Biomedical wastes* - define, categories*, method of disposal; colour code system of bags for disposal 2. Hospital-Acquired Infections - define, mention two organisms 3. Segregation of Hospital Waste LAQ 1. Hospital Acquired Infections 2 MBBS REFER APURB SHASTRI MUHS EXAM ORITNTED detail answer of questions colour diagrams as well for exam important points for muhs exam cover all
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
I now have all the content needed. Let me compile the full MUHS exam-oriented answer.
🏥 MUHS 2nd MBBS - Community Medicine (PSM)
Biomedical Waste, Hospital-Acquired Infections & Hospital Waste Segregation
(Based on Park's Textbook of Preventive and Social Medicine - Standard MUHS Reference)
SHORT ANSWER QUESTIONS (SAQ)
1. BIOMEDICAL WASTE
✅ Definition
"Bio-medical waste means any waste which is generated during the diagnosis, treatment or immunization of human beings or animals, or in research activities pertaining thereto or in the production or testing of biologicals."
- Bio-Medical Waste (Management & Handling) Rules, 1998 (updated 2016), India
- 75-90% of healthcare waste is non-risk / general waste (comparable to domestic waste)
- Remaining 10-25% is hazardous and creates health risks
✅ Sources of Biomedical Waste
Hospitals, nursing homes, clinics, PHCs, laboratories, blood banks, mortuaries, slaughterhouses, research organizations, vaccination centres, biotechnology institutions
✅ CATEGORIES & COLOUR CODE SYSTEM (BMW Rules 2016 - Schedule 1)
EXAM KEY: 4 colour codes = Yellow, Red, White (Translucent), Blue
╔══════════════════════════════════════════════════════════════════════════════════╗
║ BIOMEDICAL WASTE - COLOUR CODING (BMW Rules 2016) ║
╠══════════╦══════════════════════════════════════════╦══════════════════════════╣
║ COLOUR ║ TYPE OF WASTE ║ DISPOSAL METHOD ║
╠══════════╬══════════════════════════════════════════╬══════════════════════════╣
║ 🟡 ║ (a) Human anatomical waste (tissues, ║ Incineration / Plasma ║
║ YELLOW ║ organs, body parts, foetus) ║ Pyrolysis / Deep burial ║
║ (Non- ║ (b) Animal anatomical waste ║ ║
║ chlor. ║ (c) Soiled waste (dressings, blood- ║ Incineration / deep ║
║ plastic ║ soaked cotton, plaster casts) ║ burial / autoclaving ║
║ bag) ║ (d) Expired/discarded medicines, ║ Return to manufacturer / ║
║ ║ cytotoxic drugs, ampoules, vials ║ Incineration >1200°C ║
║ ║ (e) Chemical waste (disinfectants) ║ Incineration / Plasma ║
║ ║ (f) Chemical liquid waste ║ Effluent treatment system║
║ ║ (g) Discarded linen, mattresses, ║ Chemical disinfection + ║
║ ║ beddings (blood-soaked) ║ Incineration ║
║ ║ (h) Microbiology/lab waste (blood bags, ║ Pre-treat → sterilize → ║
║ ║ lab cultures, vaccines, cell cultures║ Incineration ║
╠══════════╬══════════════════════════════════════════╬══════════════════════════╣
║ 🔴 ║ Contaminated (recyclable) waste: ║ Autoclaving / ║
║ RED ║ IV tubes, bottles, catheters, urine bags,║ Microwaving / ║
║ (Non- ║ syringes (without needles), gloves, ║ Hydroclaving → Shredding ║
║ chlor. ║ vaccutainers (needles cut) ║ → Recycling ║
║ plastic ║ ║ ║
║ bag) ║ ║ ║
╠══════════╬══════════════════════════════════════════╬══════════════════════════╣
║ ⬜ ║ Waste sharps (including metals): ║ Autoclaving / ║
║ WHITE ║ Needles, syringes with fixed needles, ║ Dry heat sterilization / ║
║(Translu- ║ scalpels, blades, lancets and other ║ Chemical disinfection → ║
║ cent) ║ sharps used in patient care ║ Shredding/mutilation → ║
║ Puncture-║ ║ Sent to metal recycler ║
║ proof ║ ║ ║
║container)║ ║ ║
╠══════════╬══════════════════════════════════════════╬══════════════════════════╣
║ 🔵 ║ Glassware: Broken/discarded and ║ Disinfection by soaking ║
