Piles examination
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a structured, comprehensive guide to the examination of piles (haemorrhoids) based on S Das's Manual on Clinical Surgery and Bailey & Love's Short Practice of Surgery.
Examination of Piles (Haemorrhoids)
Definition & Background
Haemorrhoids (piles) are symptomatic enlargements of the internal haemorrhoidal venous plexus / anal cushions. The word derives from Greek: haima = blood, rhos = flowing; the Latin synonym pila means a ball.
- Internal piles arise from the internal haemorrhoidal plexus above the dentate line (covered by mucosa, insensate)
- External piles / skin tags arise from the external plexus below the dentate line (covered by skin, sensitive to pain)
- Primary internal piles are classically found at the 3, 7, and 11 o'clock positions with the patient in the lithotomy position, corresponding to the main branches of the superior haemorrhoidal vein (left lateral, right anterior, right posterior)
- Secondary piles (4-5) may develop between the primary positions
Golden Rule of Examination Order
"The anal region must be INSPECTED firstly, PALPATED secondly, and DIGITAL EXAMINATION lastly."
- S Das, Manual on Clinical Surgery
I. Positions for Examination
| Position | Features |
|---|---|
| Left lateral (Sims') | Most popular; patient on left side, buttocks at edge of table, hips and knees well flexed toward chest. Best for inspection and proctoscopy |
