Can you change your settings and bring back the version where the answer and topics would be more detailed?
I don't have adjustable settings or different "versions" that can be toggled. My response style is consistent — I don't have a previous mode with more detailed answers that I can switch back to.
That said, I can absolutely give you more detailed, thorough responses. The easiest way to get that is to:
- Ask me to go deeper — just say "explain this in detail" or "give me a comprehensive answer"
- Be specific about what you want — e.g., "cover the pathophysiology, treatment, and complications"
- Tell me the audience — e.g., "explain this at a medical student level"
If you had a previous conversation where the answers felt more thorough, that was likely shaped by how the questions were phrased rather than a different setting. What topic would you like to explore in depth?
TB meningitis cause, treatment, radiology, complications and Patho physiology explain all this in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Searching PubMed
tuberculous meningitis
Reading File
Reading File
Loading Image
Reading File
I now have rich, comprehensive content from five major textbooks (Adams & Victor's Neurology, Harrison's Principles, Robbins Pathology, Murray & Nadel's Respiratory Medicine, and Grainger & Allison's Radiology) plus the latest 2026 Lancet Infectious Diseases guideline. Let me compile the full answer.
Tuberculous Meningitis (TBM) — Comprehensive Review
1. CAUSE & EPIDEMIOLOGY
Causative organism: TBM is caused primarily by Mycobacterium tuberculosis. Rare causes include M. bovis, M. avium, M. kansasii, and M. fortuitum (the latter mainly after neurosurgical procedures or cranial trauma). The emergence of HIV has dramatically increased cases from both typical and atypical mycobacteria.
— Adams and Victor's Principles of Neurology, 12th Ed.
Epidemiology:
- TBM accounts for ~5% of all extrapulmonary TB cases
- In the U.S., incidence declined steadily until ~1985, when a 16% annual increase occurred — driven largely by HIV (tuberculosis may be the first clinical manifestation of HIV; among patients with full-blown AIDS, the incidence is nearly 500 times that of the general population)
- In developing countries (especially sub-Saharan Africa), TB is ~25 times more frequent than in the U.S., again largely due to HIV prevalence
- In more than half of TBM cases, evidence of old pulmonary lesions or a miliary pattern is found on chest X-ray — Adams & Victor; Harrison's Principles of Internal Medicine, 22nd Ed.
Risk groups: Children under 20 (though in the U.S. adults now predominate), HIV-infected individuals, alcoholics, immigrants from high-prevalence regions (Asia, Africa, India), elderly, and immunocompromised patients.
2. PATHOPHYSIOLOGY
Step 1 — Primary Infection and Hematogenous Seeding
TBM does not arise directly from a primary pulmonary focus. The two-stage pathogenesis (Rich's hypothesis) involves:
- Hematogenous seeding of the meninges and subpial brain parenchyma → formation of subpial or subependymal tubercles (Rich foci)
- Rupture of one or more tubercles into the subarachnoid space → bacterial discharge triggers intense meningeal inflammation
Step 2 — Basal Meningeal Exudate
The brunt of the pathologic process falls on the basal meninges. A thick, gelatinous exudate accumulates, obliterating:
- Pontine and interpeduncular cisterns
- Third ventricular floor and subthalamic region
- Optic chiasm
- Undersurfaces of the temporal lobes
Microscopically, the exudate contains fibrin, lymphocytes, plasma cells, mononuclear cells, and some PMNs. The meningeal tubercles consist of central caseation surrounded by epithelioid cells, Langhans giant cells, lymphocytes, and connective tissue. The ependymia and choroid plexus are studded with minute tubercles.
Step 3 — Cascade of Injury
| Mechanism | Consequence |
|---|---|
| Obliterative endarteritis — marked intimal thickening of penetrating arteries within the subarachnoid space | Arterial occlusion → brain infarction (basal ganglia, internal capsule, brainstem) |
| CSF obstruction — exudate blocks basal cisterns and aqueduct | Communicating or obstructive hydrocephalus |
| Cranial nerve entrapment — nerves traverse the exudate-filled basal cisterns | Cranial nerve palsies (especially CN III, IV, VI for oculomotor; CN VII, VIII) |
| Arachnoid fibrosis — dense fibrous adhesive arachnoiditis in chronic disease | Progressive hydrocephalus, spinal cord compression, nerve root involvement |
| Vasogenic edema — surrounding tuberculomas | Mass effect, seizures |
| Paradoxical immune response (IRIS in HIV patients) | Tuberculoma enlargement during treatment |
Key distinction from bacterial meningitis: Unlike pyogenic meningitis, the disease process is not confined to the subarachnoid space — it penetrates the pia and ependymia and invades underlying brain, making it truly a meningoencephalitis.
