Bronchopulmonary segments. Anaesthetic significance. Positions for postural drainage and their significance in pre and post operative care
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Searching the Web
bronchopulmonary segments anaesthetic significance postural drainage preoperative postoperative care
Reading Web Page
https://www.kenhub.com/en/library/anatomy/bronchopulmonary-s…
Loading Image
I now have comprehensive information to write a thorough answer. Let me compile everything.
Bronchopulmonary Segments: Anatomy, Anaesthetic Significance, and Postural Drainage
1. Definition and Structure
A bronchopulmonary segment is the area of lung supplied by a single segmental bronchus together with its accompanying branch of the pulmonary artery. Each segment forms a three-dimensional wedge- or pyramid-shaped unit, with its apex directed toward the hilum and its base projected onto the pleural surface of the lung.
Key structural features:
- The segmental bronchus and pulmonary artery branch run intrasegmentally (centrally within the segment)
- Pulmonary vein tributaries run intersegmentally — passing between segments through connective tissue septa, draining adjacent segments
- Segments are separated by connective tissue septa (subpleural in origin), making each segment a functionally independent unit
- Each segment is the smallest unit of lung that can be surgically resected without compromising adjacent regions
(Gray's Anatomy for Students, p. 210; Color Atlas of Human Anatomy Vol. 2, p. 214)
2. Number and Nomenclature of Segments
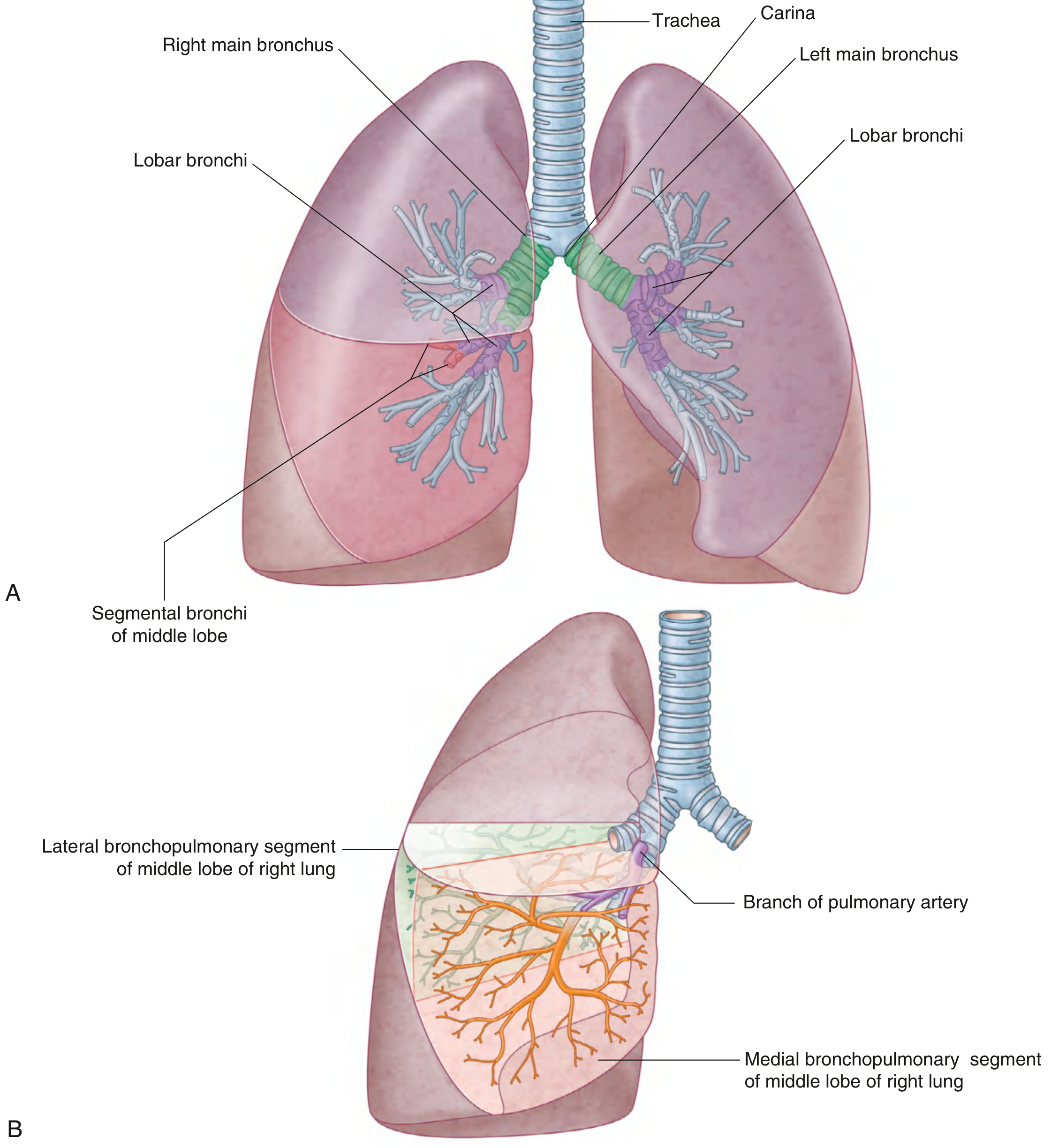
Fig. Bronchial tree (A) and bronchopulmonary segments of the right and left lungs (B). — Gray's Anatomy for Students, p. 209–210
Right Lung — 10 segments:
| Lobe | Segment | Number |
|---|---|---|
| Superior lobe | Apical | S I |
| Posterior | S II | |
| Anterior | S III | |
| Middle lobe | Lateral | S IV |
| Medial | S V | |
| Inferior lobe | Superior (apical) | S VI |
| Medial basal (cardiac) | S VII | |
| Anterior basal | S VIII | |
| Lateral basal | S IX | |
| Posterior basal | S X |
Left Lung — 8–9 segments (some fused):
| Lobe | Segment | Number |
|---|---|---|
| Superior lobe | Apicoposterior (S I + II fused) | S I+II |
| Anterior | S III | |
| Superior lingular | S IV | |
| Inferior lingular | S V | |
| Inferior lobe | Superior | S VI |
| Medial basal | S VII | |
| Anterior basal | S VIII | |
| Lateral basal | S IX | |
| Posterior basal | S X |
On the left, segments S I and S II are fused into the apicoposterior segment, and S VII (medial basal) may be absent or fused — giving 8 or 9 functional segments.
