Here are detailed answers for Questions 6-10, exam-ready with diagrams:
Question 6 - Classify Amino Acids on the Basis of Nutritional and Metabolic Significance. Add a Note on Biologically Important Peptides.
Definition
Amino acids are organic compounds containing an amino group (-NH₂) and a carboxyl group (-COOH) attached to the same alpha carbon (α-carbon), along with a distinctive side chain (R group). General formula: NH₂-CHR-COOH
Classification Diagram
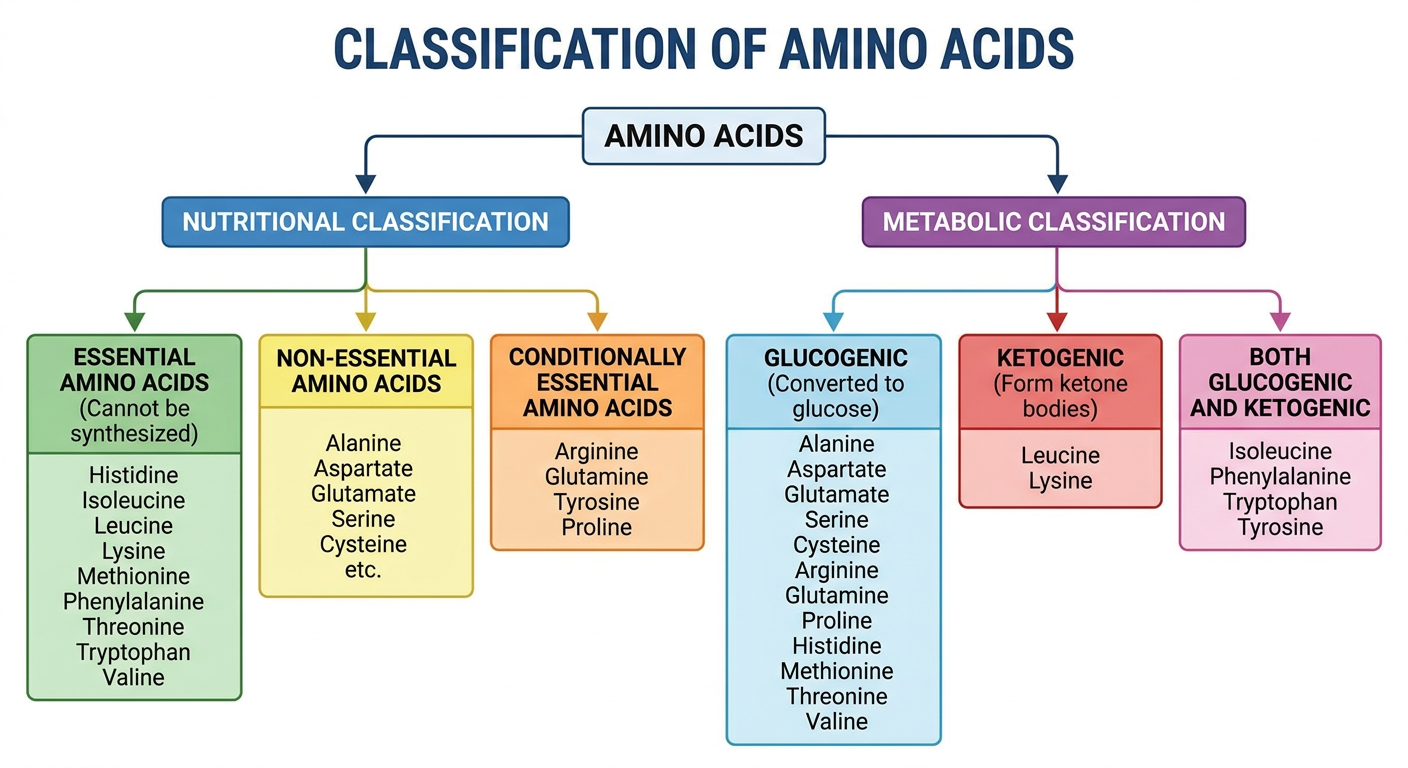
A. Classification Based on Nutritional Significance
1. Essential Amino Acids (Indispensable)
Cannot be synthesized by the body in adequate amounts - must be obtained from diet.
