Send toughest Genitourinary spotters 20 images from textbook
Radiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here are 20 Toughest Genitourinary Radiology Spotters from Grainger & Allison's Diagnostic Radiology:
🫘 GENITOURINARY RADIOLOGY — 20 TOUGH SPOTTERS
1. Acute Pyelonephritis — MRI (T2W)
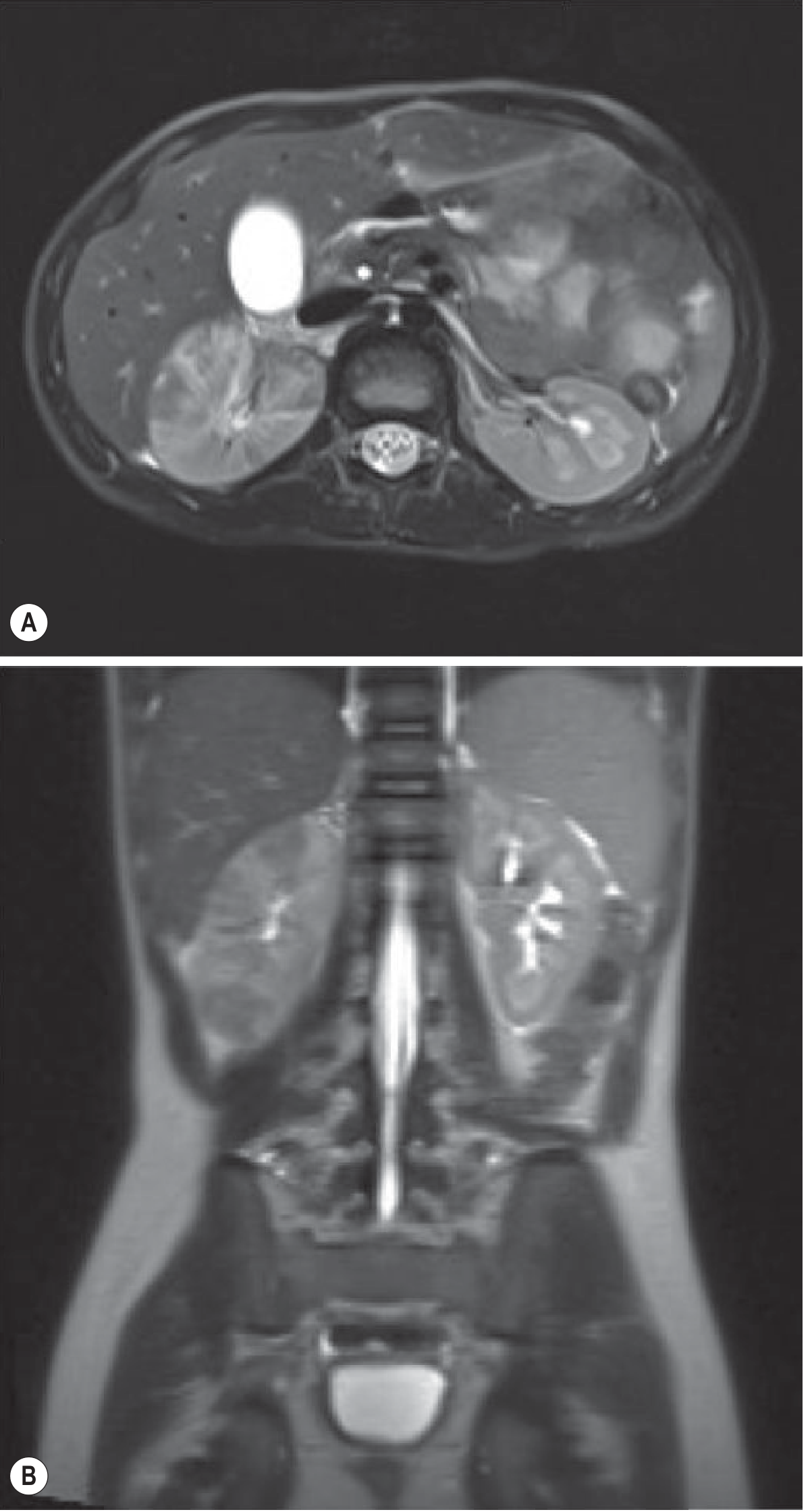
Fig. 26.20 — T2 weighted MRI showing striated signal in the right kidney with perinephric fluid.