| Dorsal (lithotomy) | Patient on back, hips flexed. Suitable for bimanual examination and when patient is too ill to move. Better chance of feeling high rectal lesions |
| Knee-elbow position | Best for palpating prostate and seminal vesicles; also used for proctoscopy and sigmoidoscopy |
| Right lateral | Used for carcinoma at the pelvirectal junction |
II. Inspection
Inspect the perianal region carefully before any instrumentation. Look for:
- Anal tags (external piles) - soft, skin-covered tags at the anal verge; can appear anywhere around the anus
- Sentinel pile - a specific, thickened skin tag at the lower end of a fissure-in-ano; almost always located on the midline posteriorly
- Prolapsed internal piles - pinkish-red vascular cushions protruding at the anus (seen in 3rd/4th degree)
- Fistula-in-ano - note the external orifice, its distance from the anus, and whether anterior or posterior (apply Goodsall's rule for determining internal opening position)
- Fissure-in-ano - a linear ulcer in the anal canal, mostly midline posteriorly; the lower end may be seen when anal margins are gently separated (causes extreme pain)
- Pilonidal sinus, condyloma, carcinoma - excluded on inspection
III. Digital Rectal Examination (DRE)
Key Point
Uncomplicated internal piles CANNOT be felt with the finger - they are diagnosed by proctoscopy. Only chronically inflamed and thrombosed piles are palpable on DRE.
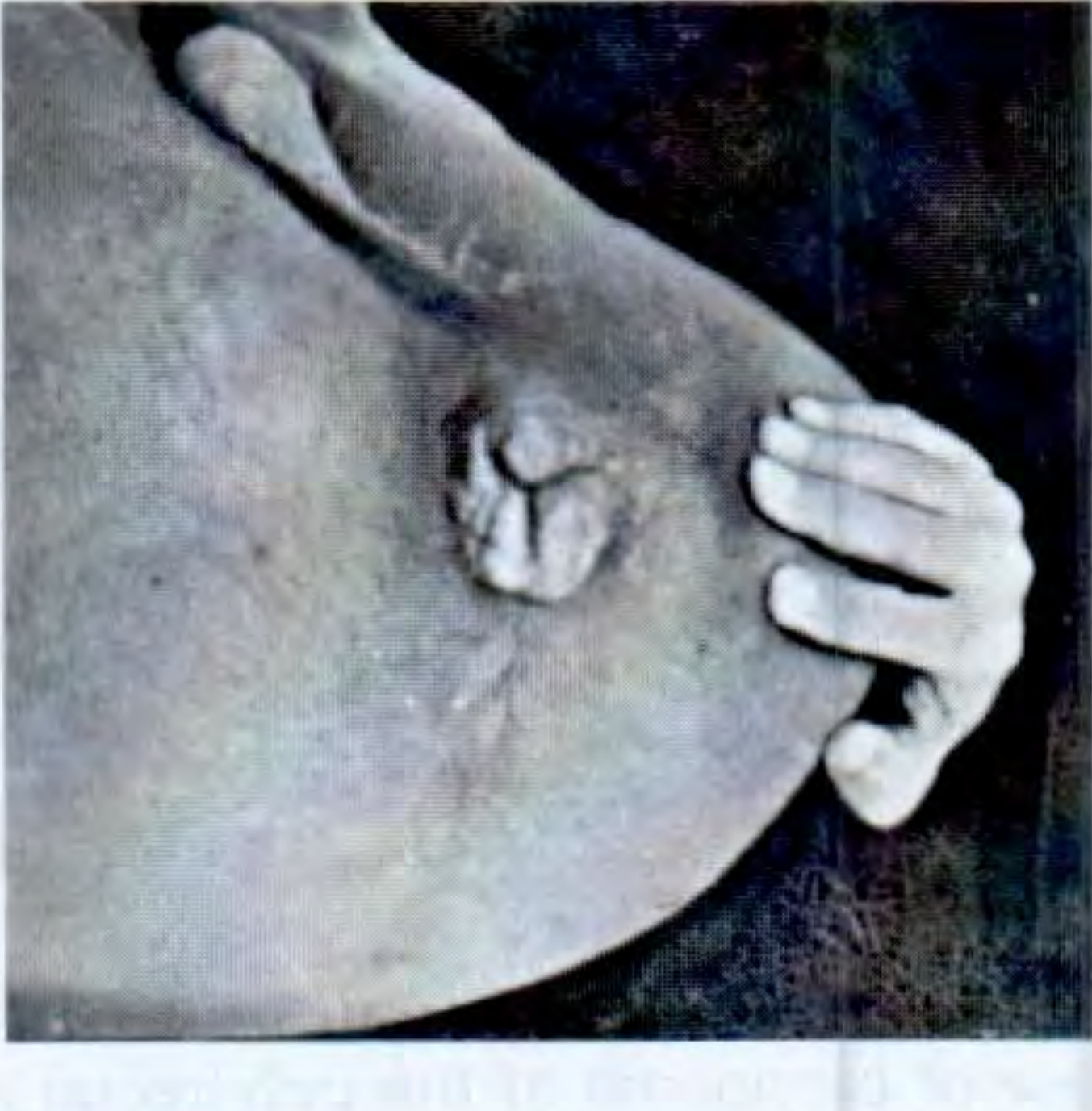
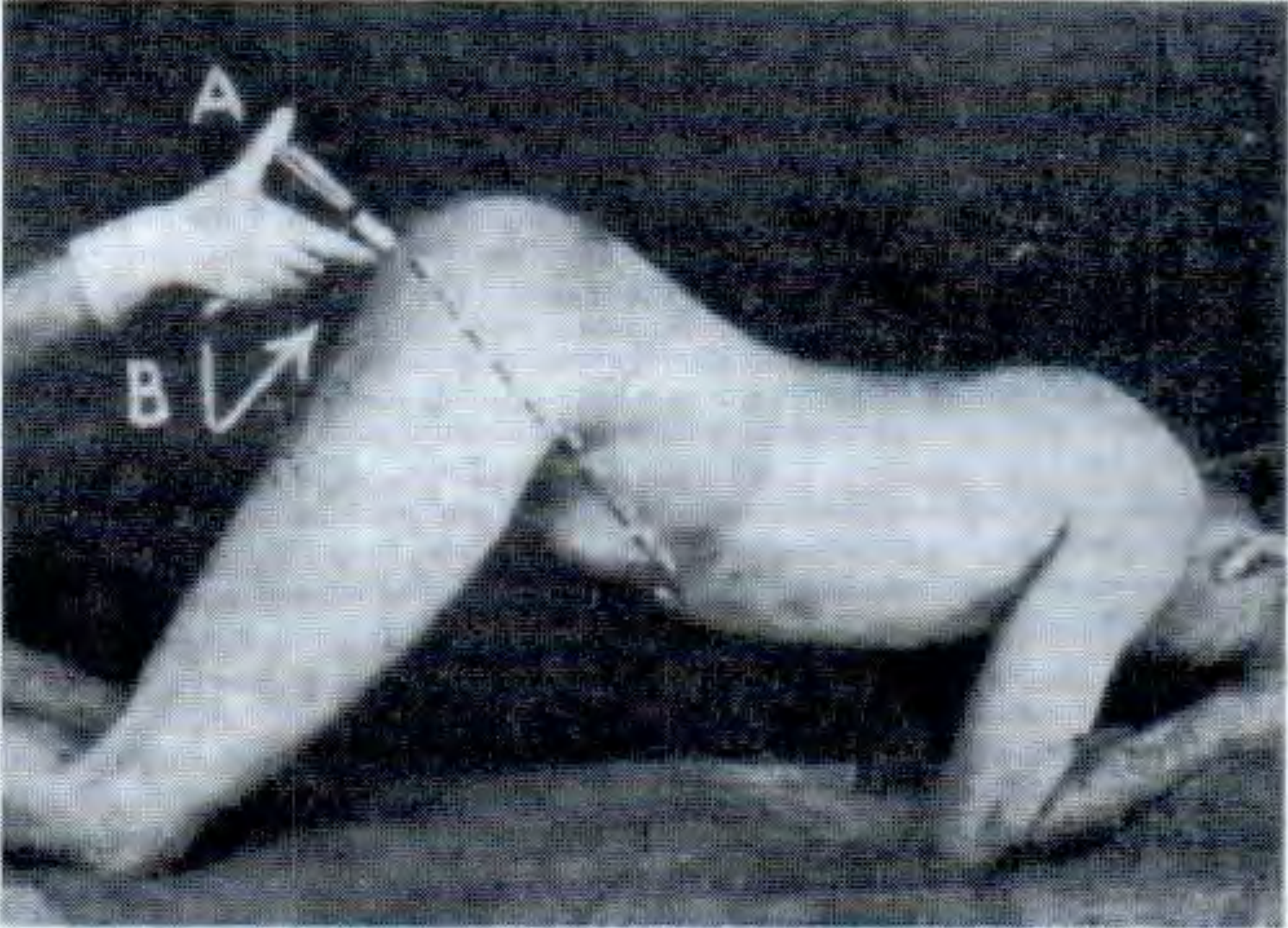