║ BLUE ║ contaminated glass including medicine ║ in sodium hypochlorite ║
║ (Card- ║ vials and ampoules EXCEPT those with ║ or any other disinfectant║
║ board ║ cytotoxic wastes ║ for 30 min → sent to ║
║ box or ║ ║ glass recyclers OR ║
║ puncture║ ║ defacing and disposal ║
║ -proof ║ ║ in secure landfill ║
║container)║ ║ ║
╚══════════╩══════════════════════════════════════════╩══════════════════════════╝
🔑 MUHS Memory Aid:
| Colour | Waste Type | Remember as |
|---|---|---|
| Yellow | Anatomical, soiled, expired drugs, lab waste, chemical | "Yellow = Dangerous/Infectious/Body parts" |
| Red | Recyclable contaminated plastics | "Red = Recyclable plastics" |
| White | Sharps (metal) | "White = Wounding sharps" |
| Blue | Broken glass | "Blue = Breakable glass" |
✅ Methods of Disposal of Biomedical Waste
I. Incineration
- High-temperature dry oxidation process
- Reduces organic/combustible waste to inorganic incombustible matter
- Significant reduction in volume and weight
- Types: Rotary kiln, pyrolytic double-chamber, single-chamber, drum/brick incinerator
- NOT suitable for: PVC plastics, pressurized containers, silver-containing wastes, mercury/cadmium waste, radioactive waste
II. Autoclave (Steam Sterilization)
- Uses pressurized steam at 121°C or 134°C
- Effective for infectious waste, lab waste, sharps after chemical disinfection
- Followed by shredding/mutilation
III. Chemical Disinfection
- Uses sodium hypochlorite, formaldehyde, glutaraldehyde
- Suitable for liquid waste, blood, lab cultures
- Requires qualified technicians
IV. Microwave Irradiation
- Frequency ~2450 MHz, wavelength 12.24 nm
- Destroys microorganisms by heating water within waste
- Efficiency checked by bacteriological and virological tests
V. Land Disposal
- Sanitary landfills (NOT open dumps for biomedical waste)
- Must have: geological isolation, engineering preparation, staff control, organized deposit with daily coverage
- For small facilities lacking treatment options
VI. Inertization
- Mixing waste with cement and substances before disposal
- Typical mix: 65% pharmaceutical waste + 15% lime + 15% cement + 5% water
- Prevents toxic substances from migrating to groundwater
VII. Deep Burial
- For anatomical waste in areas without incineration facilities
- Pit lined with lime, depth 2 metres, covered with lime before closure
2. HOSPITAL-ACQUIRED INFECTIONS (HAI)
✅ Definition
Hospital-Acquired Infection (Nosocomial Infection) is an infection originating in a patient while in a hospital or other health care facility. It denotes a new disorder (unrelated to the patient's primary condition) that was NOT present or incubating at the time of admission or residual of an infection acquired during a previous admission.
- Infections occurring more than 48 hours after admission are considered nosocomial
- Also includes infections acquired in hospital but appearing after discharge
- Infections among hospital staff are also considered nosocomial
(Park's Textbook of PSM)
✅ Two Important Organisms Causing HAI
| Organism | Type of HAI |
|---|---|
| Staphylococcus aureus | Wound infections, bacteraemia, skin infections (carried in nose/skin of staff) |
| Escherichia coli (B. coli) | Urinary tract infections (most common HAI) |
Other important organisms: Haemolytic Streptococci (throat of staff), Salmonella (gut of staff), Pseudomonas aeruginosa, Klebsiella
3. SEGREGATION OF HOSPITAL WASTE
✅ Definition of Segregation
Segregation is the separation of different categories of waste at the point of generation to reduce risk, facilitate appropriate treatment, and minimize the quantity of waste requiring specialized treatment.
