (AAP)
This is a shared conversation. Sign in to Orris to start your own chat.