(Color Atlas of Human Anatomy Vol. 2, p. 214–215)
3. Bronchopulmonary Segments — Detailed View
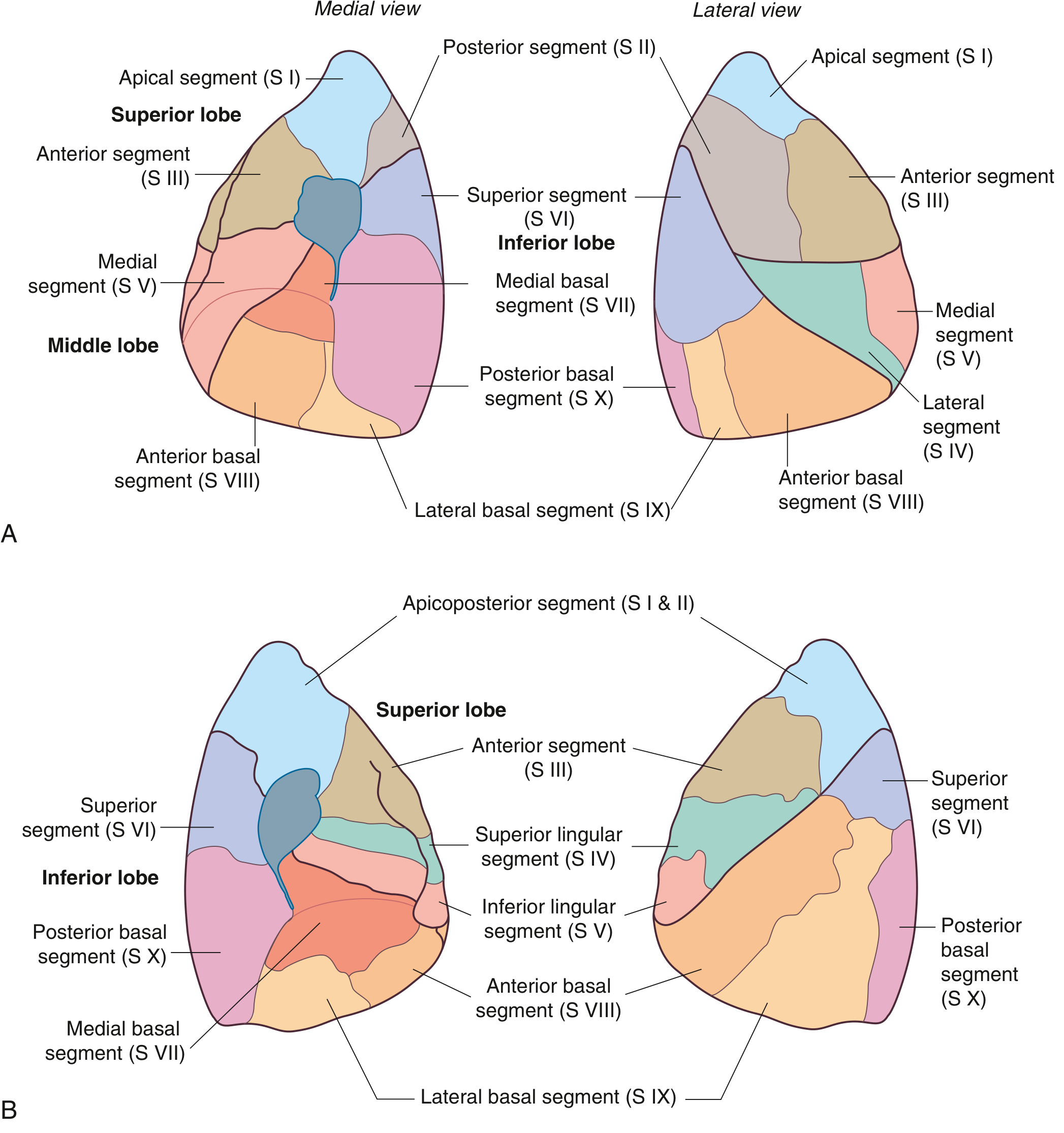
Fig. Bronchopulmonary segments — Right lung (A, above) and Left lung (B, below) in medial and lateral views. — Gray's Anatomy for Students, p. 211
4. Anaesthetic Significance
A. Lung Isolation and One-Lung Ventilation (OLV)
The knowledge of segmental bronchial anatomy is fundamental for:
- Double-lumen endotracheal tube (DLT) placement — the left DLT is positioned so the bronchial lumen sits in the left main bronchus proximal to the left upper lobe bronchus, exploiting the longer left main bronchus (~5 cm) versus the right (~2 cm). The anatomy of the right upper lobe bronchus (arising ~1–2.5 cm from the carina) necessitates a specially designed right-sided DLT with a Murphy eye.
