Melanoma
Reading File
Finding Sources
Searching PubMed
melanoma treatment immunotherapy targeted therapy
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Here is a comprehensive overview of Melanoma (Malignant Melanoma) drawn from authoritative dermatology and surgery textbooks.
Melanoma (Malignant Melanoma)
Definition & Origin
Melanoma is a malignant tumor arising from melanocytes - pigment-producing cells located primarily at the dermal-epidermal junction (DEJ). Almost half arise from preexisting nevi, but the majority develop on previously normal-appearing skin. Typically there is a prolonged, radially oriented growth phase before a vertical growth phase develops (which marks invasive potential and risk of metastasis). - Andrews' Diseases of the Skin, p. 315
Risk Factors
-
Light complexion, light eyes, blond or red hair
-
History of blistering sunburns in childhood
-
Poor tanning ability, easy sunburning
-
Large number of common nevi or clinically dysplastic nevi
-
Family history of melanoma
-
Mutations in BRAF gene (nonchronically sun-exposed skin in Caucasians)
-
KIT gene mutations and cyclin D1/CDK4 amplifications (acral and mucosal lentiginous types)
-
PUVA therapy, tanning lamps, xeroderma pigmentosum, immunodeficiency
-
Giant congenital nevi (axial), p16/CDK4 gene mutations
-
Andrews' Diseases of the Skin, p. 326
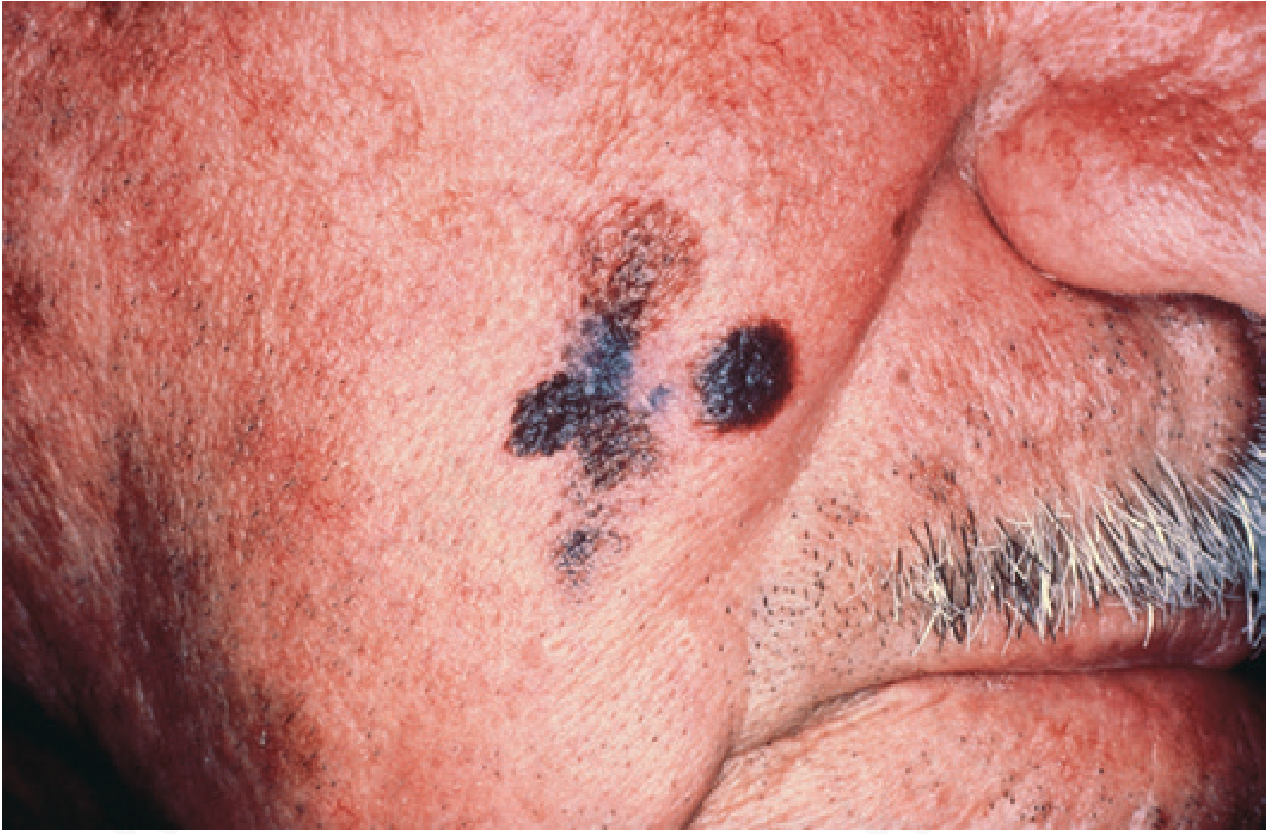