✅ Principle
"Waste that is not segregated shall be treated as Category 1 waste (most hazardous) and disposed of accordingly."
✅ Colour-Coded Segregation at Source
| Container/Bag Colour | Waste Category |
|---|---|
| Yellow non-chlorinated plastic bag | Anatomical, soiled, chemical, lab waste, expired drugs |
| Red non-chlorinated plastic bag | Contaminated recyclable plastics |
| White puncture-proof translucent container | Sharps (needles, blades, scalpels) |
| Blue cardboard box / puncture-proof container | Broken glass, glass ampoules |
| Black bag | General municipal solid waste (non-biomedical) |
✅ Steps in Hospital Waste Management
- Generation - waste produced at point of care
- Segregation - at source, using colour-coded containers
- Collection - in colour-coded bags/containers
- Transport - using closed trolleys to central storage
- Storage - not exceeding 48 hours
- Treatment - incineration, autoclave, chemical disinfection
- Disposal - landfill, recycling, energy recovery
LONG ANSWER QUESTION (LAQ) - MUHS Exam Style
🔴 HOSPITAL ACQUIRED INFECTIONS (HAI) - DETAILED ANSWER
Introduction
Hospital-Acquired Infection (HAI), also known as Nosocomial Infection, is a major public health concern and indicator of quality of health care delivery. A high frequency of HAI is evidence of poor quality of health service delivery.
Definition
- WHO Definition: "Nosocomial infections, also called hospital-acquired infections, are infections acquired during hospital care which are NOT present or incubating at admission."
- Infections occurring more than 48 hours after admission are usually considered nosocomial
- Park's Definition: "Hospital-acquired infection is cross infection of one patient by another or by doctors, nurses and other hospital staff, while in hospital."
- Includes infections among hospital staff
- Includes infections acquired in hospital but manifesting after discharge
Magnitude & Significance
- HAI affects millions of patients worldwide each year
- Leads to prolonged hospital stay, increased costs, morbidity and mortality
- Special risk groups: ICU patients, immunocompromised, surgical patients, neonates
Types of Nosocomial Infections
- Endemic - most common; occur routinely in hospitals
- Epidemic - unusual increase above baseline of a specific organism/infection (outbreak)
Analysis of HAI - Three Angles
1. SOURCE
(a) Patients:
- Viral infections (measles, rubella, influenza, hepatitis B)
- Skin infections (discharging wounds, bed sores, infected skin lesions, eczema, psoriasis, boils)
- Respiratory infections (pulmonary TB, sore throat, chest infection)
- Urinary tract infections (E. coli)
(b) Hospital Staff:
- Staphylococcus aureus - carried in nose or skin
- Haemolytic Streptococci - carried in throat
- Salmonella - carried in gut
- Staff with active infections are a major risk
(c) Environment:
- Hospital dust, linen, bed clothes, furniture, sinks, basins, door handles, air
- All are laden with microorganisms
2. ROUTES OF SPREAD
| Route | Example |
|---|---|
| Direct contact | Hands of nurse/doctor to patient |
| Droplet infection | Coughing, sneezing (droplets from nose/throat) |
| Air-borne particles | Droplet nuclei, fungal spores |
| Hospital dust | Released into air during cleaning |
| Hospital procedures | Catheterization, IV procedures, infected catgut, dressings, sputum cups, bed pans, urinals |
3. RECIPIENTS (Susceptible Patients)
All hospitalized patients are potential recipients, especially:
- Severely ill patients
- Patients under corticosteroid therapy (immunosuppressed)
- Patients in Intensive Care Units
- Patients in urological, geriatric, and neonatal (special baby care) wards
Common Sites of Nosocomial Infection
(French National Prevalence Survey)
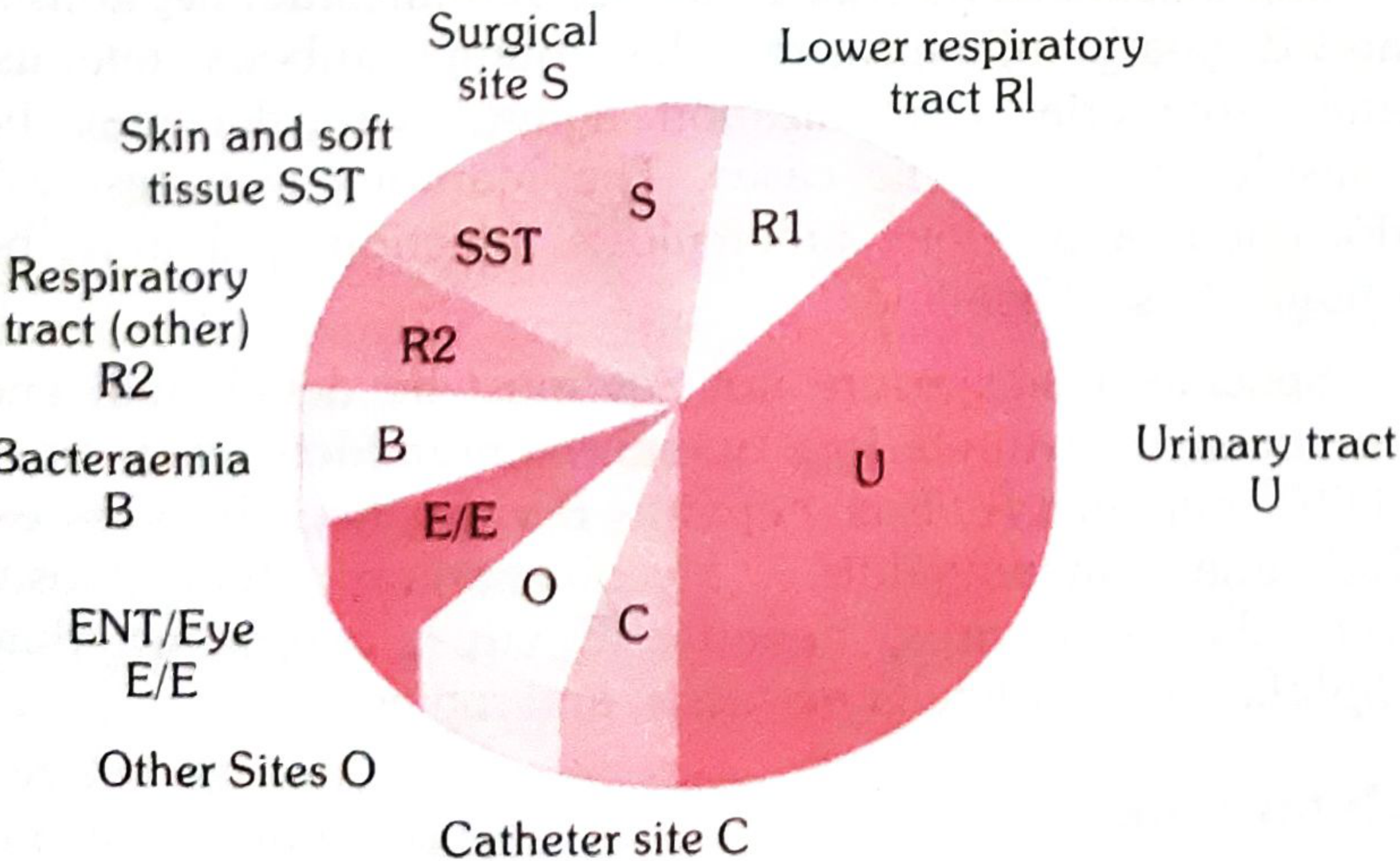
| Site | Features |
|---|---|
| Urinary tract (U) - LARGEST segment | Mostly catheter-associated; E. coli |
| Lower respiratory (R1) | Ventilator-associated pneumonia |
| Surgical site (S) | Post-operative wound infection |
| Skin & soft tissue (SST) | Wound infections, bed sores |
| Bacteraemia (B) | IV line, catheter-related sepsis |
| ENT/Eye (E/E) | Conjunctivitis, otitis |
| Other sites (O) | Gastrointestinal, reproductive |
| Catheter site (C) | Vascular catheter infection |
Simplified Criteria for Surveillance (WHO)
| Type of HAI | Simplified Criteria |
|---|---|
| Surgical site infection | Any purulent discharge, abscess or spreading cellulitis at surgical site within 1 month of operation |
| Urinary infection | Positive urine culture (1 or 2 species) with ≥10⁵ bacteria/ml ± clinical symptoms |
| Respiratory infection | Respiratory symptoms + ≥2 signs: cough, purulent sputum, new infiltrate on CXR |
| Vascular catheter infection | Inflammation, lymphangitis or purulent discharge at catheter insertion site |
| Septicaemia | Fever or rigors + ≥1 positive blood culture |
Important Organisms in HAI
| Organism | Common HAI Caused |
|---|---|
| Staphylococcus aureus | Wound infections, bacteraemia, skin infections |
| Escherichia coli | UTI (most common HAI) |
| Pseudomonas aeruginosa | Respiratory infections, wound infections |
| Klebsiella pneumoniae | Pneumonia, UTI |
| Haemolytic Streptococcus | Wound infections, septicaemia |
| Clostridium difficile | Antibiotic-associated diarrhoea |
| Hepatitis B virus | Blood-borne, needlestick |
