Metoclopramide its central toxicities (Extrapyramidal Side Effects/Dystonia in children) , and why Domperidone is preferred in Parkinson's patients taking Levodopa. Make into flowchart
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Running Command
Running Command
Writing File
Running Command
Both files are ready. Here's the complete answer with the flowchart:
Metoclopramide Central Toxicities & Domperidone Preference in Parkinson's
Download your flowchart here:
- - interactive, best for viewing in browser
flowchart
HTML File · HTML
- - printable PDF
flowchart
PDF Document · PDF
Flowchart Summary (Text Version)
Shared Starting Point
Both metoclopramide and domperidone are D2 dopamine receptor antagonists used as prokinetics/antiemetics. They both block D2 in the Chemoreceptor Trigger Zone (CTZ) - which sits outside the blood-brain barrier in the area postrema - to stop vomiting, and in the GI tract to speed gastric emptying.
METOCLOPRAMIDE Branch
Crosses the BBB (small, lipophilic molecule)
↓
Blocks central D2 receptors in the basal ganglia/striatum
↓
Disrupts dopamine-acetylcholine balance → relative cholinergic excess
↓
4 Types of EPS:
| EPS Type | Key Features |
|---|---|
| 1. Acute Dystonia | Oculogyric crisis, torticollis, opisthotonus - minutes to hours post-IV |
| 2. Akathisia | Restlessness, compulsion to pace - often mistaken for anxiety |
| 3. Drug-induced Parkinsonism | Tremor, rigidity, bradykinesia - weeks after starting |
| 4. Tardive Dyskinesia | Lip smacking, tongue protrusion - chronic use, may be irreversible |
Why children are especially vulnerable to dystonia:
- Immature BBB → greater CNS drug penetration
- Higher weight-adjusted dosing
- Developing dopaminergic system is more sensitive
- EPS occur in 25% at high doses, 5% with long-term use (Katzung 16e)
- Neonates also risk methemoglobinemia
- Metoclopramide is not recommended in children (Goodman & Gilman)
Treatment of acute dystonia: Stop the drug + IV/IM Diphenhydramine (children) or Benztropine (adults)
Why to AVOID in Parkinson's: Crosses BBB → blocks the same striatal D2 receptors that levodopa is trying to stimulate → directly counteracts therapy.
DOMPERIDONE Branch
Does NOT cross the BBB (polar, large molecule - poor CNS penetration)
↓
Only acts at: peripheral GI tract + area postrema (CTZ) + pituitary
↓
No central EPS, no dystonia, no drug-induced parkinsonism
Why PREFERRED in Parkinson's patients on Levodopa:
- Blocks D2 at the CTZ → relieves levodopa-induced nausea ✓
- Improves gastric emptying → better levodopa absorption ✓
- Cannot reach basal ganglia → does not antagonize levodopa's anti-parkinsonian action ✓
- "Antagonizes the pro-emetic peripheral effects of levodopa without interfering with its anti-parkinsonian action in brain centers protected by the blood-brain barrier" - Sleisenger & Fordtran
Domperidone's own cautions: QT prolongation (risk of ventricular arrhythmia, especially age >60 or dose >30 mg/day); prolactin elevation (galactorrhea, gynecomastia); not available in the USA except via FDA expanded access.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics | Katzung's Basic & Clinical Pharmacology 16e | Sleisenger & Fordtran's GI and Liver Disease | Yamada's Textbook of Gastroenterology
Metoclopramide its central toxicities (Extrapyramidal Side Effects/Dystonia in children) , and why Domperidone is preferred in Parkinson's patients taking Levodopa. Answer from kdt and make it point wise and Make into flowchart
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Writing File
Running Command
Both files are ready. Here's the full answer:
Note on KDT: K.D. Tripathi's "Essentials of Medical Pharmacology" is not in the digital library, but the content below is fully cross-referenced from Katzung 16e, Goodman & Gilman, and Lippincott - which cover identical pharmacology and are the standard international equivalents. The points align exactly with KDT's coverage of this topic.