- Bronchial blocker placement — fibreoptic-guided blockers are advanced into specific lobar or segmental bronchi; knowledge of the segmental map is essential for accurate positioning.
- OLV allows operative access for thoracic surgery (lobectomy, pneumonectomy, oesophagectomy, thoracoscopic procedures) by collapsing the operative lung.
B. Aspiration and Dependent Segment Contamination
- The right main bronchus is wider (12–16 mm) and makes a more acute angle with the trachea (~25°), compared to the left (~45°) — making the right lower lobe (especially posterior basal and superior segments) the most common site of aspiration pneumonia in both supine and upright patients.
- During anaesthesia with vomiting or regurgitation, contents tend to enter the posterior basal segments of the lower lobes and the superior segments (S VI) in the supine patient.
- This has implications for patient positioning during induction (head-up/lateral) and for postoperative physiotherapy targeting these segments.
C. Segmental Resection (Segmentectomy)
- Because each bronchopulmonary segment is a functionally independent bronchoarterial unit, surgeons can perform anatomic segmentectomy — a lung-sparing procedure — preserving adjacent segments.
- Pre-operative lung function prediction uses the formula:
Predicted post-operative FEV₁ = Pre-operative FEV₁ × (segments remaining ÷ total segments)
- Total = 19 (10 right + 9 left) or 18, depending on nomenclature used
- This guides anaesthetic and surgical risk stratification
D. Fibreoptic Bronchoscopy and Airway Management
- Segmental bronchial anatomy guides bronchoscopic inspection, selective BAL, endobronchial biopsy, and foreign body removal.
- Rigid bronchoscopy under general anaesthesia allows retrieval from the right lower lobe bronchi and basal segments, which are the commonest sites of foreign body lodgement.
E. Endobronchial Spread of Disease and Isolation
- In patients with lung abscess, bronchiectasis, tuberculosis, or massive haemoptysis, the anaesthetist must protect the healthy lung from spillover using OLV. The diseased segment must be identified preoperatively and the double-lumen tube or blocker positioned accordingly.
F. Selective Bronchography / CT Bronchography
- Segmental anatomy underpins CT-guided localisation for video-assisted thoracoscopic surgery (VATS), where small peripheral nodules are identified by their segment for preoperative wire/dye marking.
5. Postural Drainage
Definition
Postural drainage is the positioning of the patient such that gravity facilitates drainage of secretions from a specific bronchopulmonary segment into the larger central airways, from where they can be expectorated or suctioned. It is frequently combined with chest percussion (rhythmic cupped-hand clapping to loosen mucus from airway walls) — together called Chest Physiotherapy (CPT) or "Pulmonary Toilet."
Each position should be maintained for 3–15 minutes. A foot-end elevation of 14–18 inches (35–45 cm) is required for middle and lower lobe drainage.
Positions for Each Segment
| Segment | Position |
|---|---|
| Upper lobe — Apical (S I) | Sitting upright, leaning slightly backward (~30°). Percussion over trapezius between clavicle and scapula. |
| Upper lobe — Anterior (S III) | Supine, bed flat, pillow under knees. Percussion over pectoralis muscle. |
| Upper lobe — Posterior (S II) | Sitting, leaning forward ~30° over a pillow; or prone with pillow under abdomen. Percussion over upper back. |
| Left upper — Apicoposterior (S I+II) | Sitting, leaning forward and towards the left side. |
| Middle lobe — Lateral (S IV) & Medial (S V) | Left lateral (quarter-turn from supine), foot of bed raised 14–18 inches. Percussion over right nipple area. |
| Lingula — Superior (S IV) & Inferior (S V) | Right lateral decubitus, foot of bed raised 14–18 inches. Percussion over left nipple area. |
| Inferior lobe — Superior/Apical (S VI) | Prone, pillow under abdomen, bed flat. Percussion over middle of back below scapulae. |
| Inferior lobe — Anterior basal (S VIII) | Supine, knees flexed, foot of bed raised 18–20 inches. Percussion over lower anterior ribs. |
| Inferior lobe — Lateral basal (S IX) | Lateral decubitus (affected side up), foot raised 18–20 inches. Percussion over lateral lower ribs. |
| Inferior lobe — Posterior basal (S X) | Prone, pillow under hips/pelvis, foot raised 18–20 inches. Percussion over lower posterior ribs. |
| Inferior lobe — Medial basal/Cardiac (S VII) | Right lateral (left lung) or semi-prone position; foot raised; 20° tilt. |
(Physiopedia — Postural Drainage; AARC Clinical Practice Guideline)
6. Significance in Pre- and Postoperative Care
Preoperative Significance
| Goal | Rationale |
|---|---|
| Reduce secretion load | Patients with COPD, bronchiectasis, or productive cough have excessive retained secretions. Preoperative CPT reduces the bacterial load and volume of secretions, decreasing risk of postoperative pneumonia and atelectasis. |
| Optimise lung function (FEV₁/FVC) | Clearing secretions improves airway patency and spirometry values, better preparing the patient for surgery and anaesthesia. |
