Tell me all drugs that include in gynaecology and obstetrics for table viva
Drugs in Gynaecology & Obstetrics - Table Viva Guide
1. UTEROTONICS (Drugs that stimulate uterine contractions)
| Drug | Class | Mechanism | Uses | Key Side Effects |
|---|---|---|---|---|
| Oxytocin | Posterior pituitary hormone | Binds oxytocin receptors (Gq-PLC-IP3) → ↑ intracellular Ca²⁺ → myometrial contraction | Induction/augmentation of labor, PPH prevention, 3rd stage management | Hypotension, water intoxication (antidiuretic effect), fetal distress, uterine hyperstimulation |
| Ergometrine (Ergonovine) | Ergot alkaloid | α-adrenergic + 5-HT receptor agonist → sustained tonic uterine contraction | PPH (3rd stage), subinvolution | Hypertension, nausea, vomiting - CONTRAINDICATED in hypertension/pre-eclampsia |
| Methylergometrine (Methergine) | Ergot alkaloid | Same as ergometrine | PPH, 3rd stage | Same as ergometrine |
| Misoprostol (PGE₁ analogue) | Prostaglandin | PGE₁ receptor → ↑ Ca²⁺ in myometrium | Cervical ripening, induction, PPH, MTP | Diarrhea, fever, shivering, hyperstimulation |
| Carboprost (15-methyl PGF₂α) | Prostaglandin | FP receptor → uterine contraction | Refractory PPH, MTP (2nd trimester) | Bronchospasm - CONTRAINDICATED in asthma |
| Dinoprostone (PGE₂) | Prostaglandin | PGE₂ receptor | Cervical ripening, induction, MTP | Hypotension, fever, GI upset |
| Carbetocin | Oxytocin analogue (long-acting) | Same as oxytocin but longer half-life (~40 min vs 4-6 min) | PPH prevention in C-section | Similar to oxytocin, less water retention |
2. TOCOLYTICS (Drugs that inhibit uterine contractions)
| Drug | Class | Mechanism | Notes |
|---|---|---|---|
| Ritodrine | β₂-adrenergic agonist | ↑ cAMP → PKA → phosphorylates/inactivates MLCK | Only tocolytic with FDA approval; withdrawn from US market |
| Terbutaline | β₂-adrenergic agonist | Same as ritodrine | Used off-label; SC/IV/oral; delays birth only first 48h; causes maternal tachycardia, hypotension, pulmonary edema |
| Nifedipine | Ca²⁺ channel blocker | Blocks voltage-sensitive Ca²⁺ channels → ↓ MLCK activation | First-line tocolytic; better fetal outcomes, fewer maternal side effects than β₂ agonists |
| Indomethacin | COX inhibitor (NSAID) | Inhibits PG synthesis → ↓ PGF₂α-driven contraction | Used <32 weeks; risk of premature closure of ductus arteriosus, oligohydramnios |
| Atosiban | Oxytocin receptor antagonist | Blocks OXTR → prevents IP3/Ca²⁺ signaling | Licensed in Europe; fewer cardiovascular side effects |
| Magnesium sulfate (MgSO₄) | Inorganic salt | Competes with Ca²⁺, blocks Ca²⁺ influx; also neuroprotective for fetus | Also used in eclampsia prophylaxis/treatment; monitor for toxicity (loss of reflexes, respiratory depression) |
| NO donors (e.g., GTN patches) | Nitric oxide donor | ↑ cGMP → PKG → MLCK inactivation | Experimental; riociguat (sGC activator) is CONTRAINDICATED in pregnancy |
3. DRUGS FOR PRE-ECLAMPSIA / ECLAMPSIA
| Drug | Use | Key Point |
|---|---|---|
| Magnesium sulfate | Eclampsia seizure prophylaxis & treatment | Gold standard; Pritchard or Zuspan regimen; antidote = calcium gluconate |
| Labetalol | Acute severe hypertension in pregnancy | α+β blocker; IV preferred |