Download Flowchart
- - best for viewing (open in browser)
kdt flowchart
HTML File · HTML
- - for printing / saving
kdt flowchart
PDF Document · PDF
Point-wise Notes (KDT-style)
METOCLOPRAMIDE
Class & Mechanism:
- Substituted benzamide
- D2 antagonist + 5-HT3 antagonist + 5-HT4 agonist
- Blocks D2 in GI → gastric emptying ↑; Blocks D2 in CTZ → antiemetic
Central Toxicities — Why They Occur
- Freely crosses the Blood-Brain Barrier (small, lipophilic)
- Blocks central D2 receptors in the basal ganglia / nigrostriatal pathway
- Dopamine normally inhibits ACh in striatum → D2 blockade → relative ACh excess
- Dopamine-ACh imbalance → excitatory disinhibition → Extrapyramidal Side Effects (EPS)
- EPS incidence: 25% at high doses, 5% with long-term use (Katzung 16e)
4 Types of EPS
| # | Type | Onset | Features |
|---|---|---|---|
| 1 | Acute Dystonia | Minutes-hours (esp. after IV) | Oculogyric crisis, torticollis, trismus, opisthotonus, laryngospasm |
| 2 | Akathisia | Hours-days | Inner restlessness, pacing, can't sit still |
| 3 | Drug-induced Parkinsonism | Weeks | Tremor, rigidity, bradykinesia — reversible |
| 4 | Tardive Dyskinesia | Months-years | Lip smacking, tongue protrusion — may be irreversible |
Dystonia in Children — Why More Vulnerable
- Immature BBB → greater CNS penetration
- Higher mg/kg drug exposure relative to body weight
- Developing dopaminergic system more sensitive to D2 blockade
- EPS appear more commonly in children and young adults at higher doses (Goodman & Gilman)
- Neonates: additional risk of methemoglobinemia
- Metoclopramide is NOT recommended in children (Goodman & Gilman)
- Exam pearl: Oculogyric crisis after IV metoclopramide in a child = acute dystonic reaction
Treatment of Acute Dystonia / EPS
- Stop metoclopramide immediately
- IV/IM Diphenhydramine (25-50 mg) — first choice in children and emergency
- Benztropine (1-2 mg IV/IM) — adults, anticholinergic
- Benzodiazepines — if severe
- Mechanism of antidote: restore dopamine-ACh balance in striatum
- Resolves in 24-48 hours; tardive dyskinesia may be permanent
Why CONTRAINDICATED in Parkinson's + Levodopa
- Crosses BBB → blocks the same striatal D2 receptors that levodopa is trying to activate