Diagnosis: Acute Pyelonephritis
Key teaching: Striated nephrogram on MRI = wedge-shaped T2 hypointense areas radiating from medulla to cortex. Perinephric fluid indicates spread beyond capsule.
2. Acute Pyelonephritis in Transplanted Kidney — US + MRI + DWI
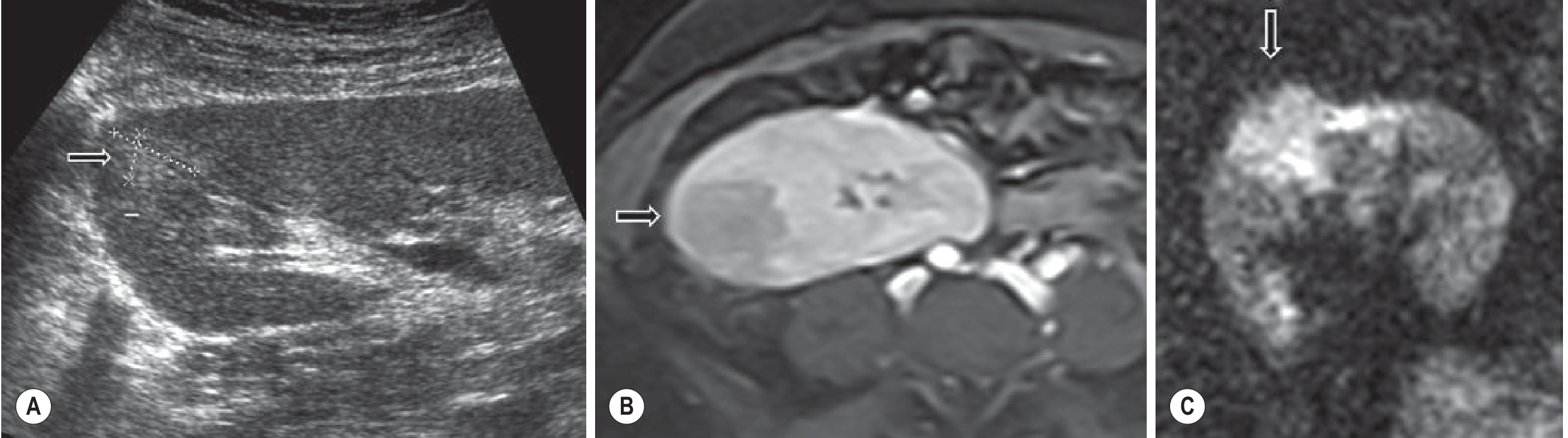
Fig. 26.21 — (A) Upper pole hyperechoic lesion on US; (B) Hypoenhancing on post-contrast T1W MRI; (C) Diffusion restriction on DWI (b=800).
Diagnosis: Acute Pyelonephritis in Transplant Kidney
Key teaching: DWI (high b-value >600) is highly sensitive — restricted diffusion distinguishes APN from ischaemia and tumour only with clinical correlation.
3. Renal Tuberculosis — CT

Fig. 26.27 — Calcification and parenchymal destruction in renal TB.
Diagnosis: Renal Tuberculosis
Key teaching: Autonephrectomy = complete replacement of renal parenchyma by calcification. Three or more of: pelvicalyceal thickening, ulceration, fibrosis/stricture → highly suggestive of TB. "Phantom calyx" = infundibular stricture obstructing a renal segment.
4. Bosniak Class II Renal Cyst — CT

Fig. 29.1 — CT showing cyst with thin septa and thin mural calcification, no enhancement.
Diagnosis: Bosniak Class II Renal Cyst (benign)
Key teaching: Bosniak classification — Class I/II = benign, no follow-up. Class IIF = surveillance. Class III = indeterminate (biopsy/surgery). Class IV = malignant. The trap: hyperdense cysts (high HU on unenhanced CT) that don't enhance are still Bosniak II.
5. Bosniak Class III Indeterminate Cystic Renal Mass

Fig. 29.2 — Thickened irregular septa, mural nodular calcification with equivocal enhancement.
Diagnosis: Bosniak Class III — Indeterminate Cystic Mass
Key teaching: <50% are malignant, but surgical exploration or biopsy mandated. Significant inter-observer variation — this is the hardest Bosniak class to call.
