Morel lavelle Leison
Reading File
Searching the Web
Morel-Lavallee lesion clinical features treatment 2024
Finding Sources
Searching PubMed
"Morel-Lavallee" lesion
Reading File
Reading File
Reading Article
PMID: 40905976
Loading Image
Loading Image
Finding Sources
Now I have rich content from Campbell's, Rockwood & Green's, web sources, and the latest 2026 systematic review. Here is a comprehensive overview:
Morel-Lavallée Lesion
Definition & Pathophysiology
The Morel-Lavallée lesion (MLL) is a closed internal degloving injury first described by French surgeon Victor Auguste François Morel-Lavallée in 1863. It results from tangential shearing forces (typically high-velocity trauma) that abruptly separate the skin and subcutaneous tissue from the underlying deep fascia. This disrupts perforating vessels, lymphatics, and cutaneous nerves, creating a potential space that fills with blood, lymph fluid, and necrotic/viable fat globules. Over time, the body's inflammatory response leads to encapsulation by dense fibrotic tissue, making the cavity persistent and increasingly resistant to non-operative treatment.
Key anatomy: The lesion forms in regions where skin is mobile over rigid bony prominences and there is abundant subcutaneous fat - explaining its typical distribution.
Epidemiology & Common Sites
Site frequency (approximate):
| Location | Frequency |
|---|---|
| Pelvis / greater trochanter | ~69% |
| Knee (prepatellar) | ~16% |
| Gluteal region | ~6% |
| Lumbosacral | ~3% |
| Abdominal wall | ~1.5% |
| Lower leg | ~1.5% |
- Commonly associated with pelvic fractures, acetabular fractures, and proximal femur fractures (the bony injury is often the distracting diagnosis)
- More common in obese individuals and in high-energy mechanisms (road traffic accidents, falls, crush injuries)
Clinical Features
Signs and symptoms appear within hours to days of injury, but up to 33% present months to years later (delayed presentation):
- Fluctuant, boggy, compressible swelling - the hallmark finding
- Ecchymosis/bruising and skin discoloration
- Skin hypermobility - the skin slides freely over the underlying tissue
- Decreased skin sensation - due to shearing of cutaneous nerves
- Pain and tautness over the area
- Possible skin necrosis (acute or delayed) if the overlying skin is devascularized
The lesion is frequently missed initially because the clinician's attention is drawn to associated fractures.
Imaging
MRI is the modality of choice. Signal characteristics evolve with lesion age:
| Phase | T1 | T2 |
|---|---|---|
| Acute (<1 week) | Hypointense | Hyperintense |
| Subacute (1-6 weeks) | Hyperintense (homogeneous) | Hyperintense |
| Chronic (>6 weeks) | Variable | Variable, often with fat-fluid levels, peripheral enhancement, ± septations |
Chronic lesions may show a fibrous pseudocapsule, internal septations, and fat globules floating in a hemolymphatic collection. MRI also differentiates MLL from other diagnoses such as bursitis, hematoma, and soft-tissue sarcoma.
CT can identify large lesions on initial trauma workup. Ultrasound is useful for confirmation and guidance of aspiration.
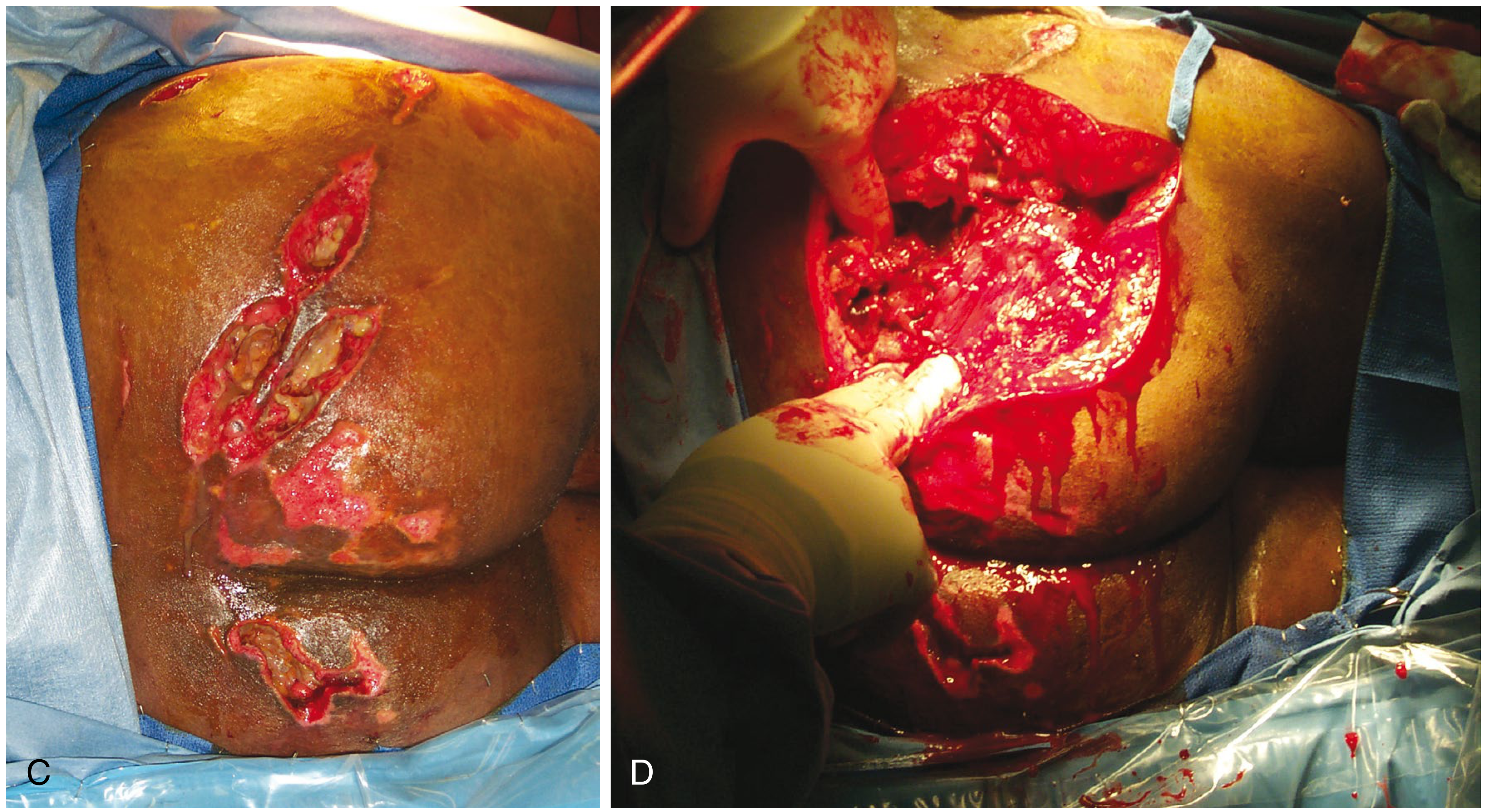
Clinical Images (from Campbell's Operative Orthopaedics 15th Ed 2026)
Figure 58.11A-B - Large Morel-Lavallée lesion of the thigh following pelvic fracture, showing extensive ecchymosis and swelling:

Figure 58.11C-D - Large MLL of the buttock (C) and operative exposure showing the depth of the lesion with necrotic fat and hematoma (D):
Management
No universally accepted guidelines exist. Treatment is guided by lesion size, chronicity, presence of capsule, and infection risk.
1. Conservative (Non-operative)
- Indicated for small, acute lesions with no fibrous capsule
- Compression bandaging, rest, observation
- Not effective for large or chronic/encapsulated lesions
2. Percutaneous Aspiration
- Useful for smaller lesions as a first step
- High recurrence rate - generally ineffective for chronic encapsulated lesions
3. Sclerotherapy
- Injection of a sclerosant (e.g., doxycycline, polidocanol, talc) into the cavity to obliterate the potential space
- Increasingly used; shows good results in literature for select cases
4. Percutaneous Surgical Drainage (Tseng-Tornetta Technique)
As described in Campbell's Operative Orthopaedics:
- Two 2-cm incisions over the distal and superior/posterior extents of the lesion
- Suction and debridement of loose fat and hematoma using a plastic brush
- Pulsed lavage until fluid is clear
- Closed-suction drain left in place (attached to wall suction until drainage <30 mL/24 hours - may require up to 8 days)
- Perioperative cephalosporin antibiotics for 24 hours after drain removal
This technique achieved good results in 19 patients when performed within 3 days of admission.
5. Open Debridement
- Reserved for large, chronic, infected, or recurrent lesions
- Higher risk of wound complications, including devascularization of overlying skin
- The preferred timing is simultaneous with fracture stabilization when surgical fixation is planned
- A 2024 case report demonstrated successful limited incisional debridement with wound drain and vacuum-assisted dressing, achieving good 1-year outcomes with minimal scarring
Key Decision Point
Collections >50 mL under an MLL are generally best treated surgically rather than by aspiration alone (Rockwood & Green's, 10th Ed 2025).
Complications
- Wound infection / surgical site infection - MLL is an independent risk factor, especially when internal fixation is planned
- Skin necrosis - acute or delayed, from vascular disruption
- Seroma recurrence - common after aspiration alone
- Chronic encapsulated collection - if untreated
- Nerve injury - decreased sensation from shearing of cutaneous nerves
Key Clinical Pearls
- Think about it with every pelvic/acetabular fracture - it is frequently missed when attention is focused on the bony injury
- Delayed presentation is common (33% present months-years later)
- Obesity is a risk factor - more subcutaneous tissue = larger potential space
- Do not operate through an untreated MLL - high risk of wound breakdown and infection after internal fixation
- MRI is confirmatory - use it before elective fixation to plan soft-tissue management
Sources:
- Campbell's Operative Orthopaedics, 15th Ed 2026, Chapter 58 (Technique 58.1, Fig. 58.11)
- Rockwood & Green's Fractures in Adults, 10th Ed 2025, Table 16-13
- Sarani N et al. "Morel-Lavallée lesion: What you need to know." J Trauma Acute Care Surg. 2026 - Systematic Review, PMID 40905976
- Nguyen PD et al. "Clinical Presentation, Imaging Features, and Management of Morel-Lavallee Lesions: A Scoping Review." Am Surg. 2026 - PMID 41126680
This is a shared conversation. Sign in to Orris to start your own chat.