Technique
- Lubricate the examining (right index) finger well
- Place the pulp of the finger at the anus and press gently - allow the sphincter to relax before advancing
- Insert first toward the patient's umbilicus (direction of the anal canal), then curve posteriorly
- The examining finger can explore approximately 10 cm from the anus
What to Assess
In the anal canal:
- Tone of the sphincter (assess internal and external sphincters)
- Tenderness - severe pain suggests fissure-in-ano (may need to defer examination)
- A circular groove just inside the anus marks the intersphincteric groove (boundary between external and internal haemorrhoidal plexuses)
- The ano-rectal ring is felt approximately 3 cm above the anal verge, best felt posteriorly (puborectalis component of levator ani)
Within the rectal lumen:
- Hard faeces (may need to give enema first for proper examination)
- Any prolapsed mass - if felt, ask patient to strain down to bring it lower
In the rectal wall:
- Smooth mucosa = normal; loss of smoothness suggests ulceration
- The valve of Houston (soft mucosal fold) may be felt
- Note any thickening, induration, or mass
Outside the rectal wall (bimanual examination):
- Assess pelvic viscera (uterus, prostate, seminal vesicles, rectovesical/recto-uterine pouch)
IV. Proctoscopy - The Key Investigation for Piles
Proctoscopy is the definitive method for diagnosing internal haemorrhoids. It is mandatory for any patient with rectal bleeding.