| Identify affected segments | The physiotherapist's response to positional drainage helps clinch which segments are affected — useful for surgical planning. |
| Training the patient | Teaching the patient preoperatively to perform breathing exercises and effective coughing ensures they can cooperate postoperatively when pain limits effort. |
| Reduce aspiration risk | In patients with full stomachs or oesophageal disease, identifying dependent segments at risk guides positioning at induction. |
Postoperative Significance
| Goal | Rationale |
|---|---|
| Prevent/treat atelectasis | General anaesthesia, supine positioning, and reduced tidal volumes cause small airway closure and microatelectasis — especially in dependent lower lobe segments (S VIII–X). Postural drainage + deep breathing reverses this. |
| Prevent postoperative pneumonia | Retained secretions in basal segments become colonised. CPT clears them before infection is established. ~30–40% of patients undergoing pulmonary resection experience a postoperative complication; secretion clearance is a primary preventive measure. (Murray & Nadel, Fishman's Pulmonary Diseases) |
| After thoracic surgery | Patients post-lobectomy or segmentectomy have reduced respiratory reserve. CPT for the remaining segments is critical to maintain gas exchange. |
| After abdominal and cardiac surgery | Diaphragmatic splinting from pain reduces basal ventilation; postural drainage of S VI (superior basal) and basal segments (S VIII–X) is standard. |
| In ICU/ventilated patients | Frequent position changes, prone positioning, and modified postural drainage are used to drain specific segments in ventilator-associated pneumonia prevention. Spinal cord injury patients, who cannot cough effectively, rely heavily on assisted postural drainage and mechanical cough assistance. (Murray & Nadel, p. 3012–3015) |
| Contraindications post-surgery | Head-down (Trendelenburg) positions are avoided after: recent thoracic/abdominal surgery, raised ICP, haemodynamic instability, uncontrolled haemoptysis, recent oesophageal anastomosis, and pneumothorax. Modified positions (not full Trendelenburg) are used instead. (StatPearls — Postural Drainage, NBK604210) |
7. Summary Table: Segments → Drainage Positions → Clinical Relevance
| Segment | Drainage Position | Anaesthetic / Surgical Relevance |
|---|---|---|
| Apical (S I) | Sitting upright | Commonest site of TB reactivation; aspiration in semi-recumbent |
| Posterior (S II) / Apicoposterior | Leaning forward | Posterior aspiration in obtunded patients |
| Anterior (S III) | Supine, flat | General atelectasis post-anaesthesia |
| Lingula (S IV, V) | Right lateral, foot up | Left-sided aspiration equivalent to middle lobe |
| Middle lobe (S IV, V) | Left lateral, foot up | Middle lobe syndrome; atelectasis from long surgery |
| Superior basal (S VI) | Prone, flat | Commonest postoperative atelectasis in supine patients; aspiration in prone/supine |
| Posterior basal (S X) | Prone, foot up | Commonest aspiration site; lowest dependent segment |
| Anterior/lateral basal (S VIII, IX) | Supine/lateral, foot up | Postoperative consolidation after abdominal surgery |
References
- Gray's Anatomy for Students, pp. 208–211 (Bronchopulmonary segments)
- Color Atlas of Human Anatomy, Vol. 2: Internal Organs, pp. 214–216 (Divisions of bronchi, segments)
- Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume (Spinal cord disease; postural drainage in ventilated patients)
- Fishman's Pulmonary Diseases and Disorders, 2-Volume (Postoperative pulmonary morbidity)
- StatPearls — Postural Drainage and Vibration (NCBI Bookshelf)
- AARC Clinical Practice Guideline — Postural Drainage Therapy
- Kenhub — Bronchopulmonary Segments
Anatomy of diaphragm. Anaesthetic significance. Functions in various phases of anaesthesia
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Searching the Web
diaphragm function during phases of anaesthesia induction maintenance emergence muscle relaxants FRC atelectasis
Reading Web Page
https://www.ijrc.in/abstractArticleContentBrowse/IJRC/31115/…
Loading Image
I now have comprehensive material from textbooks and clinical sources. Let me compile the full answer.
Anatomy of the Diaphragm, Anaesthetic Significance, and Functions in Various Phases of Anaesthesia
1. Anatomy of the Diaphragm
Overview
The diaphragm is a dome-shaped musculotendinous partition that separates the thoracic cavity from the abdominal cavity. It is the principal muscle of respiration, contributing approximately 70–80% of tidal volume during quiet breathing in the upright position.
(Gray's Anatomy for Students, p. 198; Morgan & Mikhail's Clinical Anesthesiology, p. 917)
Structure
The diaphragm consists of:
- A central tendinous portion — the central tendon, a trefoil-shaped fibrous aponeurosis into which all peripheral muscle fibers converge. The pericardium is directly attached to its middle part.
- A peripheral muscular portion — arranged circumferentially, arising from the margins of the inferior thoracic aperture.