— Adams & Victor; Robbins Pathologic Basis of Disease; Grainger & Allison's Diagnostic Radiology
3. CLINICAL FEATURES
Prodrome (1–2 weeks before diagnosis)
- Low-grade fever, malaise, anorexia, irritability
- Headache (>50% of cases)
- Lethargy, confusion
Established Disease
- Neck stiffness (75%), Kernig's sign, Brudzinski's sign
- Cranial nerve palsies — especially oculomotor (CN III, IV, VI) — present in ~20% at diagnosis
- Papilledema — from raised ICP
- Hypothermia and hyponatremia (SIADH)
- Seizures (especially in children)
- Focal deficits from arteritis and infarction
Key feature: Symptoms evolve over 1–2 weeks, much slower than pyogenic bacterial meningitis — this subacute/chronic onset is a hallmark diagnostic clue.
CSF Findings (Lumbar Puncture — cornerstone of diagnosis)
| Parameter | Typical Finding |
|---|---|
| Leukocytes | Up to 1000/μL; lymphocyte predominance (neutrophils may dominate early) |
| Protein | Markedly elevated: 1–8 g/L (100–800 mg/dL) |
| Glucose | Low (moderately reduced or rarely normal) |
| AFB smear | Low sensitivity; repeated LPs increase yield |
| Culture | Diagnostic in up to 80% — gold standard |
| Xpert MTB/RIF | Sensitivity ~80%; preferred initial test |
4. RADIOLOGY
CT Scan
CT (with contrast) is typically the first imaging obtained. Key findings:
- Basal cistern obliteration — isoattenuating or slightly hyperattenuating exudate fills the interpeduncular and sylvian cisterns; enhances with IV contrast
- Communicating hydrocephalus — dilatation of lateral, third, and fourth ventricles; seen in 50% of adults and 85% of children
- Most sensitive/specific CT criteria for TBM:
- Linear enhancement of the middle cerebral artery cisterns
- Obliteration of CSF spaces around normal vascular enhancement
- Y-shaped enhancement at the junction of the suprasellar and MCA cisterns
- Asymmetry of enhancement
- Infarcts — basal ganglia, internal capsule, brainstem (from perforator arteritis)
- Tuberculomas — small rounded lesions, iso- or hypoattenuating, with variable vasogenic edema; ring enhancement with central caseation ("target sign")
MRI (Superior to CT)
MRI shows greater sensitivity for all features of TBM:
- Post-contrast T1: Marked basal meningeal enhancement (see image below)
- FLAIR: High-signal abnormalities in basal ganglia from subacute infarction
- ADC maps/DWI: Restricted diffusion in subacute infarcts; tuberculomas may show restricted or elevated diffusion
- T2: Caseating tuberculomas show characteristically low signal (due to solid proteinaceous content); non-caseated lesions are T2-bright
- Differential for basal enhancement: fungal meningitis, neurosarcoidosis, carcinomatous meningitis
MRI of TBM — gadolinium-enhanced axial image showing intense basal meningeal enhancement with multiple abscesses and hydrocephalus:
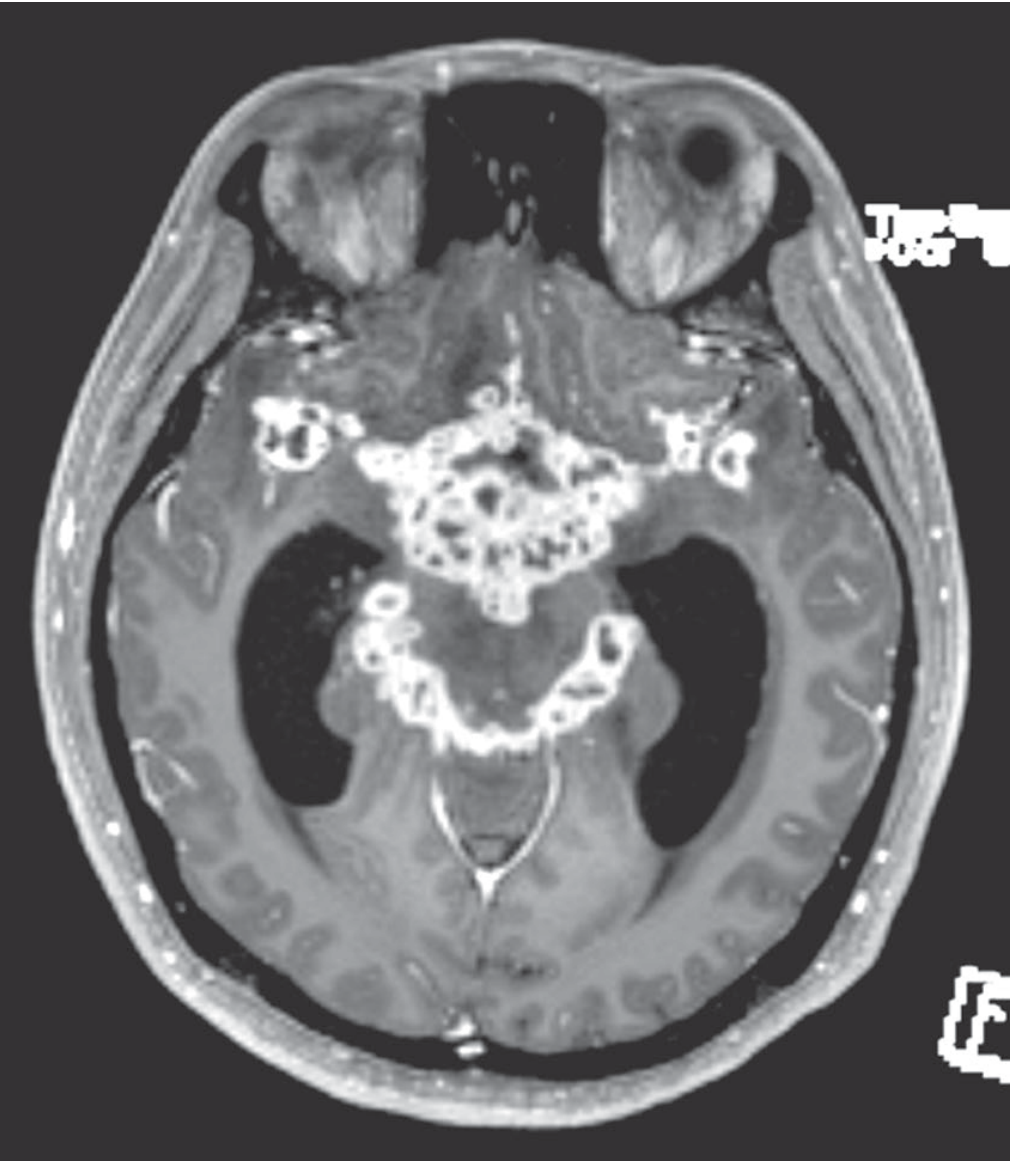
MRI — axial post-gadolinium T1: intense enhancement of the basal cisterns (interpeduncular and perimesencephalic) with hydrocephalus and cranial nerve involvement. — Adams & Victor's Principles of Neurology
The classic neuroradiologic triad of TBM:
- Basal meningeal enhancement
- Hydrocephalus
- Cerebral/brainstem infarction — ROSEN's Emergency Medicine; Grainger & Allison's Diagnostic Radiology
5. TREATMENT
Antituberculous Chemotherapy
Standard regimen (adults):
| Phase | Duration | Drugs |
|---|---|---|
| Intensive phase | 2 months | Isoniazid (INH) + Rifampicin (RIF) + Pyrazinamide (PZA) + Ethambutol (EMB) |
| Continuation phase | 7–10 months (total 9–12 months) | INH + RIF |
Total treatment duration for TBM is 9–12 months — significantly longer than pulmonary TB (6 months), due to poor CNS drug penetration and high mortality/morbidity.
Children (per AAP guidelines):
- Initial 2 months: INH + RIF + PZA + ethionamide or aminoglycoside (in place of EMB, which has poor CNS penetration)
- Continuation phase 7–10 months: INH + RIF
Drug penetration into CNS:
- INH and PZA have excellent CSF penetration
- RIF has moderate penetration (enhanced with inflammation)
- EMB has poor CSF penetration — reason for substitution in pediatric TBM
Adjunctive Corticosteroids (HIGH-QUALITY EVIDENCE — STRONGLY RECOMMENDED)
Corticosteroids are one of the few adjunctive therapies in infectious disease supported by high-quality RCT evidence. They reduce mortality and disability.