6. Cystic Renal Cell Carcinoma — Bosniak IV

Fig. 29.3/29.4 — Cystic mass with solid enhancing nodule.
Diagnosis: Cystic Renal Cell Carcinoma (Bosniak IV)
Key teaching: Enhancement >20 HU post-contrast = malignancy. Solid enhancing nodule within a cyst = Bosniak IV = treat as RCC.
7. Papillary Renal Cell Carcinoma — CT (Pre & Post Contrast)
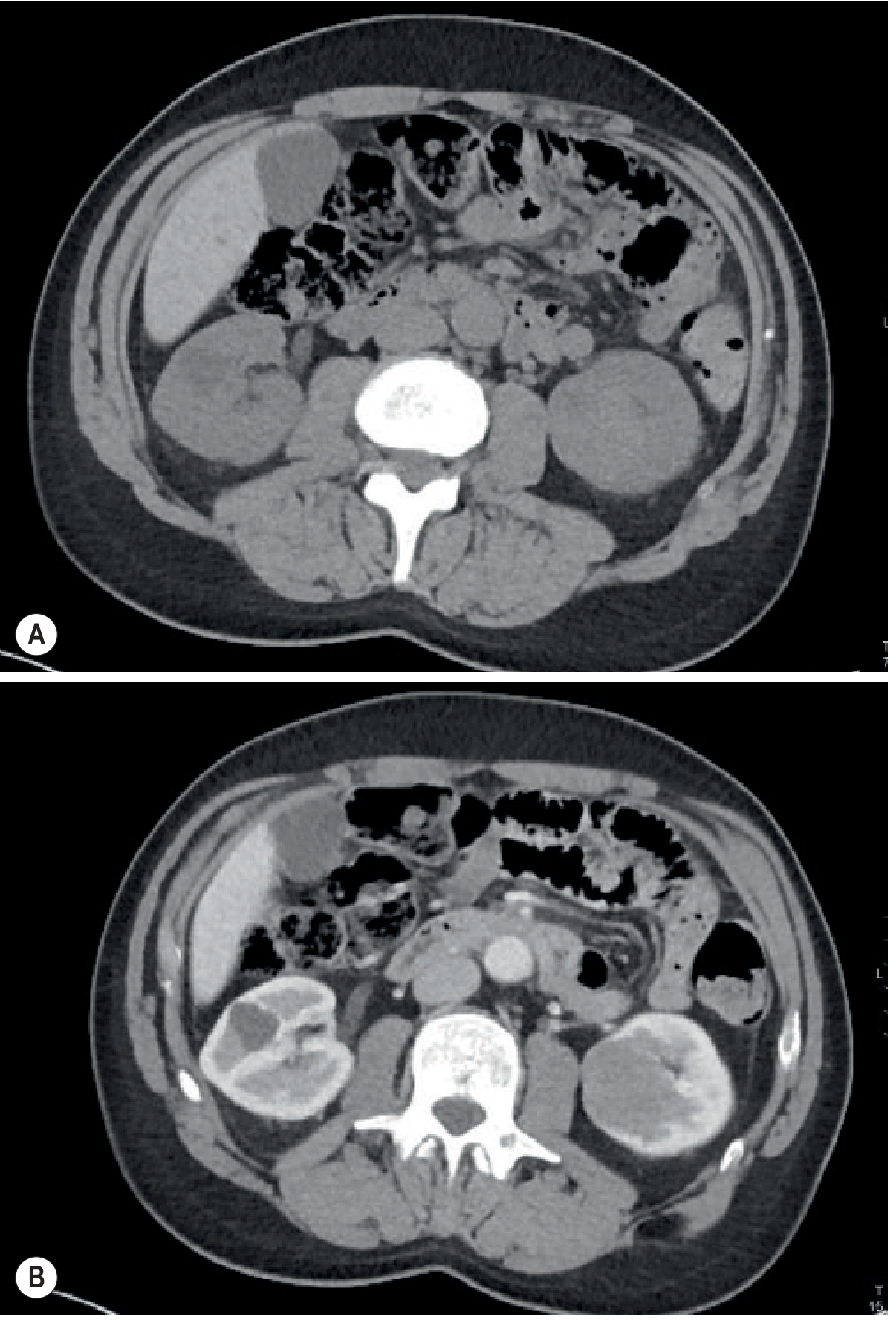
Fig. 29.14 — Pre- and post-contrast CT: large solid left renal mass with characteristically low-level enhancement. Right kidney shows a simple cyst for comparison.