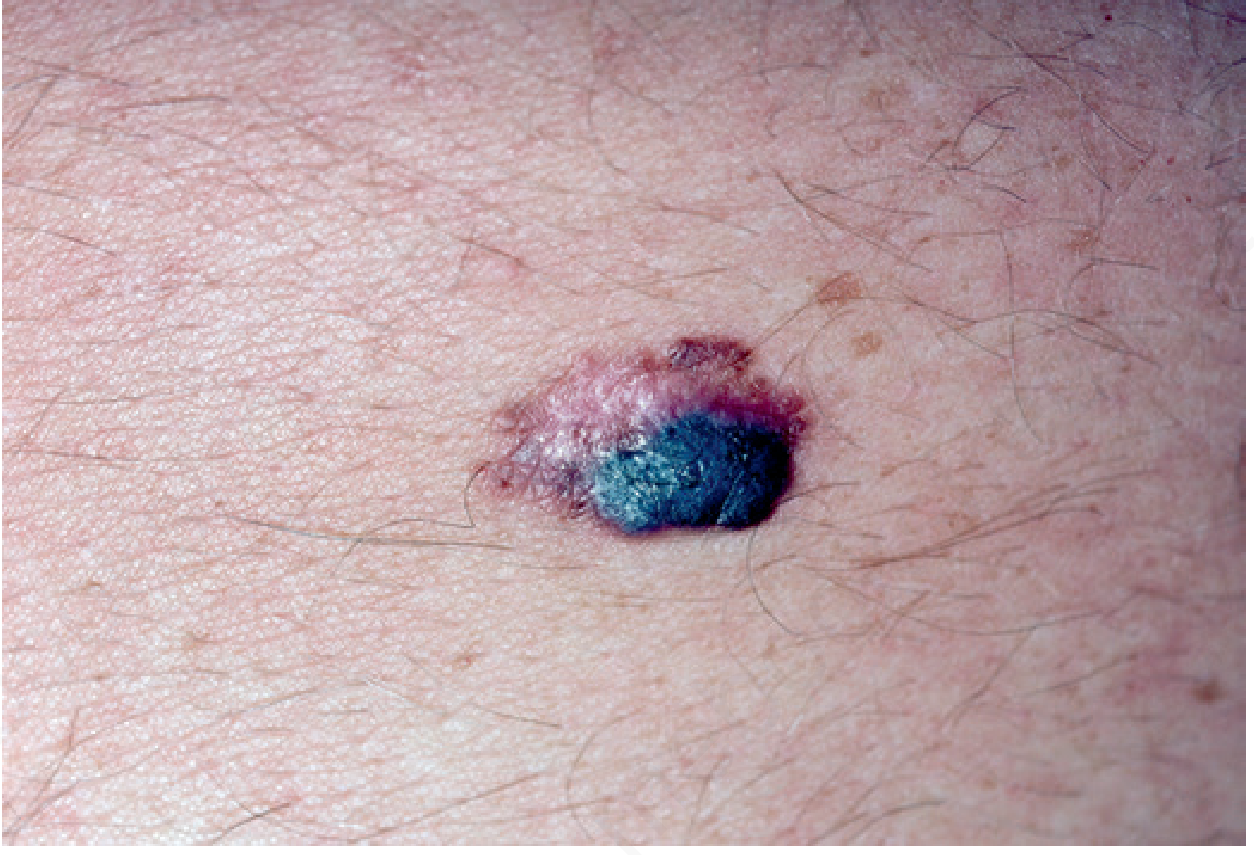
Clinical Recognition - The ABCDE Criteria
| Letter | Feature |
|---|---|
| A | Asymmetry |
| B | Border irregularity |
| C | Color variegation |
| D | Diameter > 6 mm |
| E | Evolution (change over time) |
Amelanotic lesions appear as raised pink, purple, or flesh-colored papules and are frequently diagnosed late. - Schwartz's Principles of Surgery, p. 2550
Subtypes / Clinicopathologic Types
1. Lentigo Maligna Melanoma
Begins as a tan macule on sun-damaged skin in older patients, extending peripherally with gradual darkening over 5-20 years. After a prolonged radial growth phase, a vertical growth phase develops. May appear increasingly common and some data suggest it is now the most frequent form.
2. Superficial Spreading Melanoma
The most common type in Caucasians. Predominantly radial growth phase.
3. Acral-Lentiginous Melanoma
Found on palmar, plantar, and subungual surfaces. Accounts for 29-72% of melanomas in dark-skinned individuals. Not associated with sun exposure.
4. Nodular Melanoma
Vertical growth phase predominates from the outset. More aggressive behavior.
5. Desmoplastic Melanoma
May appear as a papule, firm plaque, or inconspicuous area of induration; associated with lentiginous types.
6. Other Types
Mucosal melanoma, ocular melanoma, primary CNS melanoma, primary soft tissue malignant melanoma.