Technique
- Patient in left lateral or knee-elbow position
- A warm, well-lubricated proctoscope (with obturator in) is gently inserted, first directed upward and forward toward the patient's umbilicus - this follows the axis of the anal canal
- Once the anal canal is passed, the instrument is directed posteriorly to enter the rectum
- The obturator is withdrawn and the interior is visualized under light
- Piles prolapse into the lumen of the proctoscope as the instrument is slowly withdrawn - this is when they are best visualized
- Note the position, size, and degree of the piles
- Fissures, ulcers, polyps, growths, and the internal opening of a fistula can also be seen
- Biopsy can be taken through the proctoscope if needed
V. Sigmoidoscopy
- A 35 cm instrument that examines the whole rectum and a large part of the sigmoid colon
- Position: knee-elbow or left lateral
- Introduced along the axis of the anal canal; once the tip enters the rectum, all further passage is under direct vision (the obturator is removed)
- Important to exclude rectal carcinoma and inflammatory bowel disease in patients presenting with presumed haemorrhoidal bleeding
VI. Grading of Internal Haemorrhoids (Four Degrees)
| Degree | Features |
|---|---|
| 1st | Bleed only; no prolapse |
| 2nd | Prolapse on straining but reduce spontaneously |
| 3rd | Prolapse on straining; require manual reduction |
| 4th | Permanently prolapsed; cannot be reduced |
Bailey & Love's Short Practice of Surgery, 28th Ed.
VII. Additional Investigations
- Barium enema X-ray / colonoscopy: Mandatory in all cases of internal haemorrhoids to exclude carcinoma above the rectum as the true cause of bleeding
- Sigmoidoscopy / colonoscopy: If barium enema is negative but symptoms persist; to confirm positive findings; to take biopsy
- CT scan / ultrasound: Only in suspected rectal carcinoma - to detect lymph node enlargement and visceral spread
VIII. Differential Diagnosis on Examination
Conditions to distinguish from piles:
- Rectal prolapse (procidentia) - full-thickness protrusion with concentric mucosal rings
- Anal fissure - sentinel pile at the lower end; extreme pain on examination; linear ulcer in anal canal
- Rectal polyp - single soft pedunculated mass
- Carcinoma of the rectum - hard, irregular, ulcerated mass on DRE; does not prolapse into proctoscope
- Fistula-in-ano - track palpable; external opening visible on inspection
IX. Complications Visible on Examination
| Complication | Findings |
|---|---|
| Thrombosis | Acutely tender, firm, blue-black swelling at anal verge |
| Strangulation | Circumferential prolapse with impending mucosal necrosis; distinguish from rectal prolapse |
| Ulceration | Surface mucosal breakdown |
| Gangrene | Black, necrotic pile mass |
Sources: S Das, A Manual on Clinical Surgery, 13th Ed., p. 545-551 | Bailey & Love's Short Practice of Surgery, 28th Ed., p. 1451-1454
How to take history of pateint for hysterectomy surgery
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
I've gathered sufficient material from the textbooks. Now let me compile a thorough, structured answer from the Berek & Novak's Gynecology, Bailey & Love, and standard surgical/anaesthetic pre-op assessment principles.
History Taking for a Patient Undergoing Hysterectomy
Taking a history before hysterectomy has two parts: (1) the gynaecological history that establishes the indication for surgery, and (2) the general pre-operative surgical history that assesses fitness for anaesthesia and identifies risk factors for complications.
1. Presenting Complaint and History of Present Illness
Begin with an open question: "What problem has brought you here?"