Diagnosis: Papillary Renal Cell Carcinoma
Key teaching: The trap — papillary RCC shows minimal enhancement, easily mistaken for a hyperdense cyst. Always compare pre- and post-contrast HU values. Papillary RCC = homogeneous, hypovascular, often multiple.
8. Medullary Renal Cell Carcinoma — CT
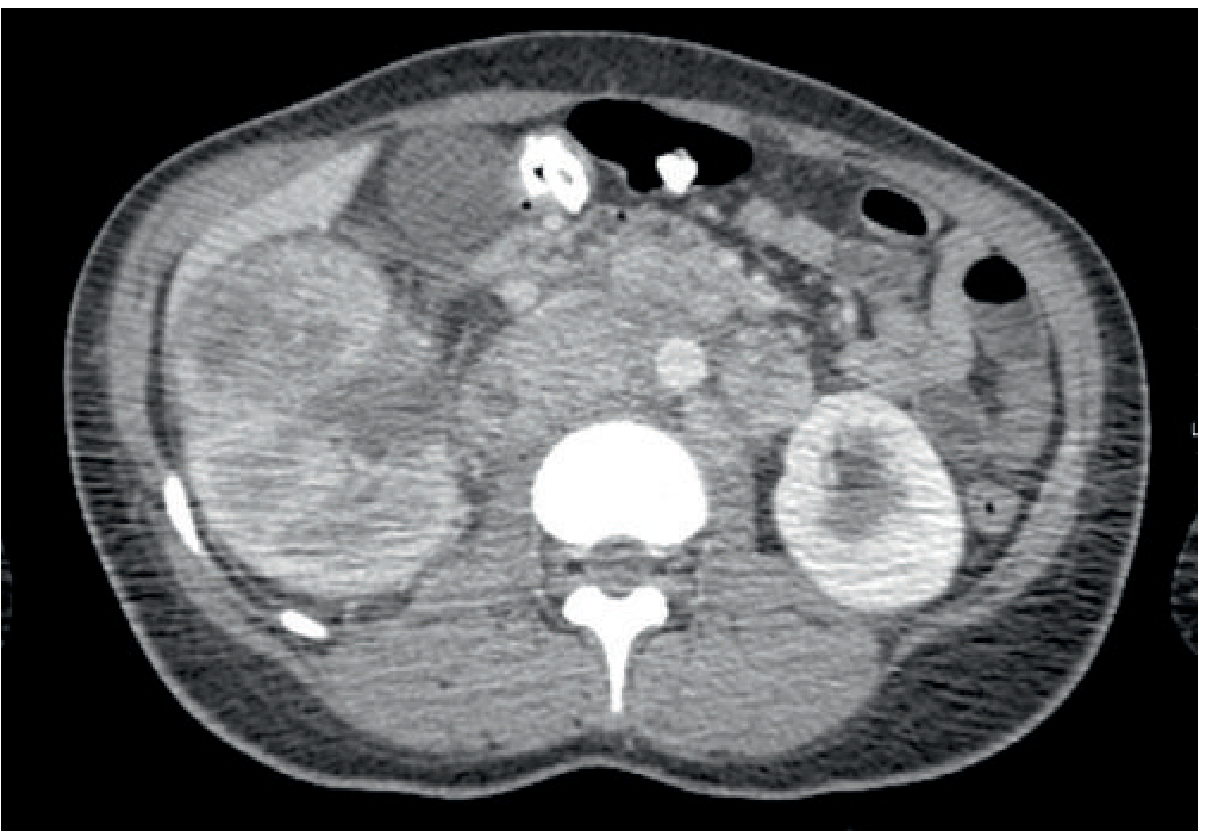
Fig. 29.15 — Post-contrast CT showing medullary carcinoma.
Diagnosis: Medullary Renal Carcinoma
Key teaching: Almost exclusively in sickle cell disease or trait. Arises from collecting duct epithelium, medullary location, usually metastatic at diagnosis. Young patient + sickle cell + infiltrating renal mass = medullary carcinoma until proven otherwise.
9. Renal Angiomyolipoma — CT (Macroscopic Fat)

Fig. 29.8 — CT demonstrating a mass with macroscopic fat (-20 to -80 HU) within the kidney.