| Hydralazine | Acute severe hypertension | Direct arteriolar dilator; IV bolus or infusion |
| Nifedipine (oral) | Acute severe hypertension | Avoid sublingual (precipitous BP drop) |
| Methyldopa | Chronic hypertension in pregnancy | Drug of choice for chronic HTN in pregnancy |
| Clonidine | Chronic hypertension | Central α₂ agonist; second-line |
| Amlodipine | Chronic hypertension | Ca²⁺ channel blocker; safe in pregnancy |
- ACE inhibitors (captopril, enalapril) - fetal renal agenesis, oligohydramnios
- ARBs - same as ACE inhibitors
- Atenolol - fetal growth restriction
- Nitroprusside - cyanide toxicity to fetus (avoid prolonged use)
4. DRUGS FOR MEDICAL TERMINATION OF PREGNANCY (MTP)
| Regimen | Drug | Dose | Gestational Age |
|---|---|---|---|
| 1st trimester | Mifepristone (RU-486) 200 mg oral + Misoprostol 800 mcg vaginal/sublingual (48h later) | Most effective <9 weeks | |
| 1st trimester surgical prep | Misoprostol alone | Cervical priming before MVA | |
| 2nd trimester | Mifepristone + Misoprostol or Carboprost (PGF₂α) | 13-24 weeks | |
| Mifepristone | Antiprogestogen; blocks progesterone receptors → sensitizes uterus to prostaglandins | - |
5. HORMONAL CONTRACEPTIVES
Combined Oral Contraceptive Pill (COCP)
- Estrogen component: Ethinylestradiol (EE) 20-35 mcg (low dose)
- Progestogen components: Levonorgestrel, Norethisterone, Desogestrel, Gestodene, Norgestimate, Drospirenone
Progestogen-Only Pill (POP / Mini-pill)
- Desogestrel 75 mcg (most effective POP - inhibits ovulation)
- Levonorgestrel 30 mcg, Norethisterone 350 mcg
Injectables
- Depot medroxyprogesterone acetate (DMPA / Depo-Provera): 150 mg IM every 3 months
- Norethisterone enantate: 200 mg IM every 2 months
Implants
- Etonogestrel implant (Nexplanon/Implanon): Subdermal, 3 years, most effective reversible method
Emergency Contraception
| Drug | Dose | Window | Mechanism |
|---|---|---|---|
| Levonorgestrel (Plan B) | 1.5 mg oral single dose | Within 72h (up to 120h) | Delays/inhibits ovulation |
| Ulipristal acetate (EllaOne) | 30 mg oral | Within 120h | Selective progesterone receptor modulator |
| Cu-IUD | Insertion | Within 120h | Most effective EC (>99%); also ongoing contraception |
Intrauterine Devices
- Levonorgestrel IUS (Mirena): 52 mg LNG, releases 20 mcg/day; 5-8 years; reduces menorrhagia
- Copper IUD (Cu-T 380A): Non-hormonal; 10 years; Cu ions toxic to sperm
6. DRUGS FOR ENDOMETRIOSIS
| Drug | Class | Mechanism | Use |
|---|---|---|---|
| GnRH agonists (Leuprolide, Goserelin, Buserelin) | GnRH analogue | Downregulate pituitary GnRH receptors → ↓ FSH/LH → medical castration | Endometriosis, fibroids, IVF |
| Danazol | Androgen derivative | Inhibits gonadotrophins; androgenic/anabolic | Endometriosis, menorrhagia; causes virilization, weight gain |
| Progestogens (MPA, norethisterone, dienogest) | Progestogen | Decidualization → atrophy of endometriotic implants | First-line hormonal Rx |
| COCP | Combined OC | Suppresses endometrium, reduces retrograde menstruation | Mild-moderate endometriosis |
| LNG-IUS (Mirena) | Intrauterine progestogen | Local endometrial suppression | Endometriosis-associated menorrhagia |