- Andrews' Diseases of the Skin, p. 336
Diagnosis & Staging
Biopsy: Suspicious lesions should undergo excisional biopsy with 1-3 mm margins. Large or anatomically difficult lesions may undergo incisional or punch biopsy. Tissue must include full thickness down to subcutis.
Key Prognostic Factors:
- Breslow thickness - the single most important prognostic indicator (replaces Clark's level in modern staging); measures depth from top of granular layer into dermis
- Tumor ulceration
- Mitotic rate ≥ 1/mm²
- Lymph node involvement (number of positive nodes most important in stage III)
- For stage IV: site of metastasis + elevated LDH (worse prognosis)
AJCC Staging:
| Stage | Disease |
|---|---|
| I-II | Localized |
| III | Regional (nodal) |
| IV | Distant metastatic |
Imaging: CT of chest/abdomen/pelvis, whole-body PET-CT, and brain MRI are recommended for stage III or higher disease. No role for routine chest X-ray or CT in early-stage (node-negative) disease. - Schwartz's Principles of Surgery, p. 2568-2577
Sentinel Lymph Node Biopsy (SLNB)
SLNB was introduced in 1992 and is now a cornerstone of melanoma staging for clinically node-negative disease. The technique involves:
- Preoperative lymphoscintigraphy with intradermal technetium-sulfur colloid
- Intraoperative injection of isosulfan or methylene blue dye near the tumor
- Excision of the first draining lymph node
- Pathology with H&E + immunohistochemistry (S100, HMB45, MART-1/Melan-A)
The radioactive tracer-dye combination identifies the sentinel node in 98% of cases. SLNB should be offered for lesions > 1.2 mm and for thin lesions with high-risk features (thickness > 0.75 mm, ulceration, mitoses ≥ 1/mm²). - Schwartz's Principles of Surgery, p. 2579
Treatment
Surgical - Wide Local Excision
Primary curative treatment. Excision margins depend on Breslow depth:
- In situ: 5 mm margin standard (though lentiginous types often extend subclinically beyond this)
- Invasive: wider margins (up to 2 cm) guided by thickness
Regional Disease
- Isolated Limb Perfusion (ILP): Hyperthermic ILP with melphalan achieves a 63% complete response rate for unresectable in-transit disease
- Isolated Limb Infusion (ILI): Provides ~31% response rate with less morbidity
Radiotherapy
- Used for palliation of unresectable lesions
- Adjuvant radiation may benefit patients at high risk for local/regional failure (thickness > 4 mm, ulceration, satellitosis, positive margins, desmoplastic histology, perineural invasion)
- Melanoma is treated with hypofractionated radiation: fraction sizes of 4-6 Gy (e.g., 30 Gy in 5 fractions)
- Note: recurrence risk after radiation is significantly higher than for squamous or basal cell carcinoma
Systemic Therapy
| Agent | Mechanism | Notes |
|---|---|---|
| BRAF inhibitors (vemurafenib, dabrafenib) | Target BRAF V600E mutation | First-line for BRAF-mutant melanoma |
| MEK inhibitors (trametinib) | Target downstream MAPK pathway | Often combined with BRAF inhibitors |
| Ipilimumab | Anti-CTLA-4 antibody | Immune checkpoint inhibitor |
| Pembrolizumab / Nivolumab | Anti-PD-1 antibodies | Major survival benefit in metastatic disease |
| High-dose IL-2 | Cytokine immunotherapy | Selected patients only |
| High-dose Interferon (IFN) | Adjuvant therapy | Improves DFS in melanoma > 4 mm; pooled analyses did not show overall survival benefit |
A recent 2024 network meta-analysis (PMID 39684531) found that combined targeted + immune therapy offers additional advantages over monotherapy in advanced melanoma, though at increased toxicity.
Metastatic Disease
- Most common metastatic sites: lung, liver, followed by brain, GI tract, distant skin, subcutaneous tissue
- Limited small-volume brain/GI/distant skin metastases: surgical resection or directed radiation
- Liver metastases: generally not resected unless from ocular primary
- Stereotactic radiosurgery (SRS) for brain metastases, often combined with immunotherapy or targeted therapy - a 2024 systematic review (PMID 39097248) confirms SRS + immunotherapy provides superior outcomes in melanoma brain metastases
Prognosis
- Depth of invasion (Breslow thickness) is the single greatest predictor of metastatic risk
- Ulceration and high mitotic rate worsen prognosis
- Stage IV 5-year survival was historically < 10%, but modern immunotherapy and targeted therapy have significantly improved outcomes
- Melanoma occurring during pregnancy has a shorter disease-free interval after excision but no adverse effect on overall survival
Sources: Andrews' Diseases of the Skin (Clinical Dermatology), Fitzpatrick's Dermatology (Volumes 1 & 2), Schwartz's Principles of Surgery (11th ed.), Textbook of Family Medicine (9th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.