Diagnosis: Renal Angiomyolipoma (AML)
Key teaching: Macroscopic fat on CT = AML (virtually pathognomonic). Beware fat-poor AML — may mimic RCC, requiring biopsy. AML >4 cm at risk of spontaneous haemorrhage (Wunderlich syndrome). Multiple bilateral AML = tuberous sclerosis.
10. Renal Oncocytoma — CT (Central Scar)

Fig. 29.12 — Homogeneously enhancing renal mass with central stellate scar.
Diagnosis: Renal Oncocytoma (benign)
Key teaching: Central scar is characteristic but NOT pathognomonic (also seen in chromophobe RCC). Cannot be reliably distinguished from RCC by imaging alone — biopsy required. Spoke-wheel vascularity on angiography is classic.
11. Autosomal Dominant Polycystic Kidney Disease (ADPKD) — CT

Fig. 25.49/25.50 — CT showing massively enlarged kidneys with innumerable cysts of varying sizes and densities (some haemorrhagic = high HU).
Diagnosis: ADPKD
Key teaching: Haemorrhagic cysts appear hyperdense on unenhanced CT — do not confuse with enhancing solid masses. Hepatic cysts in 80%. Pancreatic cysts in 10%. Increased risk of RCC. Associated with Berry aneurysms.
12. Transitional Cell Carcinoma — IVU/CT Urography (Filling Defect)

Fig. 31.2 — Irregular filling defect in the renal pelvis/ureter on CT urography.
Diagnosis: Transitional Cell Carcinoma (Urothelial Carcinoma)
Key teaching: "Goblet sign" = TCC at pelviureteric junction. Synchronous/metachronous lesions in 30–40% (field defect). CT urography = investigation of choice for haematuria evaluation.
