Siderosis bulbi
Reading File
Finding Sources
Finding Sources
Searching PubMed
siderosis bulbi intraocular iron foreign body
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full clinical review:
Siderosis Bulbi
Definition
Siderosis bulbi (also called siderosis oculi) is a progressive degenerative condition of the eye caused by the retention of an iron-containing (ferrous) intraocular foreign body (IOFB). The iron undergoes electrolytic dissociation and deposits throughout the intraocular epithelial structures, where it exerts direct toxic effects on cellular enzyme systems, causing progressive cell death.
Etiology and Mechanism
- Cause: A retained ferrous IOFB - most commonly a steel fragment projected during hammering or power tool use
- Mechanism: The ferrous IOFB undergoes spontaneous dissociation in the ocular environment. Free iron ions deposit into epithelial structures and generate reactive oxygen species (Fenton reaction), disrupting cellular enzyme systems and leading to progressive cell death
- Structures affected: Lens epithelium, iris epithelium, ciliary body epithelium, and sensory retina (particularly the photoreceptors and RPE)
Clinical Features (Signs)
| Structure | Sign |
|---|---|
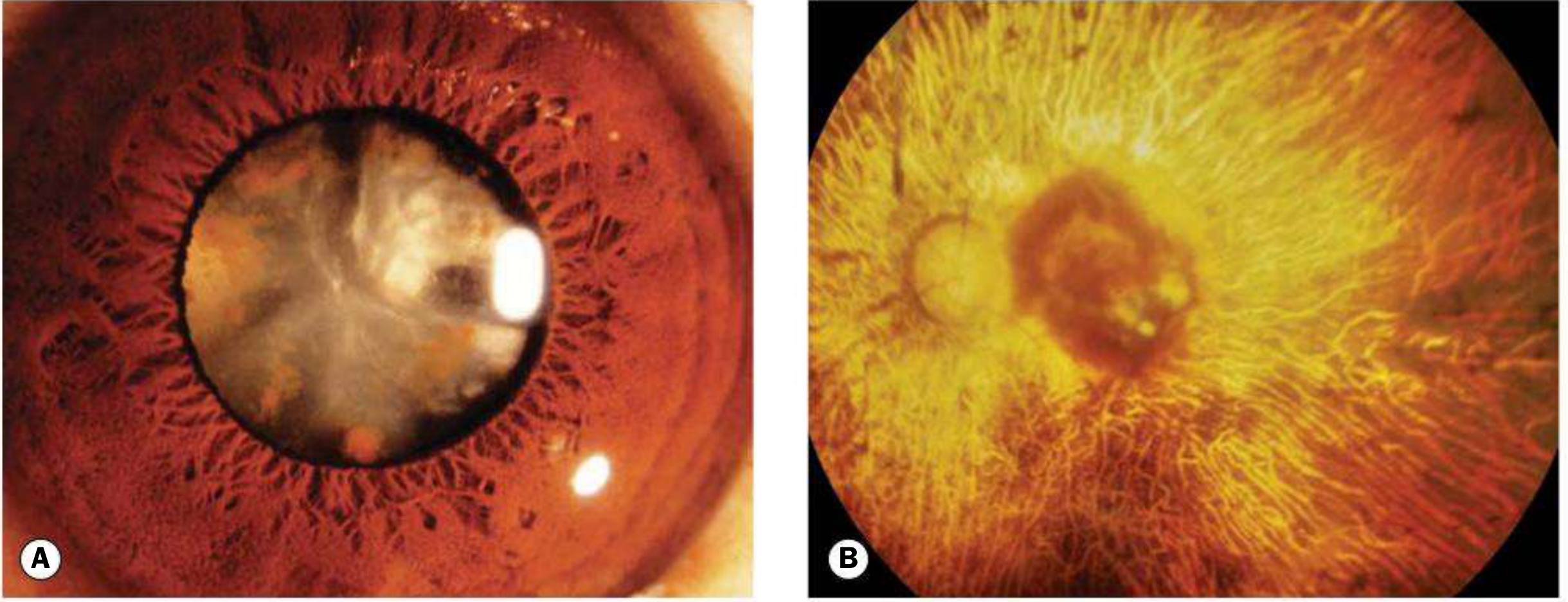
| Lens | Anterior capsular cataract with radially distributed iron deposits on the anterior lens capsule ("iron lines" or rust-colored deposits) |
| Iris | Reddish-brown staining of the iris → heterochromia iridis (the affected eye becomes darker/rust-colored) |
| Pupil | Dilated (iron mydriasis) - a classic and notable sign |
| Trabecular meshwork | Trabecular damage → secondary open-angle glaucoma |
| Retina/RPE | Pigmentary retinopathy → atrophy of the retina and RPE, potentially leading to profound, irreversible visual loss |
| ERG | Progressive attenuation of the b-wave on electroretinography (photoreceptor toxicity) - an early and sensitive marker |
The iris heterochromia and iron mydriasis may be subtle or missed in cases of an occult (unrecognized) IOFB.