| Letrozole | Aromatase inhibitor | ↓ local estrogen production in endometriotic tissue | Recurrent/refractory cases |
7. DRUGS FOR POLYCYSTIC OVARY SYNDROME (PCOS)
| Drug | Use | Mechanism |
|---|---|---|
| Metformin | Insulin resistance; restore ovulation | Activates AMPK → ↓ hepatic glucose production, ↑ insulin sensitivity |
| Clomiphene citrate | Ovulation induction | Competitive estrogen receptor antagonist at hypothalamus → ↑ GnRH/FSH/LH |
| Letrozole | Ovulation induction (1st line) | Aromatase inhibitor → ↑ FSH via negative feedback; superior to clomiphene in PCOS |
| Gonadotrophins (FSH/hMG) | Ovulation induction | Direct ovarian stimulation; risk of OHSS |
| COCP | Symptom control (hirsutism, menstrual irregularity) | Suppresses androgens, regulates cycle |
| Spironolactone | Anti-androgen (hirsutism/acne) | Blocks androgen receptors; also aldosterone antagonist |
| Cyproterone acetate | Anti-androgen | Androgen receptor blocker; component of Diane-35 |
8. DRUGS FOR MENORRHAGIA
| Drug | Mechanism | Notes |
|---|---|---|
| Tranexamic acid | Antifibrinolytic (inhibits plasminogen activation) | Non-hormonal; reduces blood loss ~50% |
| Mefenamic acid | COX inhibitor (NSAID) | Reduces PG-driven vasodilation; also dysmenorrhea |
| LNG-IUS (Mirena) | Local progestogen → endometrial atrophy | Most effective medical treatment |
| COCP | Endometrial suppression | Regular cycles, reduced blood loss |
| Norethisterone | Progestogen | 5 mg TDS day 5-26; used for cycle control |
| Danazol | Androgen derivative | Endometrial atrophy; significant side effects |
9. DRUGS IN INFERTILITY / ART
| Drug | Use | Notes |
|---|---|---|
| Clomiphene citrate | Ovulation induction | Anti-estrogen; 50-150 mg day 2-6; SERM |
| Letrozole | Ovulation induction (PCOS preferred) | Aromatase inhibitor; fewer multiple pregnancies |
| FSH (Follitropin α/β) | Controlled ovarian hyperstimulation | Gonal-F, Puregon; monitor for OHSS |
| hMG (Menotropin) | Ovarian stimulation | FSH + LH; Merional, Menopur |
| GnRH agonists | Pituitary downregulation in IVF | Leuprolide, Buserelin; "long protocol" |
| GnRH antagonists | Prevent premature LH surge | Cetrorelix, Ganirelix; "antagonist protocol" - more convenient |
| hCG (Choriogonadotropin) | Trigger ovulation (LH surge mimic) | Given when follicle ≥18 mm; also luteal support |
| Progesterone | Luteal phase support | Vaginal gel (Crinone), pessaries; post IVF/embryo transfer |
| Cabergoline | Hyperprolactinemia | D₂ agonist; reduces prolactin; first-line over bromocriptine |
| Bromocriptine | Hyperprolactinemia | D₂ agonist; older drug, more side effects |
10. CORTICOSTEROIDS IN OBSTETRICS
| Drug | Indication | Dose | Effect |
|---|---|---|---|
| Betamethasone | Antenatal corticosteroid (ACS) | 12 mg IM x2 doses, 24h apart | Fetal lung maturation (induces surfactant); reduces RDS, IVH, NEC - given 24-34 weeks when preterm birth expected within 7 days |
| Dexamethasone | Alternative to betamethasone | 6 mg IM x4 doses, 12h apart | Same; preferred if betamethasone unavailable; also used in HELLP syndrome |
| Hydrocortisone | Addisonian crisis in pregnancy | Stress dosing | - |
11. ANTIEMETICS IN PREGNANCY (Nausea/Vomiting/Hyperemesis Gravidarum)