13. Renal Calculi — Non-Contrast CT KUB

Fig. 32.1 — Non-contrast CT showing hyperdense calculi in the renal collecting system and ureter.
Diagnosis: Urolithiasis / Renal Calculi
Key teaching: NCCT = gold standard (sensitivity 96%, specificity 99%). All stones except pure uric acid are hyperdense. Uric acid stones = radiolucent on plain film but visible on CT. Staghorn = struvite (infection stones).
14. Renal Transplant Lymphocele — Ultrasound
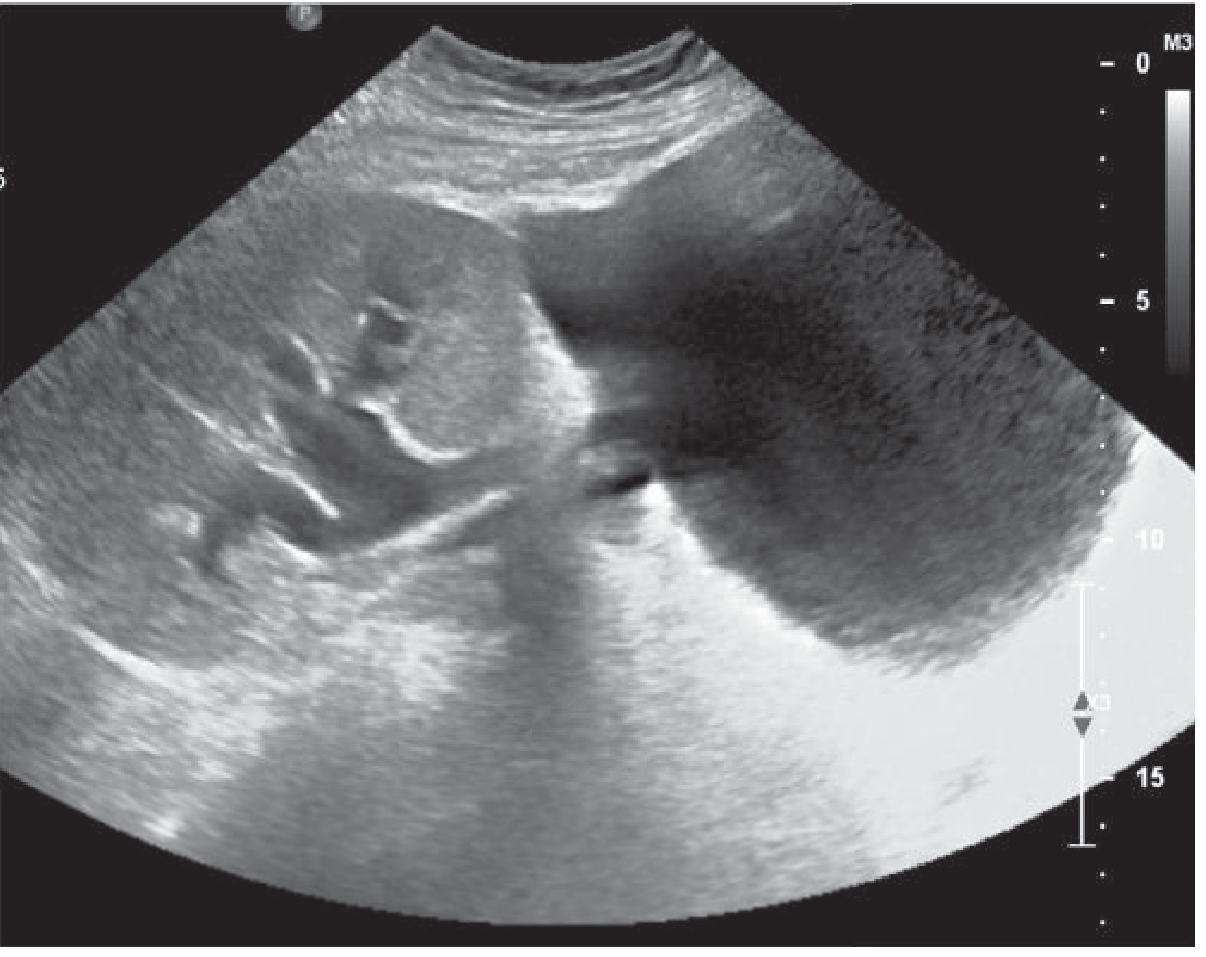
Fig. 30.19 — US: large hypoechoic fluid collection medial to the transplant kidney causing hydronephrosis.
Diagnosis: Post-Transplant Lymphocele
Key teaching: Commonest pelvic collection post-transplant (0.6–18%). Anechoic/hypoechoic with possible septations, medial to kidney. Distinguished from urinoma by aspiration fluid creatinine. Treat by sclerotherapy or surgical marsupialisation.
15. Post-Transplant Hydronephrosis — Ultrasound

Fig. 30.20 — US: hydronephrotic transplant kidney with dilated calyces.
Diagnosis: Transplant Ureteric Obstruction
Key teaching: Always scan pre- AND post-micturition — full bladder causes false-positive hydronephrosis. Causes: ureteric stricture (ischaemia of distal ureter), blood clot, fungal ball, lymphocele compression, stone. Rise in creatinine + hydronephrosis = nephrostomy + nephrostogram.
16. Post-Transplant Urinoma — CT
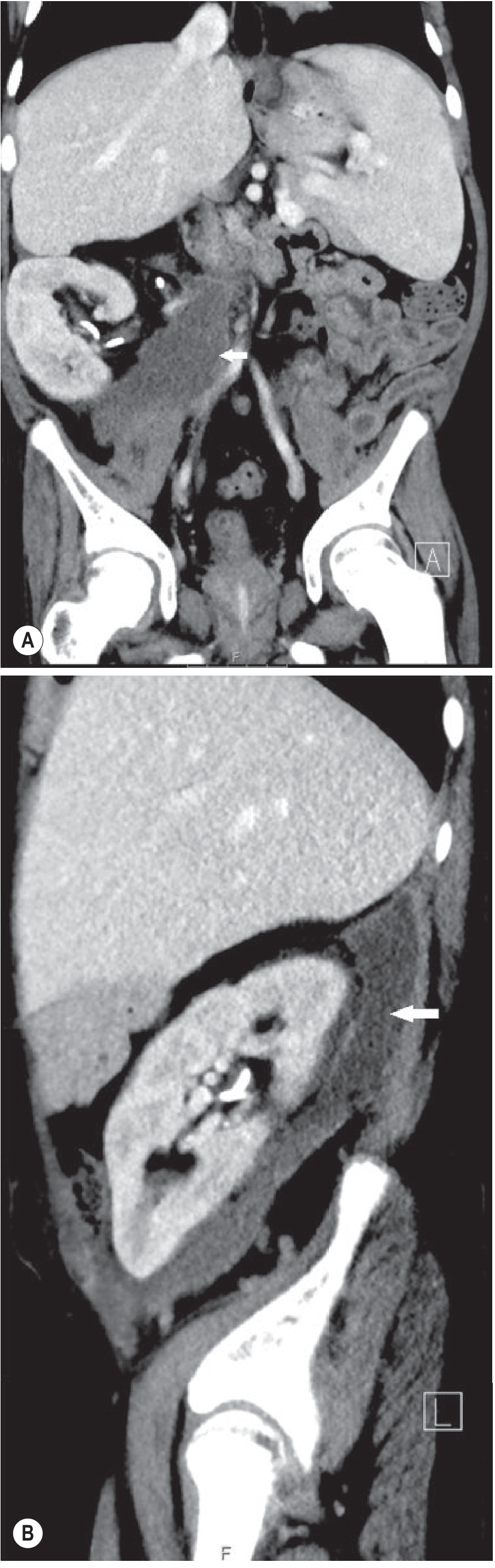
Fig. 30.18 — CT (coronal + sagittal): fluid collection at transplant-to-native ureter anastomosis site.