Dexamethasone schedule (adults >14 years):
- 0.4 mg/kg/day IV, tapering by 0.1 mg/kg/week for 4 weeks
- Then oral: 4 mg/day, tapering by 1 mg/week for 4 weeks
- Total: ~6–8 weeks
Children (<14 years):
- Prednisolone 4 mg/kg/day (or dexamethasone 0.6 mg/kg/day) for 4 weeks, then taper over 2–4 weeks
Note: In PLWH (HIV), a recent placebo-controlled study demonstrated no mortality benefit from adjunctive dexamethasone. This is an important exception to the general recommendation.
CSF Monitoring
Repeated lumbar punctures are recommended to monitor cell count, glucose, and protein — especially early in therapy. An overly robust inflammatory response in this closed-space infection can worsen outcomes.
Management of HIV Co-infection
Antiretroviral therapy (ART) should be started within 2 weeks of initiating antituberculous therapy in HIV-infected patients.
Surgical Management
Neurosurgical intervention is required in a subset of patients:
- Hydrocephalus — ventriculoperitoneal shunt or external ventricular drainage (required in up to 25% of advanced cases)
- Tuberculous cerebral abscess — drainage
- Paraparesis from spinal cord compression — Murray & Nadel's Respiratory Medicine; Harrison's; Adams & Victor's
6. COMPLICATIONS
Acute Complications
| Complication | Mechanism |
|---|---|
| Communicating hydrocephalus | Basal exudate obstructs CSF resorption at arachnoid granulations |
| Obstructive hydrocephalus | Exudate blocks aqueduct of Sylvius or 4th ventricle foramina |
| Cerebral infarction | Obliterative endarteritis of penetrating arteries → basal ganglia, internal capsule, brainstem infarcts |
| Cranial nerve palsies | CN VI (abducens) most common; also CN III, IV, VII, VIII entrapped in basal exudate |
| Raised intracranial pressure | Hydrocephalus + cerebral edema |
| Seizures | Cortical irritation, infarction, tuberculomas |
| SIADH/hyponatremia | Hypothalamic involvement |
Chronic/Long-term Complications
| Complication | Mechanism |
|---|---|
| Arachnoid fibrosis | Dense fibrous adhesive arachnoiditis at the base of brain → chronic progressive hydrocephalus, spinal cord compression, radiculopathy |
| Neurologic sequelae | Documented in 25% of treated patients, usually when diagnosis is delayed |
| Tuberculoma enlargement (paradoxical reaction/IRIS) | Immune reconstitution inflammatory syndrome during treatment — corticosteroids can reduce size and symptoms |
| Brain infarction (delayed) | Progressive arteritis with late ischemic events |
| Visual loss | Optic nerve involvement, raised ICP, optic atrophy |
| Intellectual disability / cognitive decline | Especially in children with delayed treatment |
| Death | Severe disability or death in ~50% of cases; mortality 18–40% even with treatment |
If left untreated, TBM is uniformly fatal. — Robbins Pathology; Murray & Nadel; Tintinalli's Emergency Medicine
Recent Evidence (2024–2026)
- Lancet Infect Dis 2026 — Clinical Practice Guideline for TBM (PMID 40840485): The most current guideline, published February 2026, providing updated evidence-based recommendations for TBM management.
- JAMA Network Open 2024 — Global Case Fatality of Bacterial Meningitis (PMID 39093565): Systematic review/meta-analysis over 80 years confirms the persistently high mortality of TBM compared to other bacterial meningitides.
- Biomedicine & Pharmacotherapy 2025 — Rifampicin Neuroprotection (PMID 40024057): Systematic review of rifampicin's neuroprotective properties, relevant to understanding its role beyond antimicrobial activity in TBM.
Summary
| Topic | Key Points |
|---|---|
| Cause | M. tuberculosis; hematogenous seeding of meninges |
| Pathophysiology | Tubercle formation → rupture → basal exudate → endarteritis + hydrocephalus + CN entrapment |
| Radiology | Classic triad: basal enhancement + hydrocephalus + infarction; MRI > CT |
| Treatment | 9–12 months HRZE/HR; adjunctive dexamethasone 6–8 weeks; neurosurgical shunting in 25% |
| Complications | Hydrocephalus, infarction, CN palsies, arachnoiditis, neurologic sequelae in 25% of survivors |
Sources: Adams and Victor's Principles of Neurology 12th Ed. | Harrison's Principles of Internal Medicine 22nd Ed. | Robbins Pathologic Basis of Disease | Murray & Nadel's Textbook of Respiratory Medicine | Grainger & Allison's Diagnostic Radiology | ROSEN's Emergency Medicine | Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.