| Drug | Class | Safety |
|---|---|---|
| Pyridoxine (Vitamin B6) | Vitamin | First-line; safe in 1st trimester |
| Doxylamine + Pyridoxine (Diclegis/Bonjesta) | Antihistamine + B6 | FDA Category B; first-line combination |
| Metoclopramide | D₂ antagonist (prokinetic) | Safe; IV for hyperemesis |
| Ondansetron | 5-HT₃ antagonist | Widely used; small risk of cardiac septal defects if used in 1st trimester (controversial) |
| Prochlorperazine | Phenothiazine | Second-line |
| Promethazine | Antihistamine | Sedating; second-line |
| Thiamine (Vit B1) | Vitamin | MANDATORY in hyperemesis before IV dextrose (prevents Wernicke's encephalopathy) |
12. DRUGS FOR GESTATIONAL DIABETES
| Drug | Notes |
|---|---|
| Insulin | Gold standard; all types safe (NPH, aspart, lispro, glargine) |
| Metformin | Used in some guidelines (NICE); crosses placenta but safe evidence accumulating |
| Glibenclamide (Glyburide) | Used in some countries; crosses placenta more than metformin - not preferred |
13. ANTIBIOTICS SAFE IN PREGNANCY
| Safe | Use with Caution | Contraindicated |
|---|---|---|
| Penicillins (amoxicillin, ampicillin) | Metronidazole (avoid 1st trimester - limited data) | Tetracyclines (teeth/bone) |
| Cephalosporins | Clindamycin | Fluoroquinolones (cartilage damage) |
| Azithromycin | Vancomycin (ototoxicity) | Aminoglycosides (ototoxicity) - avoid if possible |
| Nitrofurantoin (avoid at term - haemolysis) | - | Trimethoprim (folate antagonist - avoid 1st trimester) |
| Clindamycin (BV in pregnancy) | - | Chloramphenicol (grey baby syndrome at term) |
14. DRUGS FOR CERVICAL RIPENING / INDUCTION
| Drug | Route | Notes |
|---|---|---|
| Dinoprostone (PGE₂) | Vaginal gel/pessary | Bishop score <6; contraindicated in previous CS (uterine rupture risk) |
| Misoprostol (PGE₁) | Vaginal/sublingual/oral | Cheaper; used cautiously in previous CS |
| Oxytocin | IV infusion | When cervix favorable (Bishop ≥6); titrated infusion |
| Mifepristone | Oral | Cervical ripening; sensitizes uterus to PGs |
| Mechanical methods | Foley catheter, balloon | Non-pharmacological; reduces hyperstimulation risk |
15. ANTIFIBRINOLYTICS & HAEMOSTATICS IN OBSTETRICS
| Drug | Use | Dose |
|---|---|---|
| Tranexamic acid | PPH treatment | 1g IV slowly; repeat after 30 min if needed; within 3h of birth (WOMAN trial) |
| Fibrinogen concentrate | PPH with DIC | Replaces fibrinogen when <2 g/L |
| Fresh frozen plasma (FFP) | Coagulopathy in PPH | 10-15 mL/kg |
16. DRUGS FOR VULVOVAGINAL INFECTIONS
| Condition | Drug of Choice | Alternative |
|---|---|---|
| Bacterial vaginosis | Metronidazole 400 mg oral BD x5d | Clindamycin vaginal cream |
| Candidiasis | Clotrimazole 500 mg vaginal pessary (single) or Fluconazole 150 mg oral | Miconazole vaginal cream |
| Trichomoniasis | Metronidazole 2g oral single dose (+ treat partner) | Tinidazole 2g |
| Chlamydia | Azithromycin 1g single dose | Doxycycline 100 mg BD x7d (avoid in pregnancy) |
| Gonorrhoea | Ceftriaxone 500 mg IM single dose | - |
| Genital herpes | Aciclovir 200-400 mg TDS | Valaciclovir |
| Syphilis | Benzathine penicillin G 2.4 MU IM | Erythromycin (if penicillin allergy in pregnancy) |
17. DRUGS FOR GYNAECOLOGICAL CANCERS