Diagnosis: Post-Transplant Urinoma
Key teaching: Urinoma creatinine >> serum creatinine (diagnostic). Occurs at uretero-vesical anastomosis. Distinguish from lymphocele (aspiration creatinine) and haematoma (echogenic on US, +HU on CT).
17. Renal Vein Thrombosis in Transplant — Doppler US
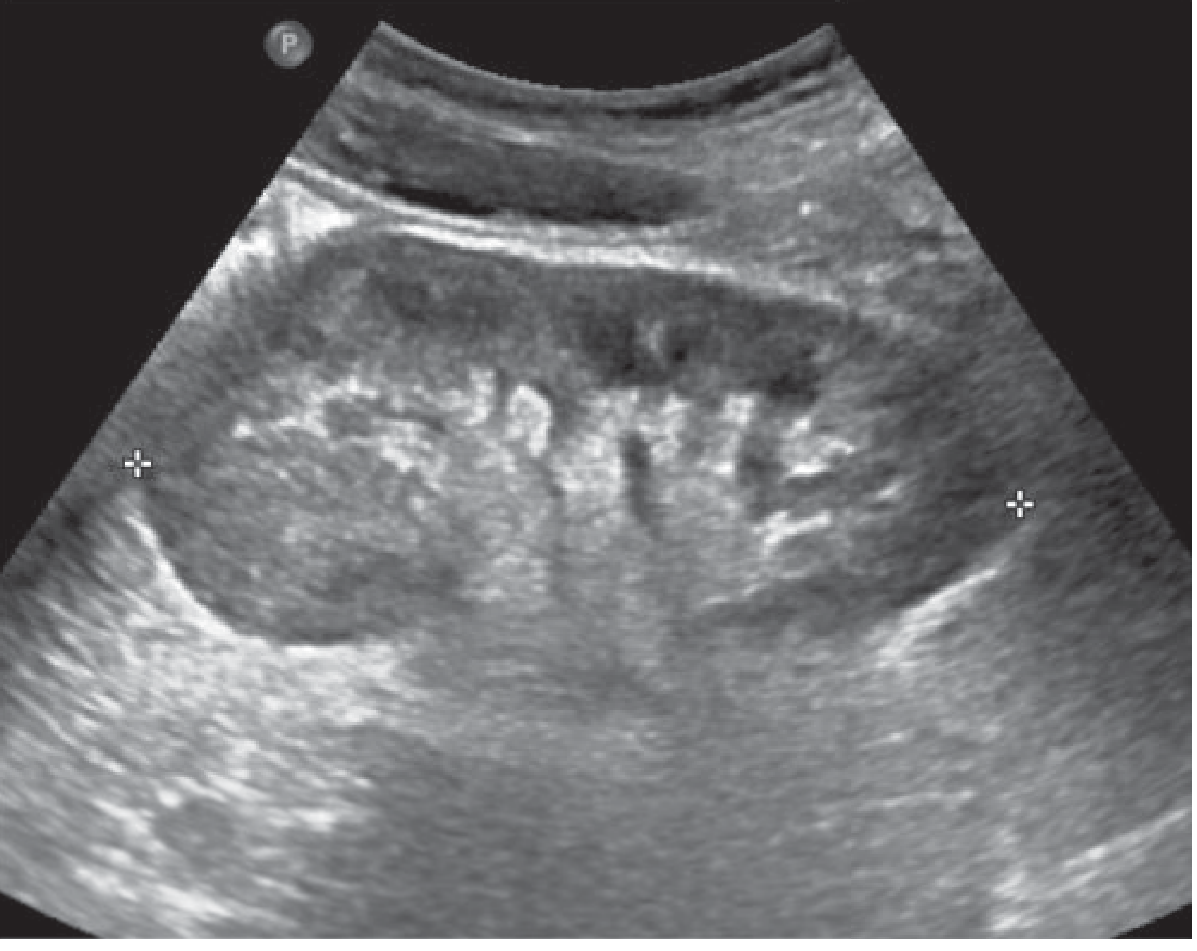
Fig. 30.2 — Doppler US: reversal of diastolic flow in transplant kidney.