| Candida spp. | Fungal infection in immunocompromised |
Prevention of HAI (MUHS IMPORTANT)
(a) Isolation
- Infectious patients must be isolated
- Susceptible patients should NOT be placed next to source patients
(b) Hospital Staff
- Staff with skin diseases, sore throat, cold, ear infection, diarrhoea must stay away from work
- Personal hygiene and regular change of aprons/clothing
(c) Hand Washing - MOST IMPORTANT
- The most common route of infection is via hands
- Must wash hands before and after every patient contact
- Wash promptly after contact with infective material
- Wash immediately after removing gloves
(d) Protective Clothing
- Gown: washable material, buttoned/tied at back, with plastic apron if needed
- Gloves: plastic gloves for contact with blood, body fluids, mucous membranes
- Mask: surgical mask to protect from splashes
(e) Standard Precautions (Universal Precautions)
- Use no-touch technique wherever possible
- Handle all sharps with extreme care
- Clean up spills of infective material promptly
- Ensure patient-care equipment is disinfected/sterilized between each patient use
- Appropriate waste handling
- Use closed drainage systems for catheters
(f) Prevention by Infection Type
| Infection | Proven Effective Measures |
|---|---|
| UTI | Limit catheter duration, aseptic technique at insertion, maintain closed drainage, antiseptic perineal cleaning |
| Surgical site | Surgical technique, clean OT, aseptic practice, limit pre-op hospital stay, preoperative shower, optimal antibiotic prophylaxis |
| Pneumonia (VAP) | Aseptic intubation/suctioning, limit ventilator duration, non-invasive ventilation, influenza vaccination for staff |
| Vascular catheter | Closed system, limit duration, aseptic technique at insertion, surgical asepsis for central lines |
(g) Health Care Worker Safety
- Review immunization history at recruitment
- Screen for prior exposures to communicable diseases (e.g., TB)
- Programmes to prevent occupational exposure
🔑 MUHS EXAM HIGH-YIELD POINTS
| Fact | Detail |
|---|---|
| Definition trigger | >48 hours after admission |
| Most common HAI | UTI (catheter-associated) |
| Most common organism | E. coli for UTI; Staph. aureus for wound |
| Most important preventive measure | Hand washing |
| High-risk wards | ICU, urology, geriatrics, neonates |
| HAI indicates | Poor quality of health service delivery |
| Term "endemic" | Routine/background HAI |
| Term "epidemic" | Unusual increase above baseline |
Sources: Park's Textbook of Preventive and Social Medicine (standard MUHS 2nd MBBS reference)
This is a shared conversation. Sign in to Orris to start your own chat.