| Drug/Class | Indication |
|---|---|
| Paclitaxel + Carboplatin | Ovarian cancer (first-line) |
| Bevacizumab (anti-VEGF) | Ovarian cancer (add-on/maintenance) |
| PARP inhibitors (Olaparib, Niraparib, Rucaparib) | BRCA-mutated ovarian cancer maintenance |
| Cisplatin + Radiotherapy | Cervical cancer (concurrent chemoradiation) |
| 5-Fluorouracil (topical) | VIN/VAIN |
| Imiquimod (topical) | HPV-related VIN, condylomata |
| Medroxyprogesterone acetate | Endometrial cancer (low grade, fertility-sparing) |
| Tamoxifen | Breast cancer (ER+); note: increases endometrial cancer risk |
QUICK RECALL TABLE - Drug Classes & Prototype
| Category | Prototype Drug |
|---|---|
| Uterotonic (oxytocic) | Oxytocin |
| Ergot oxytocic | Ergometrine |
| PG uterotonic | Carboprost (PGF₂α) |
| Tocolytic (β₂ agonist) | Terbutaline |
| Tocolytic (Ca²⁺ blocker) | Nifedipine |
| Tocolytic (OT antagonist) | Atosiban |
| Anti-eclamptic | MgSO₄ |
| Antenatal corticosteroid | Betamethasone |
| MTP drug | Mifepristone + Misoprostol |
| COCP progestogen | Levonorgestrel |
| Emergency contraceptive | Levonorgestrel |
| Ovulation induction | Clomiphene citrate / Letrozole |
| Hyperprolactinemia | Cabergoline |
| Endometriosis (medical) | GnRH agonist (Leuprolide) |
| Menorrhagia (non-hormonal) | Tranexamic acid |
| PPH (refractory) | Carboprost |
| Hyperemesis gravidarum | Pyridoxine + Doxylamine |
Create a visual flowchart for drug selection in infertility management
A detailed medical flowchart titled "Drug Selection in Infertility Management" with a clean clinical white background. The flowchart starts at the top with "INFERTILITY WORKUP COMPLETE" box, then branches into multiple pathways: LEFT BRANCH - "ANOVULATION / OVULATORY DYSFUNCTION" leading down to: - PCOS box → "1st Line: Letrozole 2.5-5mg (Day 2-6)" → "2nd Line: Clomiphene Citrate 50-150mg" → "Add Metformin if insulin resistant" → "3rd Line: Gonadotrophins (FSH/hMG)" → "Laparoscopic Ovarian Drilling" MIDDLE BRANCH - "HYPERPROLACTINEMIA" leading to: - "Cabergoline 0.25-0.5mg twice weekly" → "Bromocriptine (if cabergoline unavailable)" → "Normalize prolactin → reassess ovulation" RIGHT BRANCH - "HYPOGONADOTROPHIC HYPOGONADISM" leading to: - "Pulsatile GnRH (gold standard)" → "OR Gonadotrophins: FSH + hCG" BOTTOM SECTION - "ASSISTED REPRODUCTIVE TECHNOLOGY (ART / IVF)" large box containing: - Controlled Ovarian Hyperstimulation protocols side by side: LEFT: "LONG PROTOCOL: GnRH Agonist (Leuprolide/Buserelin) Day 21 → Downregulation → FSH injections" RIGHT: "ANTAGONIST PROTOCOL: FSH from Day 2 → GnRH Antagonist (Cetrorelix/Ganirelix) when follicle ≥14mm" - Both lead to: "Trigger Shot: hCG 10,000 IU or GnRH Agonist (antagonist protocol)" - Then: "Oocyte Retrieval → Fertilisation → Embryo Transfer" - Then: "Luteal Phase Support: Progesterone vaginal pessaries/gel" SPECIAL BOXES on the side: - "OHSS PREVENTION: Cabergoline, GnRH agonist trigger, freeze-all strategy" - "MALE FACTOR: Gonadotrophins (FSH+hCG) if hypogonadotrophic" Color coding: Blue boxes for diagnosis, Green boxes for first-line drugs, Orange for second-line, Red for warnings/contraindications. Arrows connecting all steps. Professional medical textbook style.
