Drug of choice for diabetic patients
Reading File
Finding Sources
Searching PubMed
"metformin" AND "type 2 diabetes" AND "first line"
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer.
Drug of Choice for Diabetic Patients
The answer differs by diabetes type and patient comorbidities. Here is a full breakdown:
Type 1 Diabetes Mellitus
Drug of choice: Insulin (mandatory - not optional)
Type 1 DM involves absolute insulin deficiency due to autoimmune destruction of beta cells. Insulin replacement is the only effective therapy. The regimen typically combines:
| Insulin Type | Examples | Use |
|---|---|---|
| Rapid-acting | Aspart, Lispro, Glulisine | Mealtime (prandial) control |
| Short-acting | Regular insulin | Mealtime or correction doses |
| Intermediate | NPH insulin | Basal control |
| Long-acting | Glargine, Detemir, Degludec | Basal (once daily, less hypoglycemia) |
Pramlintide (synthetic amylin analog) may be added for additional mealtime glycemic control in T1DM.
- Lippincott Illustrated Reviews: Pharmacology, p. 823
Type 2 Diabetes Mellitus
First-line drug of choice: Metformin (a biguanide)
"The biguanide metformin is the preferred initial agent for management of type 2 diabetes. The efficacy, low cost, and safety of metformin are the reasons for its recommendation as the drug of choice."
- Lippincott Illustrated Reviews: Pharmacology, p. 822
Why Metformin?
- Decreases hepatic glucose production (reduces gluconeogenesis)
- Does not cause hypoglycemia
- Does not cause weight gain
- Low cost, well-studied safety profile
- Monitor: renal function (avoid in severe renal impairment) and vitamin B12 levels (long-term use)
Management Algorithm (ADA Guidelines)
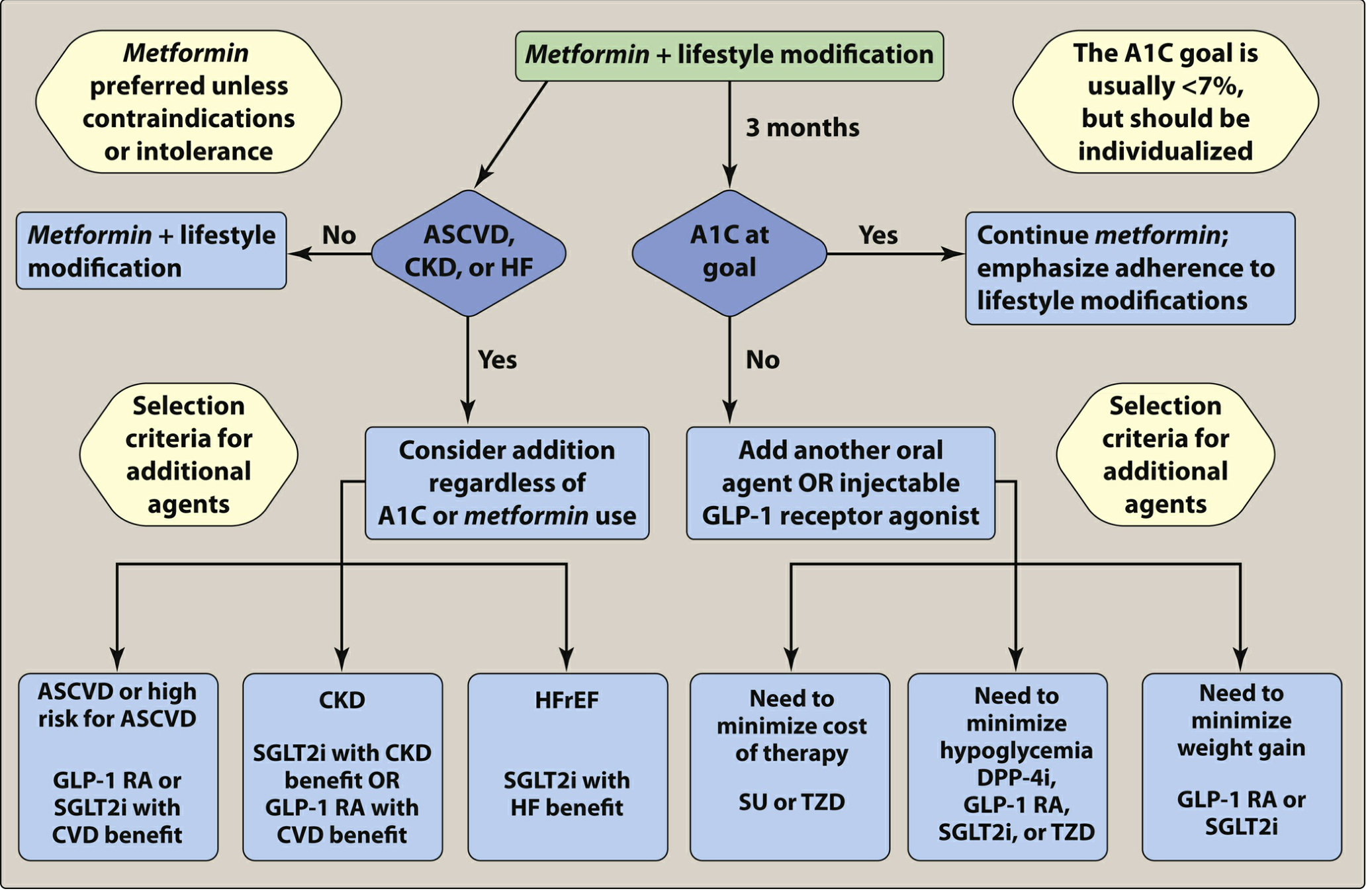
Figure 24.16 - Lippincott Illustrated Reviews: Pharmacology
When to Add a Second Agent (Beyond Metformin)
If A1C target is not reached after 3 months, or if the patient has specific comorbidities, add agents based on the clinical picture:
| Comorbidity | Preferred Add-on |
|---|---|
| ASCVD or high CV risk | GLP-1 RA (liraglutide, semaglutide) OR SGLT2i with CV benefit (empagliflozin, canagliflozin) |
| Chronic Kidney Disease (CKD) | SGLT2i with CKD benefit OR GLP-1 RA with CV benefit |
| Heart Failure with reduced EF (HFrEF) | SGLT2i (dapagliflozin, empagliflozin - also approved for HFpEF) |
| Need to minimize hypoglycemia | DPP-4i, GLP-1 RA, SGLT2i, or TZD |
| Need to minimize weight gain | GLP-1 RA or SGLT2i |