Then explore the main symptom in full detail using SOCRATES or equivalent:
- Site - uterus, pelvis, lower abdomen
- Onset - when did it start, sudden or gradual
- Character - nature of pain/bleeding
- Radiation - does pain radiate to back, thighs, rectum
- Associated symptoms - see below
- Timing - relation to menstrual cycle, constant or intermittent
- Exacerbating/relieving factors - posture, intercourse, defecation
- Severity - impact on daily life, work, sleep
2. Gynaecological History (Core Component)
A. Menstrual History (PALM-COEIN approach is helpful)
| Question | What to Ask |
|---|---|
| LMP | Last menstrual period - date, regularity |
| Cycle | Length of cycle (normal 21-35 days), duration of flow (normal 2-7 days) |
| Amount | Number of pads/tampons per day, passage of clots, flooding, soaking through clothing or bedsheets (menorrhagia) |
| Dysmenorrhoea | Painful periods - primary vs secondary; timing (onset with flow or premenstrual); severity; response to analgesia |
| Intermenstrual bleeding (IMB) | Bleeding between periods |
| Post-coital bleeding (PCB) | Bleeding after intercourse - suggests cervical pathology |
| Post-menopausal bleeding | If applicable - always consider endometrial cancer |
B. Pain History
- Location, character (crampy, constant, burning)
- Relation to menstrual cycle - cyclical (endometriosis, dysmenorrhoea) vs non-cyclical (fibroids, PID)
- Dyspareunia - superficial or deep; deep dyspareunia suggests endometriosis, PID, adenomyosis
- Chronic pelvic pain - duration; prior investigations; response to treatment
C. Vaginal Discharge
- Color, odor, consistency, associated itch or irritation
- Suggestive of infection (PID, cervicitis)
D. Urinary Symptoms
- Frequency, urgency, incontinence, dysuria
- Important because hysterectomy can affect bladder function (especially total/radical hysterectomy)
- Stress incontinence may be treated concurrently or may worsen post-operatively
E. Bowel Symptoms
- Constipation, dyschezia (pain on defecation - suggests posterior endometriosis/deep infiltrating endometriosis)
- Rectal bleeding - must be excluded as a separate pathology
F. Sexual History
- Dyspareunia (as above)
- Current sexual activity - relevant to post-operative counselling and choice of route (vaginal vs abdominal)
- Partner status - relevant for vaginal vault prolapse counselling
3. Obstetric History
| Question | Relevance |
|---|---|
| Gravidity and parity (G_P_) | Determines future fertility desires; parity affects uterine size |
| Mode of deliveries | Previous caesarean sections increase risk of adhesions, bladder injury |
| Complications of pregnancy | PPH, preeclampsia |
| Uterine/cervical surgeries | LLETZ, cone biopsy, myomectomy - affect anatomy and adhesion risk |
| Future fertility wishes | Essential - if the patient desires future pregnancy, hysterectomy may not be appropriate (consider alternatives) |
4. Gynaecological Surgical and Medical History
- Previous abdominal/pelvic surgeries (adhesions, anatomical distortion)
- Previous hysteroscopy, D&C, laparoscopy
- Known uterine fibroids - size, number, symptoms, previous treatments
- Known endometriosis - extent, previous surgeries
- Known pelvic inflammatory disease (PID) - chronic PID increases adhesion risk
- Cervical screening history - last Pap smear result; any previous CIN treatment (LLETZ, cone biopsy)
- History of ovarian cysts or adnexal pathology
- Known malignancy (cervical, endometrial, ovarian) - determines extent of surgery (simple vs radical hysterectomy)
5. Prior Medical and Surgical History (Pre-operative Assessment)
Medical History
| System | Key Points |
|---|---|
| Cardiovascular | Hypertension, ischemic heart disease, heart failure, arrhythmias, prior MI, stents, pacemaker |
| Respiratory | Asthma, COPD, obstructive sleep apnoea (affects anaesthesia) |
| Endocrine | Diabetes mellitus (glycaemic control, wound healing), thyroid disease |
| Haematological | Anaemia (common with menorrhagia - needs correction pre-op), clotting disorders, VTE history |
| Renal / Hepatic | Affects drug metabolism and clearance |
| Obesity | BMI - increases surgical complexity, VTE risk, wound infection |
| Neurological | Epilepsy, prior stroke |
| Immunosuppression | Steroids, chemotherapy - infection and healing risk |