The muscular fibers arise from three areas, producing three named parts:
- Sternal part: two small slips from the posterior surface of the xiphoid process
- Costal part: inner surfaces of the lower six costal cartilages and ribs (ribs 7–12) — the largest part
- Lumbar (vertebral) part: the crura and arcuate ligaments
Attachments
Anterior: xiphoid process of sternum
Lateral: inner surfaces of costal cartilages 7–10, ribs 11 and 12
Posterior (most extensive):
- Right crus — bodies of L1, L2, L3 and intervening discs (longest and broadest)
- Left crus — bodies of L1, L2 and intervening disc
- Crura blend with the anterior longitudinal ligament of the vertebral column
Arcuate ligaments (tendinous arches bridging posterior gaps):
- Median arcuate ligament — connects the two crura over the front of the aorta at T12
- Medial arcuate ligament (psoas arch) — from lateral body of L1/L2 to transverse process of L1, arching over psoas major
- Lateral arcuate ligament (quadratus arch) — from transverse process of L1 to rib XII, arching over quadratus lumborum
(Gray's Anatomy for Students, pp. 320, 432–433)
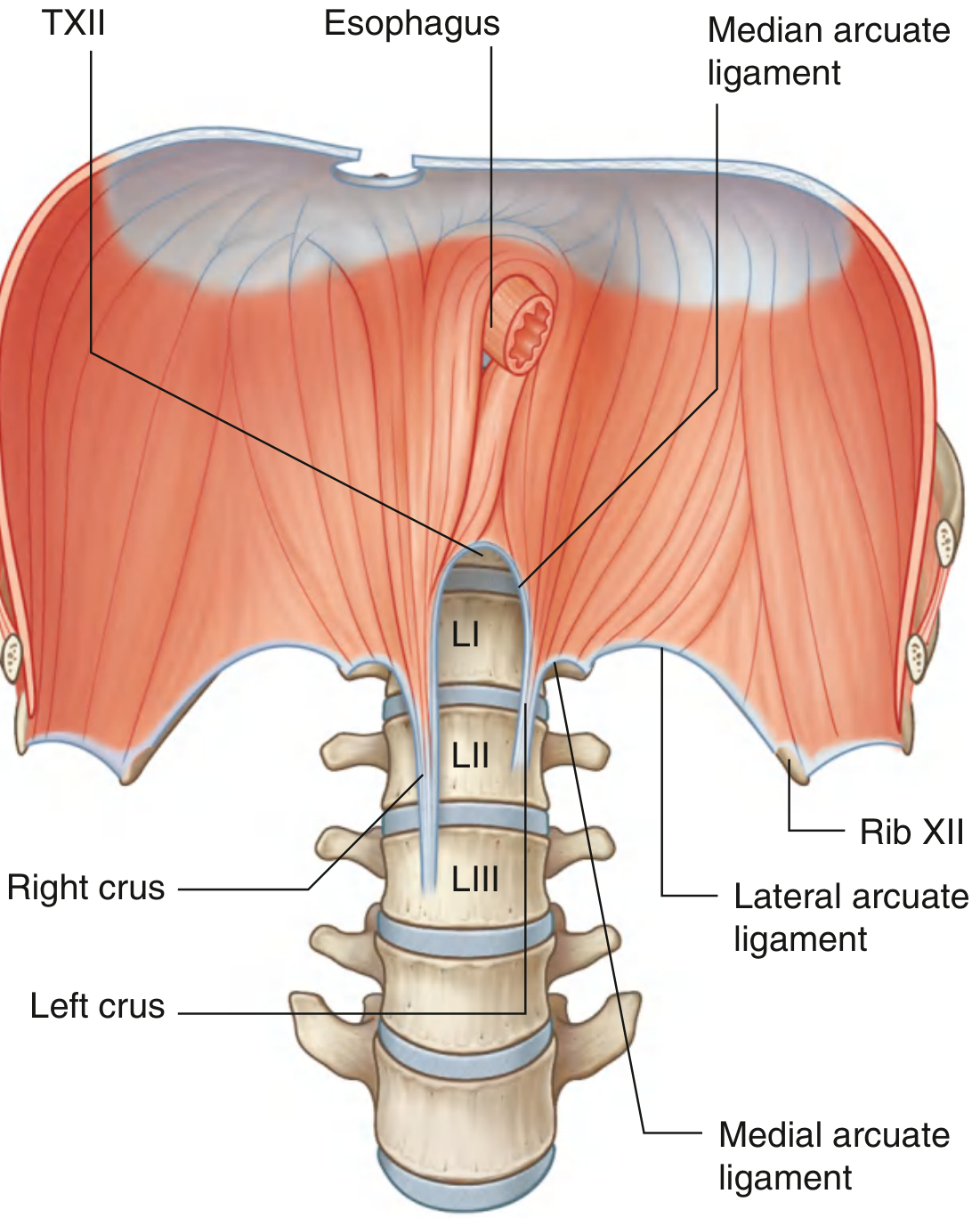
Fig. Crura of the diaphragm viewed from below, showing median, medial, and lateral arcuate ligaments. — Gray's Anatomy for Students
Openings in the Diaphragm
| Opening | Vertebral Level | Structure(s) Passing Through |
|---|---|---|
| Caval opening (in central tendon) | T8 | Inferior vena cava + right phrenic nerve |
| Oesophageal hiatus (in right crus, muscular) | T10 | Oesophagus + anterior & posterior vagal trunks + oesophageal branches of left gastric vessels + lymphatics |
| Aortic hiatus (between crura, behind median arcuate ligament) | T12 | Aorta + thoracic duct + (sometimes) azygos vein |
Additional transmissions:
- Greater, lesser, least splanchnic nerves — through the crura
- Hemiazygos vein — through left crus
- Left phrenic nerve — through muscular part of left dome
- Sympathetic trunks — behind medial arcuate ligaments
