What are hypnozoites
Reading File
Searching the Web
hypnozoites malaria Plasmodium vivax dormant liver stage
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough answer drawn from multiple medical textbooks.
Hypnozoites
What They Are
Hypnozoites (from Greek hypnos = sleep) are dormant, metabolically inactive liver-stage forms of certain Plasmodium malaria parasites. They sit quiescently inside hepatocytes without dividing, essentially "sleeping," for weeks, months, or even years after the initial mosquito bite. Only P. vivax and P. ovale form hypnozoites; P. falciparum and P. malariae do not.
How They Form - The Lifecycle
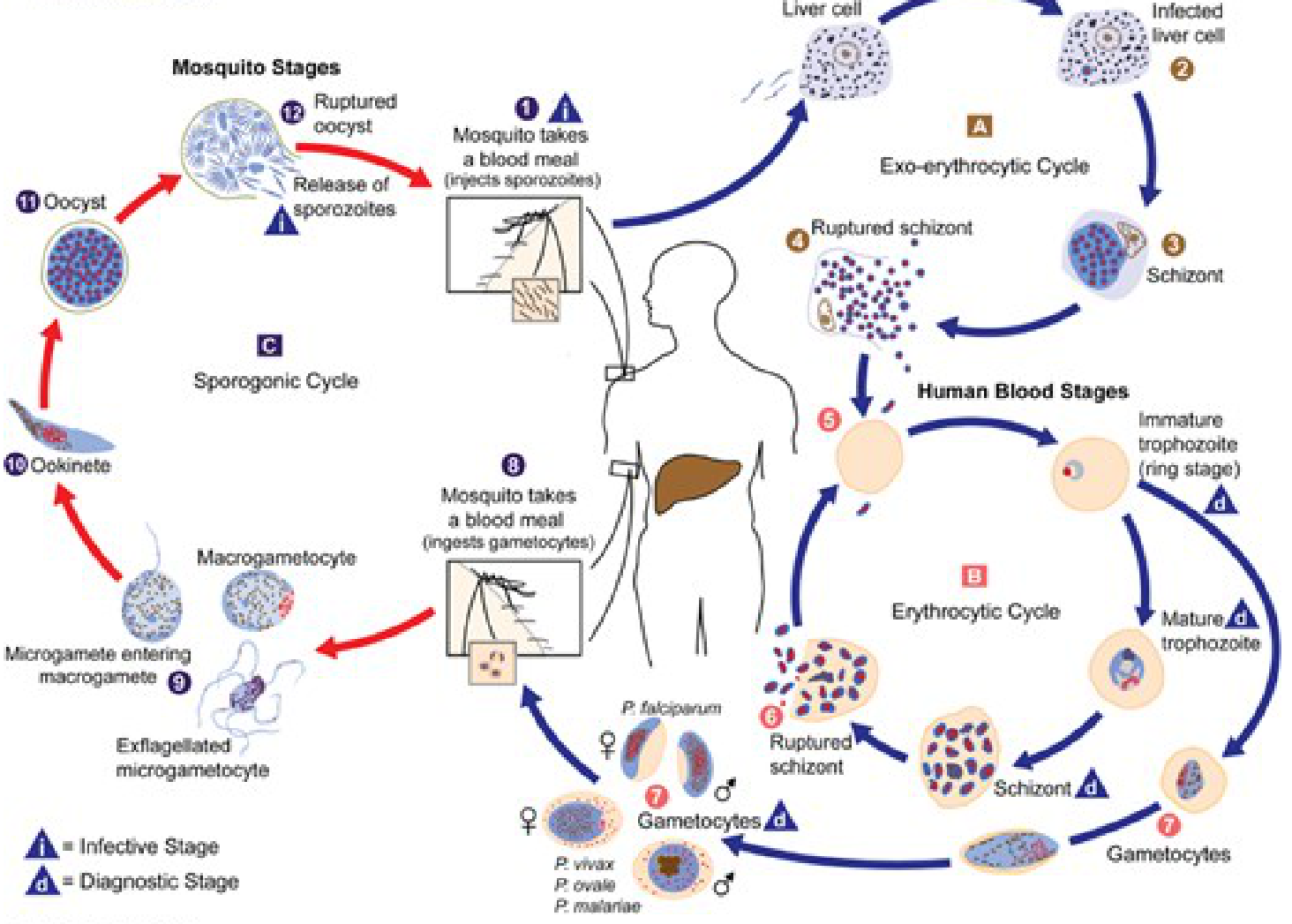
When an infected Anopheles mosquito bites a human, it injects sporozoites into the bloodstream. These travel to the liver and invade hepatocytes. In P. falciparum and P. malariae, all sporozoites proceed directly to replicate as liver schizonts, which rupture within 2-10 days and release merozoites into the blood. In P. vivax and P. ovale, some sporozoites instead arrest their development and become hypnozoites rather than immediately developing into schizonts.
What Makes Them Clinically Important
Because hypnozoites are metabolically quiescent, they are not killed by standard blood-stage antimalarials (e.g., chloroquine, artemisinin-based therapies). When they eventually reactivate - triggered by mechanisms that are not fully understood but may include host immune changes or intercurrent illness - they resume development into schizonts, which then release merozoites into the bloodstream. This causes a relapse of malaria that is clinically indistinguishable from a new infection.
Key points (from Rosen's Emergency Medicine):
"Hypnozoites are metabolically inactive and thus less susceptible to standard pharmacologic therapies. Hypnozoites can eventually release merozoites into the bloodstream weeks to months or even years after initial infection, initiating relapse in the host unless specific treatment for the hypnozoite stage was anticipated."
Relapse vs. Recrudescence
- Relapse (vivax/ovale): reactivation of a hypnozoite. The blood was previously cleared, but a dormant liver stage re-seeds it.
- Recrudescence (falciparum/malariae): blood-stage parasites were suppressed but never fully eradicated; they re-emerge from blood, not from a liver reservoir.
Treatment - Radical Cure
To achieve a radical cure (eliminating both the blood stage AND the liver stage), the drugs that specifically kill hypnozoites are the 8-aminoquinolines:
| Drug | Notes |
|---|---|
| Primaquine | Standard of care; 14-day course; contraindicated in G6PD deficiency and pregnancy |
| Tafenoquine | Newer single-dose alternative; also contraindicated in G6PD deficiency |
Standard blood schizonticides alone (chloroquine, ACTs) are insufficient - they clear the blood-stage infection but leave hypnozoites intact, allowing relapse.
From Katzung's Basic and Clinical Pharmacology:
"Standard chemoprophylaxis does not prevent a relapse of vivax or ovale malaria, because the hypnozoite forms of these parasites are not eradicated by available blood schizonticides."
Why Eradication Is Difficult
Hypnozoites are a major barrier to global malaria eradication because:
- They are tiny, dormant, and morphologically hard to distinguish from normal hepatocytes
- They cannot be detected with standard blood-film microscopy or RDTs (which only detect blood-stage parasites)
- The only drugs that kill them (8-aminoquinolines) require G6PD testing before use due to hemolytic risk
- The triggers for reactivation are still incompletely understood
Sources:
- Katzung's Basic and Clinical Pharmacology, 16th ed., PARASITE LIFE CYCLE & Antimalarial Action sections
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Chapter 122
- Lippincott Illustrated Reviews: Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.