Surgical History
- Any prior abdominal or pelvic surgery (laparotomy scars, adhesions)
- Complications of previous anaesthesia (awareness, difficult intubation, PONV, malignant hyperthermia in family)
- Previous DVT or PE (VTE prophylaxis planning)
6. Drug and Allergy History
| Drug Category | Reason for Asking |
|---|---|
| Anticoagulants (warfarin, heparin, DOACs) | Bridging therapy planning; timing of cessation |
| Antiplatelets (aspirin, clopidogrel) | Cessation timing; risk of thrombosis vs bleeding |
| Oral contraceptive pill | Stop 4-6 weeks before surgery - VTE risk |
| HRT / oestrogen therapy | VTE risk; stop before elective surgery |
| Steroids | Adrenal suppression - perioperative steroid cover needed |
| NSAIDs | Renal impairment; stop pre-operatively |
| Iron supplements | Pre-operative correction of anaemia |
| Metformin | Withhold on day of surgery |
| Herbal supplements | Many affect coagulation (ginkgo, garlic, ginseng) |
| Allergies | Latex (critical in OR), drugs, iodine, adhesives |
7. Family History
- Ovarian, endometrial, or breast cancer (BRCA1/BRCA2 mutation - influences decision on concurrent oophorectomy)
- Colon cancer (Lynch syndrome - endometrial cancer risk)
- Bleeding or clotting disorders
- Anaesthetic complications (malignant hyperthermia - autosomal dominant)
8. Social History
| Item | Relevance |
|---|---|
| Smoking | Increases VTE, anaesthetic, and wound complications; cessation improves outcomes |
| Alcohol / substance use | Affects drug metabolism, anaesthesia, healing |
| Occupation | Return-to-work planning; lifting restrictions post-op |
| Support at home | Who will care for the patient post-discharge |
| Marital / partner status | Post-operative sexual counselling (vaginal vault length, libido after oophorectomy) |
| Mental health | Prior depression, anxiety - hysterectomy affects body image; risk of psychological sequel especially if premenopausal |
9. Review of Systems (Relevant to Surgery)
- Exercise tolerance - functional capacity (METs); can she climb 4 flights of stairs without stopping? (relevant to cardiac risk)
- Anaemia symptoms - fatigue, breathlessness, palpitations (common with menorrhagia)
- DVT/PE symptoms - current leg swelling, chest pain
- Nutritional status - weight loss, poor appetite (malignancy workup)
- Urinary incontinence - may be addressed concurrently
10. Specific Considerations by Indication
| Indication for Hysterectomy | Key History Points to Emphasize |
|---|---|
| Uterine fibroids | Duration, size/bulk symptoms (urinary frequency, constipation), menorrhagia, subfertility, prior treatments (GnRH analogues, UAE, myomectomy) |
| Endometrial cancer | Post-menopausal bleeding, abnormal uterine bleeding, family history (Lynch syndrome) |
| Cervical cancer | PCB, vaginal discharge, screening history, STI history, HPV vaccination |
| Ovarian cancer | Abdominal distension, early satiety, bloating, family history (BRCA) |
| Adenomyosis | Heavy painful periods, uterine enlargement, failed medical treatment |
| Endometriosis | Cyclical pain, dyspareunia, dysmenorrhoea, dyschezia, subfertility, prior laparoscopy |
| Uterovaginal prolapse | Dragging sensation, "something coming down," urinary symptoms, obstructed defecation, prior prolapse repairs |
| Chronic pelvic pain | At least 6 months duration, multidisciplinary treatment attempted, no correctable pathology found (ACOG criteria) |
11. Counselling Points to Address During History
- Fertility - Has the patient completed her family? Does she understand that hysterectomy is irreversible?
- Menopause - If bilateral salpingo-oophorectomy is planned concurrently, explain surgical menopause (hot flushes, bone density loss, cardiovascular risk, need for HRT if premenopausal)
- Route of surgery - Abdominal (TAH), vaginal (VH), or laparoscopic (TLH/LAVH) - discuss preferences and expectations for recovery
- Expected outcomes - symptom relief, risks (bleeding, infection, bladder/ureter/bowel injury, VTE, vault prolapse)
Sources: Berek & Novak's Gynecology; Bailey & Love's Short Practice of Surgery, 28th Ed.; Morgan & Mikhail's Clinical Anesthesiology, 7th Ed.
Create a checklist or proforma for hysterectomy pre-op history
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.