Symptoms
- Gradual, painless deterioration of vision (often delayed - weeks to years after the original injury)
- Night blindness (early, due to rod photoreceptor toxicity)
- Constriction of visual fields
- History of ocular trauma is often present but may be forgotten
Investigations
- Slit-lamp examination - iris discoloration, anterior capsular deposits, pupil dilation
- Electroretinography (ERG) - progressive b-wave attenuation is the most sensitive early marker of retinal toxicity; used to monitor progression
- Plain X-ray - initial screening for radiopaque IOFB
- CT scan (axial + coronal) - gold standard for detecting and localizing a metallic IOFB; superior sensitivity and specificity compared to X-ray or ultrasound
- B-scan ultrasonography - useful when CT is unavailable or for posterior segment assessment
- MRI - CONTRAINDICATED when a ferrous metallic IOFB is suspected (risk of movement of the IOFB)
- Gonioscopy - assess trabecular iron deposition and glaucoma risk
Differential Diagnosis of the Heterochromia
- Fuchs heterochromic iridocyclitis
- Congenital iris heterochromia
- Iris nevus / melanoma
- Hemosiderosis (from old hyphema or vitreous hemorrhage)
- Pigment dispersion syndrome
Treatment
- Prompt surgical removal of the IOFB - the definitive treatment; prevents further iron dissociation
- Magnetic removal: Sclerotomy adjacent to the FB + application of a magnet, followed by cryotherapy to the retinal break
- Forceps removal (pars plana vitrectomy): For non-magnetic or poorly positioned FB, or those that cannot be safely extracted with a magnet
- Treat secondary glaucoma - topical IOP-lowering therapy or surgical intervention as needed
- Antibiotics - prophylaxis for endophthalmitis (open globe): ciprofloxacin 750 mg BD or moxifloxacin 400 mg OD, plus topical antibiotics and cycloplegia
- Serial ERG monitoring - if IOFB removal is delayed or not feasible, to track progressive retinal toxicity
Prognosis
- If the IOFB is removed early (before significant retinal damage), vision may be preserved or improved
- Delayed diagnosis leads to irreversible photoreceptor and RPE loss
- A missed ferrous IOFB is a common medicolegal pitfall - any patient with ocular trauma and unexplained progressive visual loss must be investigated
Siderosis vs. Chalcosis - Key Comparison
| Feature | Siderosis (Iron IOFB) | Chalcosis (Copper IOFB) |
|---|---|---|
| Foreign body | Iron/steel | Copper alloy (brass, bronze) |
| Iris | Rust-brown discoloration, heterochromia | Kayser-Fleischer ring |
| Lens | Anterior capsular rust deposits | "Sunflower" cataract |
| Retina | Pigmentary retinopathy, atrophy | Golden plaques; retina relatively spared |
| Visual outcome | Progressive, severe loss | Better preserved (copper less retinotoxic) |
| ERG | Progressive b-wave attenuation | Less severely affected |
| Endophthalmitis risk | Lower | High copper content → violent endophthalmitis → phthisis bulbi |
Source: Kanski's Clinical Ophthalmology - A Systematic Approach, 10th ed., pp. 942-943; Wills Eye Manual, 7th ed.; Localization in Clinical Neurology, 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.