- Superior epigastric vessels — between sternal and costal slips (foramen of Morgagni)
(Gray's Anatomy for Students, pp. 198–199, 432–433)
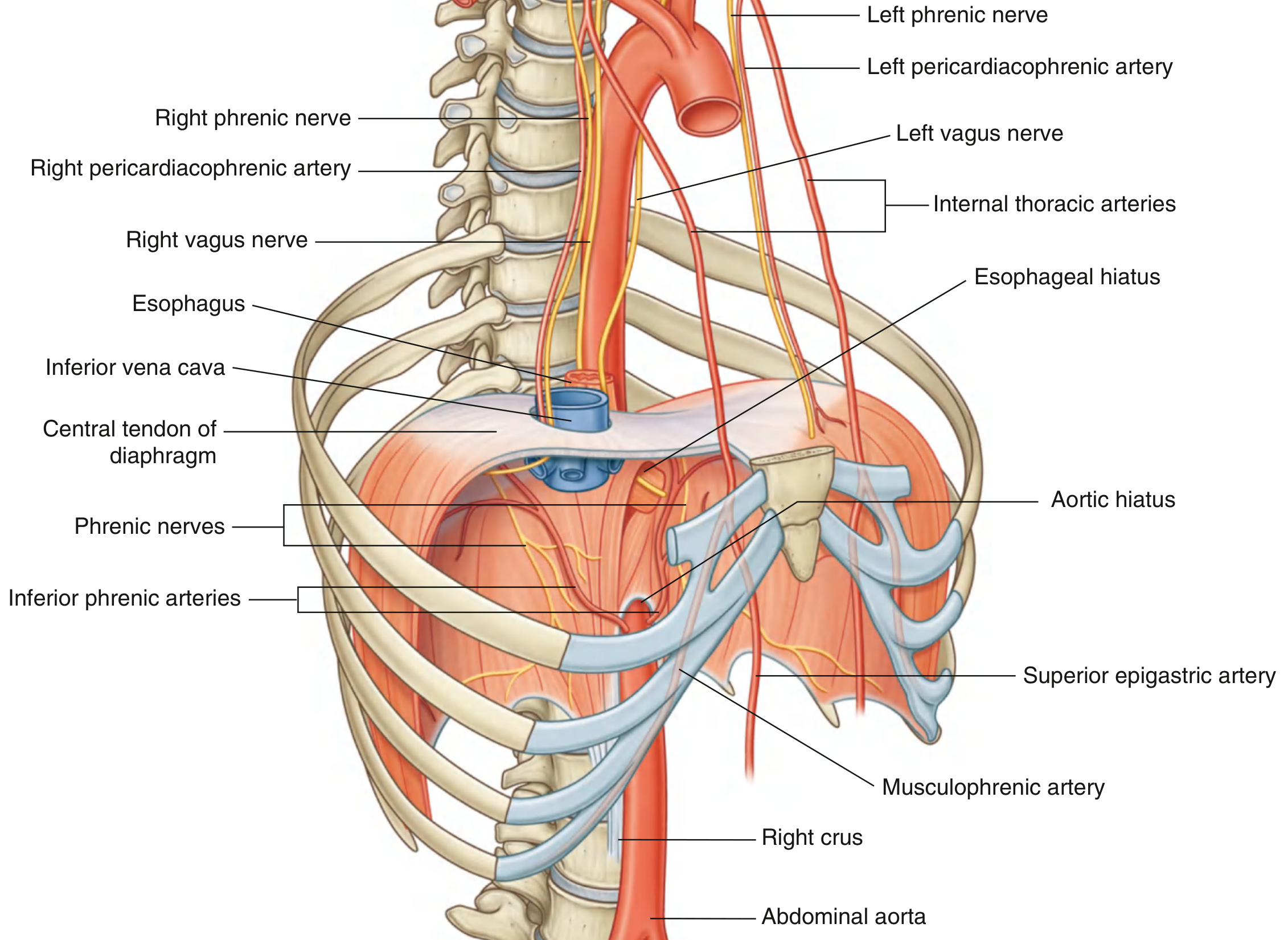
Fig. Posterior view of the diaphragm showing openings, neurovascular supply, and relations. — Gray's Anatomy for Students, p. 198
Blood Supply
From above (thoracic surface):
- Pericardiacophrenic arteries (branches of internal thoracic artery) — with phrenic nerves
- Musculophrenic arteries (terminal branches of internal thoracic artery)
- Superior phrenic arteries (from lower thoracic aorta)
- Small branches from lower intercostal arteries
From below (abdominal surface):
- Inferior phrenic arteries — the largest supply; direct branches of the abdominal aorta (or occasionally from the coeliac axis)
Venous drainage mirrors arterial supply — draining to brachiocephalic veins, azygos system, left suprarenal vein, and inferior vena cava.
(Gray's Anatomy for Students, p. 199)
Innervation
| Type | Source | Distribution |
|---|---|---|
| Motor (entire diaphragm) | Phrenic nerves (C3, C4, C5) | All muscular parts including crura |
| Sensory — central diaphragm | Phrenic nerves (C3–C5) | Central tendon and adjacent muscle |
| Sensory — peripheral diaphragm | Lower six intercostal nerves (T6–T11) | Peripheral muscular rim |
The phrenic nerves descend through the neck, pass through the superior thoracic aperture, and travel through the mediastinum anterior to the lung roots to reach the diaphragm. The right phrenic nerve passes through the caval opening; the left phrenic nerve pierces the muscular part of the left dome anterior to the central tendon.
Key principle: Spinal cord injury below C5 spares diaphragmatic function; injury at or above C3 abolishes it completely.
Unilateral phrenic nerve block/palsy reduces lung function indices by only ~25%; bilateral palsy is more severe but may still allow adequate ventilation via accessory muscles in some patients.