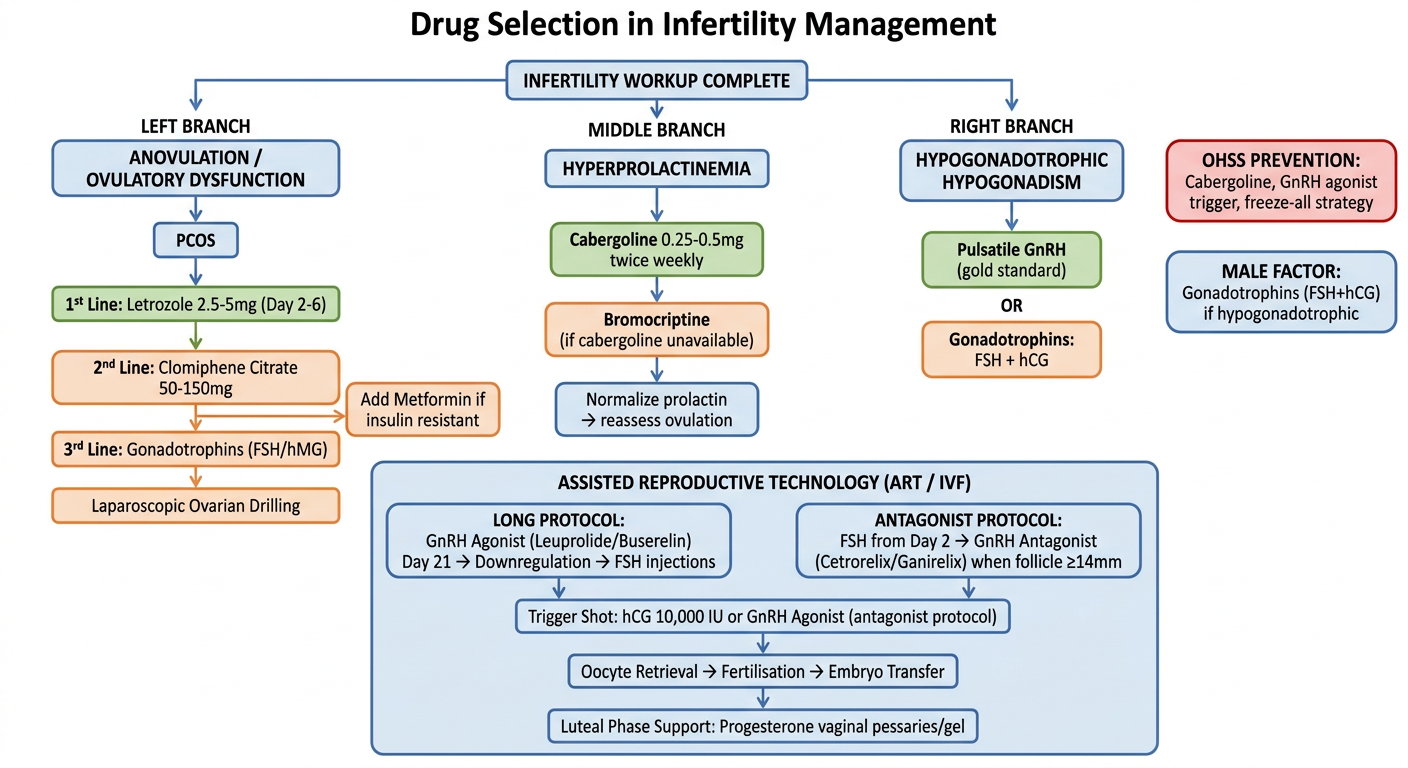
Flowchart Logic - Drug Selection in Infertility
Step 1 - Identify the Cause
| Diagnosis | First Drug |
|---|---|
| Anovulation / PCOS | Letrozole (now preferred over clomiphene) |
| Hyperprolactinemia | Cabergoline |
| Hypogonadotrophic hypogonadism | Pulsatile GnRH or Gonadotrophins |
| Unexplained / tubal / male factor (severe) | Straight to ART/IVF |
Step 2 - Ovulation Induction Ladder (PCOS)
Step 3 - ART Protocol Choice
- Long protocol (GnRH agonist): Better synchronisation, more eggs - used in poor/normal responders
- Antagonist protocol (GnRH antagonist): Shorter, lower OHSS risk - now preferred in many centres, especially high responders
Step 4 - Trigger & Luteal Support
- hCG trigger - standard, but raises OHSS risk
- GnRH agonist trigger - preferred in high OHSS risk (antagonist cycle only)
- Progesterone (vaginal) - mandatory luteal phase support after ART
Key Viva Point
"Letrozole has overtaken clomiphene as first-line ovulation induction in PCOS because it gives higher live birth rates with fewer multiple pregnancies" - based on the landmark Legro et al. NEJM 2014 RCT.