Diagnosis: Renal Vein Thrombosis (Post-Transplant)
Key teaching: Reversed diastolic flow on Doppler = RVT or severe acute rejection. Absent diastolic flow = raised renal vascular resistance (ATN, rejection, obstruction). Resistive Index (RI) >0.8 is abnormal but non-specific.
18. Acquired Cystic Kidney Disease (ACKD) with RCC — CT
Diagnosis: ACKD complicated by Renal Cell Carcinoma
Key teaching: ACKD occurs in >90% of patients on dialysis for >5 years. Small/normal-sized kidneys + numerous cysts on a background of renal failure. Increased incidence of RCC (including low-grade papillary). Persists post-transplant. Trap: do not dismiss enhancing nodule as a simple cyst in dialysis patients.
19. Alkaline-Encrusted Pyelitis/Cystitis — CT
Diagnosis: Alkaline-Encrusted Pyelitis
Key teaching: Linear hyperdense calcifications along thickened urothelium on unenhanced CT. Caused by gram-positive urea-splitting organisms. Rare, severe form of chronic UTI. Easily missed on contrast-enhanced CT — always review unenhanced series.
20. Renal Artery Stenosis — Parvus Tardus Waveform on Doppler
Diagnosis: Haemodynamically Significant Renal Artery Stenosis
Key teaching: Parvus tardus = small amplitude + delayed systolic upstroke on Doppler. RI difference >0.05 between kidneys helps identify the stenotic side. Responsible for 14% of renal failure in patients >50 years. Confirm with CT or MR angiography. One of the few treatable causes of chronic renal failure.
📋 Quick Reference Summary Table
| # | Diagnosis | Modality | Key Finding |
|---|---|---|---|
| 1 | Acute Pyelonephritis | MRI T2W | Striated nephrogram, perinephric fluid |
| 2 | APN Transplant | US/DWI | DWI restriction, hypoenhancing lesion |
| 3 | Renal TB | CT | Autonephrectomy, phantom calyx |
| 4 | Bosniak II Cyst | CT | Thin septa, no enhancement |
| 5 | Bosniak III | CT | Thick septa, equivocal enhancement |
| 6 | Cystic RCC (Bosniak IV) | CT | Enhancing solid nodule in cyst |
| 7 | Papillary RCC | CT | Minimal enhancement (trap for cyst) |
| 8 | Medullary RCC | CT | Sickle cell + medullary infiltration |
| 9 | Angiomyolipoma | CT | Macroscopic fat (-20 to -80 HU) |
| 10 | Oncocytoma | CT | Central stellate scar (non-pathognomonic) |
| 11 | ADPKD | CT | Bilateral massive cystic kidneys |
| 12 | TCC/Urothelial Ca | CTU | Filling defect, goblet sign |
| 13 | Urolithiasis | NCCT | Hyperdense calculi (uric acid = CT visible) |
| 14 | Lymphocele | US | Medial hypoechoic collection post-transplant |
| 15 | Transplant Hydronephrosis | US | Post-void to exclude bladder cause |
| 16 | Urinoma | CT | Anastomotic fluid (high creatinine) |
| 17 | Renal Vein Thrombosis | Doppler | Reversed diastolic flow |
| 18 | ACKD + RCC | CT | Enhancing nodule in dialysis patient |
| 19 | Alkaline-encrusted pyelitis | NCCT | Linear urothelial calcification |
| 20 | Renal Artery Stenosis | Doppler | Parvus tardus waveform, RI asymmetry |
Source: Grainger & Allison's Diagnostic Radiology (Grainger & Allison's), Chapters 26–32.
This is a shared conversation. Sign in to Orris to start your own chat.