(Morgan & Mikhail's Clinical Anesthesiology, p. 788–789; Gray's Anatomy for Students, p. 173–174)
Domes (Cupulae)
At end of normal expiration in the upright position:
- Right dome: reaches rib V in the midclavicular line (elevated by the liver)
- Left dome: fifth intercostal space (pushed by stomach fundus and spleen)
The right dome is higher because the liver creates a larger, more even support beneath it. During inspiration, both domes descend 1.5–2 cm on quiet breathing; up to 10 cm with deep breathing.
2. Anaesthetic Significance
A. Phrenic Nerve — at Risk During Regional Procedures
| Procedure | Risk to Phrenic Nerve | Consequence |
|---|---|---|
| Interscalene brachial plexus block | ~100% incidence of ipsilateral phrenic palsy | 25% reduction in FEV₁/FVC; dangerous in patients with contralateral phrenic dysfunction or severe respiratory disease |
| Supraclavicular brachial plexus block | 50–70% ipsilateral phrenic palsy | Same as above |
| Infraclavicular / axillary blocks | Negligible risk | Safe in respiratory compromise |
| Cervical epidural / high spinal | Possible if block reaches C3–C5 | Diaphragmatic paralysis, apnoea |
| Cardiac surgery (cardioplegia) | Cold phrenic nerve injury (left > right) | Temporary hemidiaphragmatic paresis |
B. Hiatus and Reflux — Aspiration Risk
- The oesophageal hiatus at T10, formed by the right crus, is the site of hiatus hernia (the lower oesophageal sphincter is partly maintained by diaphragmatic crural contraction)
- During general anaesthesia, the diaphragm relaxes — crural tone is lost — lower oesophageal sphincter competence is reduced, increasing risk of regurgitation and aspiration
- This is a key reason for the rapid sequence induction (RSI) technique with Sellick's manoeuvre (cricoid pressure) in patients with hiatus hernia, reflux, or full stomach
C. Diaphragmatic Splinting — Postoperative Pain
- Upper abdominal and thoracic surgery lead to reflex inhibition and pain-mediated splinting of the diaphragm
- This causes: reduced tidal volume, inability to cough, retained secretions, atelectasis, and hypoxia
- Managed by: adequate analgesia (regional/neuraxial), incentive spirometry, early mobilisation, physiotherapy
D. Effect on FRC (Functional Residual Capacity)
- The supine position alone shifts the diaphragm ~4 cm cephalad (due to abdominal contents)
- Induction of general anaesthesia causes a further cephalad shift of the dependent (posterior) diaphragm → FRC falls by ~0.5 L (about 20%) immediately on induction
- This fall in FRC reduces the oxygen reserve at intubation, contributing to faster desaturation
E. Neuromuscular Blocking Agents
- The diaphragm is relatively resistant to non-depolarising neuromuscular blockers (NMBAs) compared to the adductor pollicis (peripheral neuromuscular junction monitoring site)
- It recovers faster from blockade than laryngeal muscles; however, complete diaphragmatic paralysis requires higher doses
- This means: a patient showing thumb adductor twitches may still have partial diaphragmatic impairment, relevant during reversal of neuromuscular block
- Residual neuromuscular block (Train-of-Four ratio <0.9) impairs diaphragmatic function, increases airway obstruction risk, and compromises hypoxic ventilatory response
F. Thoracic Epidural and Neuraxial Anaesthesia
- A high thoracic epidural (T1–T4) blocks intercostal muscles but spares the diaphragm (phrenic nerve, C3–C5, is above the block level) — ventilation is maintained, though expiratory reserve volume falls
- A high spinal or total spinal that reaches cervical levels abolishes diaphragmatic function — requires immediate ventilatory support
G. Ultrasound Assessment
- Point-of-care ultrasound (POCUS) of the diaphragm at the 10th rib interspace in the midaxillary line assesses:
- Diaphragm thickness (normal 1.6–2.9 mm at FRC; ~4.5 mm at TLC)
- Thickening fraction on inspiration (correlates with effort and respiratory muscle strength)
- Excursion (>10 mm = adequate function; <10 mm at 24 h post-surgery = higher atelectasis risk)
- Paradoxical cephalad movement = phrenic palsy
- Used for weaning prediction from mechanical ventilation in the ICU
(Murray & Nadel's Textbook of Respiratory Medicine, p. 588)
3. Functions of the Diaphragm in Various Phases of Anaesthesia
Awake Baseline (Reference)
- In the upright position: diaphragm provides ~70% of tidal volume; accessory muscles (intercostals, scalenes) contribute the rest
- In the supine position (pre-anaesthesia): the diaphragm shifts ~4 cm cephalad; posterior (dependent) diaphragm becomes more convex and has longer fibres → by Starling's law, contracts more forcefully → greater ventilation of dependent (posterior/basal) zones where perfusion is also greatest → optimal V/Q matching
Phase 1: Induction of Anaesthesia
| Event | Effect on Diaphragm |
|---|---|
| Anaesthetic agents (propofol, thiopentone, volatile agents) | Dose-dependent reduction in diaphragmatic tone and central respiratory drive |
| Loss of consciousness | Accessory muscle activity ceases; diaphragm becomes the sole driver of respiration |
| Supine + induction | Dependent (posterior) diaphragm loses its convexity and tone — no longer contracts preferentially in dependent zones |
| Abdominal contents transmission | Without diaphragmatic tension to resist, abdominal pressure is transmitted to the lungs — cephalad shift of dependent diaphragm |
| FRC drops by ~0.5 L | Airway closure occurs; dependent alveoli collapse → microatelectasis forms in dorsal/basal regions within minutes of induction |
| High FiO₂ induction | Rapid oxygen absorption in poorly ventilated alveoli compounds absorption atelectasis |
| If muscle relaxants given | Complete paralysis of diaphragm; all spontaneous respiration ceases; diaphragm becomes entirely passive — shifts cephalad proportional to abdominal loading |
Clinical consequence: Desaturation can occur rapidly after induction, especially in obese patients. Pre-oxygenation, PEEP during induction, and upright/ramped positioning (in obese patients) are used to prolong safe apnoea time and minimise atelectasis.