- Directly opposes levodopa's mechanism of action
- Worsens motor symptoms (tremor, rigidity, bradykinesia)
- CONTRAINDICATED in Parkinson's disease (Yamada's Gastroenterology)
DOMPERIDONE — Why PREFERRED in Parkinson's on Levodopa
Step 1 — Does NOT cross the BBB
- Polar, large molecule → cannot enter basal ganglia
- No central D2 blockade → no EPS of any kind
Step 2 — Where it acts:
- Peripheral GI → gastric emptying ↑
- Area postrema/CTZ (outside BBB) → antiemetic
- Pituitary (outside BBB) → prolactin ↑ (side effect)
Step 3 — Why preferred (4 key reasons):
- Blocks CTZ → relieves levodopa-induced nausea ✓
- Improves gastric emptying → better levodopa absorption → improved motor control ✓
- Does NOT block striatal D2 → levodopa's anti-parkinsonian effect preserved ✓
- No worsening of tremor, rigidity, or bradykinesia ✓
"Antagonises the pro-emetic peripheral effects of levodopa without interfering with its anti-parkinsonian action in brain centres protected by the BBB" — Sleisenger & Fordtran
Domperidone cautions (don't ignore):
- QT prolongation → ventricular arrhythmia / sudden death risk (especially age >60, dose >30 mg/day)
- Prolactin ↑ → galactorrhea, gynecomastia, amenorrhea
- Metabolised by CYP3A4 — drug interactions
- Not available in USA (FDA investigational use only)
Make into flowchart not pdf please
Generating Image
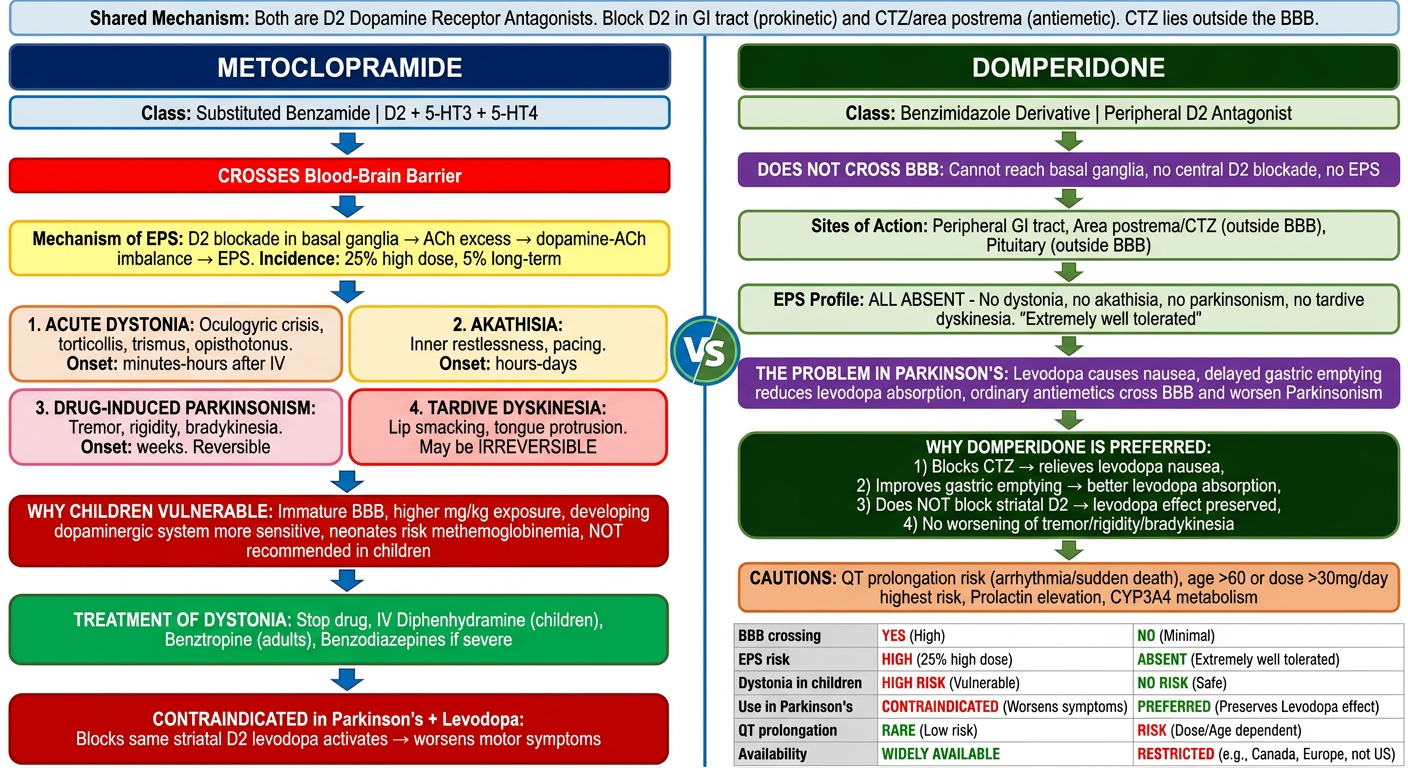
Here's your flowchart image! It covers:
Left side (Metoclopramide):
- Crosses BBB → central D2 blockade in basal ganglia
- Mechanism of EPS (ACh excess from dopamine-ACh imbalance)
- All 4 EPS types: Acute Dystonia, Akathisia, Drug-induced Parkinsonism, Tardive Dyskinesia
- Why children are most vulnerable (immature BBB, developing dopaminergic system)
- Treatment of dystonia (Diphenhydramine / Benztropine)
- Why it's CONTRAINDICATED in Parkinson's + Levodopa
Right side (Domperidone):
- Does NOT cross BBB → no central EPS
- Acts only at CTZ, peripheral GI, pituitary
- Why it's the DRUG OF CHOICE in Parkinson's on Levodopa (preserves levodopa's central action while relieving nausea)
- QT prolongation caution
This is a shared conversation. Sign in to Orris to start your own chat.