| Cost minimization | Sulfonylurea (SU) or TZD |
Full Drug Class Summary for Type 2 DM
| Class | Examples | Mechanism | Hypoglycemia Risk | Notes |
|---|---|---|---|---|
| Biguanides | Metformin | Decreases hepatic glucose production | No | 1st-line DOC |
| Sulfonylureas | Glimepiride, Glyburide | Stimulates insulin secretion | Yes | Weight gain; avoid glyburide in renal impairment |
| Meglitinides | Repaglinide, Nateglinide | Stimulates insulin secretion | Yes (rarely) | Taken with meals; postprandial effect |
| TZDs | Pioglitazone, Rosiglitazone | PPAR-γ agonist → reduces insulin resistance | No | Avoid in heart failure or liver disease |
| DPP-4 inhibitors | Sitagliptin, Linagliptin | Increases glucose-dependent insulin release; decreases glucagon | No | Renal dose adjustment needed (except linagliptin); risk of pancreatitis |
| SGLT2 inhibitors | Empagliflozin, Canagliflozin, Dapagliflozin | Increases urinary glucose excretion | No | Reduces CV mortality and HF; risk of genitourinary infections |
| GLP-1 RAs | Liraglutide, Semaglutide, Exenatide | Increases insulin release, decreases glucagon, slows gastric emptying | No | Weight loss benefit; liraglutide/semaglutide reduce CV mortality |
| α-Glucosidase inhibitors | Acarbose, Miglitol | Decreases glucose absorption | No | GI side effects; taken with meals |
| Amylin analog | Pramlintide | Slows gastric emptying, suppresses glucagon | No | Used adjunctively with insulin |
- Lippincott Illustrated Reviews: Pharmacology, pp. 821-823; ROSEN's Emergency Medicine, p. 3510-3513
Special Situations
| Situation | Drug of Choice |
|---|---|
| Type 1 DM | Insulin (mandatory) |
| Type 2 DM (general) | Metformin |
| Pregnancy / GDM | Insulin is DOC; metformin or glyburide used in certain cases |
| Type 2 with CVD | Metformin + GLP-1 RA or SGLT2i |
| Type 2 with CKD | Metformin (if eGFR adequate) + SGLT2i |
| Type 2 with HFrEF | Metformin + SGLT2i |
| Kidney transplant | Metformin (if adequate GFR) |
- Swanson's Family Medicine Review; ROSEN's Emergency Medicine; Brenner and Rector's The Kidney
Key takeaway: Metformin remains the universal first-line drug of choice for Type 2 DM. The modern paradigm also mandates early addition of SGLT2 inhibitors or GLP-1 receptor agonists in patients with established CVD, CKD, or heart failure - regardless of whether A1C is at goal - due to their proven mortality and organ-protection benefits.
This is a shared conversation. Sign in to Orris to start your own chat.