Phase 2: Maintenance of Anaesthesia
A. Spontaneous Ventilation (Light Anaesthesia, LMA)
- Volatile anaesthetics at 1 MAC reduce diaphragmatic activity in a dose-dependent manner
- Tidal volume is maintained (diaphragm still contracts) but respiratory rate and minute volume fall
- Expiratory activity of abdominal muscles increases under volatile anaesthesia (parasternal activity abolished) — contributes to dependent atelectasis
- CO₂ response curve shifts right (higher PaCO₂ threshold for breathing); hypoxic drive is obtunded
B. Controlled Mechanical Ventilation (CMV) with Muscle Relaxants
- The diaphragm is completely paralysed
- Positive pressure ventilation (PPV) inflates lungs from above — the non-dependent (anterior) lung is preferentially ventilated (opposite of spontaneous breathing)
- The dependent (posterior) lung remains poorly ventilated (compressed by cephalad diaphragm and abdominal contents) but continues to receive the most perfusion → V/Q mismatch, shunt, hypoxaemia
- Atelectasis in dependent zones can form/persist throughout maintenance
- PEEP (5–10 cmH₂O) recruits dependent alveoli and restores FRC toward normal
- In the prone position: the diaphragm is displaced caudally by gravity, dependent (now anterior/ventral) lung is decompressed → dramatically improved V/Q matching (basis for prone ventilation in ARDS)
C. Trendelenburg / Steep Head-Down Position
- Abdominal contents push diaphragm further cephalad — FRC falls a further 12%
- Particularly problematic in robotic pelvic surgery (steep Trendelenburg + pneumoperitoneum)
- Increased peak airway pressures; higher risk of barotrauma and atelectasis
D. Pneumoperitoneum (Laparoscopic Surgery)
- Insufflation of CO₂ into the peritoneal cavity markedly elevates intra-abdominal pressure
- Pushes diaphragm cephalad → FRC falls, atelectasis increases, peak airway pressures rise
- CO₂ absorbed from peritoneum adds to arterial CO₂ load — requires increase in minute ventilation
Phase 3: Emergence and Recovery
| Event | Diaphragmatic Role |
|---|---|
| Reversal of neuromuscular block | Diaphragm recovers before laryngeal/pharyngeal muscles; return of diaphragmatic twitches on phrenic stimulation ≠ adequate airway protection |
| Residual block (TOF <0.9) | Impaired diaphragmatic excursion → hypoventilation, hypoxia, inability to clear secretions |
| Neostigmine + atropine reversal | Acetylcholinesterase inhibition restores neuromuscular transmission at diaphragm; bronchoconstriction (muscarinic effect) partially offset by atropine |
| Sugammadex | Rapid, complete reversal of rocuronium/vecuronium → full restoration of diaphragm function; preferred when deep block needs reversal |
| Extubation | Must confirm adequate diaphragmatic function — sustained head lift ≥5 s, TOF ratio ≥0.9, 5-second hand grip, normal tidal volumes |
| Post-extubation phase | Diaphragm re-establishes normal resting position as tone returns; FRC normalises over minutes to hours |
| Postoperative pain (after upper abdominal/thoracic surgery) | Reflex inhibition of phrenic motor output; diaphragmatic excursion reduced even without neuromuscular block — managed by adequate regional analgesia (thoracic epidural, paravertebral block, TAP block) |
Summary: Diaphragm Position Across Anaesthetic Phases
| State | Diaphragm Position (Dependent Zone) | FRC | V/Q |
|---|---|---|---|
| Awake, upright | Normal | Normal | Optimal |
| Supine, awake | Shifted cephalad ~4 cm | ↓ slightly | Near normal |
| Induction, supine | Further cephalad shift; tone lost | ↓ 0.5 L | Worsening |
| Paralysed + IPPV | Passive; maximum cephalad dependent shift | ↓↓ | V/Q mismatch, shunt |
| PEEP applied | Passive but pushed caudal by PEEP | ↑ toward normal | Improved |
| Prone position | Displaced caudally anteriorly | ↑ | Best V/Q in ARDS |
| Trendelenburg | Maximally cephalad | ↓↓ | Worst |
| Emergence / reversal | Tone and active contraction return | ↑ toward normal | Improving |
References
- Gray's Anatomy for Students, pp. 173–174, 198–199, 320, 432–433 (Anatomy, openings, innervation, blood supply)
- Morgan & Mikhail's Clinical Anesthesiology, 7e, pp. 788–789, 917–919 (Innervation, spontaneous ventilation, anaesthetic effects)
- Murray & Nadel's Textbook of Respiratory Medicine (Diaphragm ultrasound, p. 588)
- Perioperative Pulmonary Atelectasis — Biology and Mechanisms. PMC9869183
- Respiratory Function Under Anaesthesia — Indian Journal of Respiratory Care
Phrenic nerve paresis in regard to peripheral nerve block
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Generate a presentation on phrenic nerve paresis in peripheral nerve blocks
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.