Mnemonic: PVT TIM HaLL (Private Tim Hall)
| Amino Acid | Notes |
|---|
| Phenylalanine | Precursor of tyrosine; deficiency causes PKU |
| Valine | Branched chain AA |
| Threonine | - |
| Tryptophan | Precursor of serotonin, niacin |
| Isoleucine | Branched chain AA |
| Methionine | Sulfur-containing; precursor of SAM |
| Histidine | Essential in infants/adults |
| Leucine | Branched chain AA; purely ketogenic |
| Lysine | Important for collagen cross-linking |
2. Non-Essential Amino Acids (Dispensable)
Can be synthesized by the body from metabolic intermediates.
Examples: Alanine, Aspartate, Glutamate, Asparagine, Glutamine, Serine, Glycine, Proline, Aspartic acid
3. Conditionally Essential Amino Acids
Non-essential under normal conditions but become essential during illness, growth, or stress:
- Arginine (essential in growing children and during urea cycle defects)
- Tyrosine (essential when phenylalanine is absent)
- Cysteine (essential when methionine is deficient)
- Glutamine (essential in critical illness)
B. Classification Based on Metabolic Significance
1. Glucogenic Amino Acids
Degraded to pyruvate, oxaloacetate, alpha-ketoglutarate, succinyl-CoA, or fumarate - can be converted to glucose.
- Examples: Alanine, Glycine, Serine, Threonine, Valine, Methionine, Histidine, Glutamate, Aspartate, Arginine, Proline
2. Ketogenic Amino Acids
Degraded to acetyl-CoA or acetoacetyl-CoA - form ketone bodies, cannot produce glucose.
- Purely ketogenic: Leucine, Lysine (important exam point!)
3. Both Glucogenic and Ketogenic
Degraded to both glucose and ketone body precursors:
- Isoleucine, Phenylalanine, Tryptophan, Tyrosine (remember: IP-TT)
C. Other Classifications
Based on Side Chain Chemistry:
- Non-polar/Hydrophobic: Glycine, Alanine, Valine, Leucine, Isoleucine, Proline, Methionine, Phenylalanine, Tryptophan
- Polar Uncharged: Serine, Threonine, Cysteine, Tyrosine, Asparagine, Glutamine
- Positively charged (basic): Lysine, Arginine, Histidine
- Negatively charged (acidic): Aspartate, Glutamate
Note on Biologically Important Peptides
Peptides are short chains of amino acids linked by peptide bonds. Several are of great biological and clinical significance:
| Peptide | Composition | Functions |
|---|
| Glutathione (GSH) | Glu-Cys-Gly (tripeptide) | Antioxidant, protects against free radicals; detoxification |
| Vasopressin (ADH) | 9 amino acids | Water reabsorption in kidneys; antidiuretic action |
| Oxytocin | 9 amino acids | Uterine contraction; milk ejection (childbirth & lactation) |
| Insulin | 51 amino acids (A+B chains) | Glucose uptake; hypoglycemic hormone |
| Glucagon | 29 amino acids | Raises blood glucose; glycogenolysis |
| ACTH | 39 amino acids | Stimulates adrenal cortex |
| Angiotensin II | 8 amino acids | Vasoconstriction; stimulates aldosterone |
| Bradykinin | 9 amino acids | Vasodilation; pain mediator; allergic reactions |
| Enkephalins | 5 amino acids | Endogenous opioids; pain suppression |
| Thyrotropin-releasing hormone (TRH) | 3 amino acids (tripeptide) | Stimulates TSH release |
| Carnosine | Ala-His (dipeptide) | Muscle buffer; antioxidant in muscle |
Question 7 - Define Proteins. Write in Detail Structural Organization of Proteins. Add a Note on Disorders Associated with Misfolded Proteins.
Definition
Proteins are high molecular weight biological macromolecules composed of amino acids linked together by peptide bonds (-CO-NH-). They are the most abundant and functionally diverse biological molecules, making up ~50% of dry cell mass.
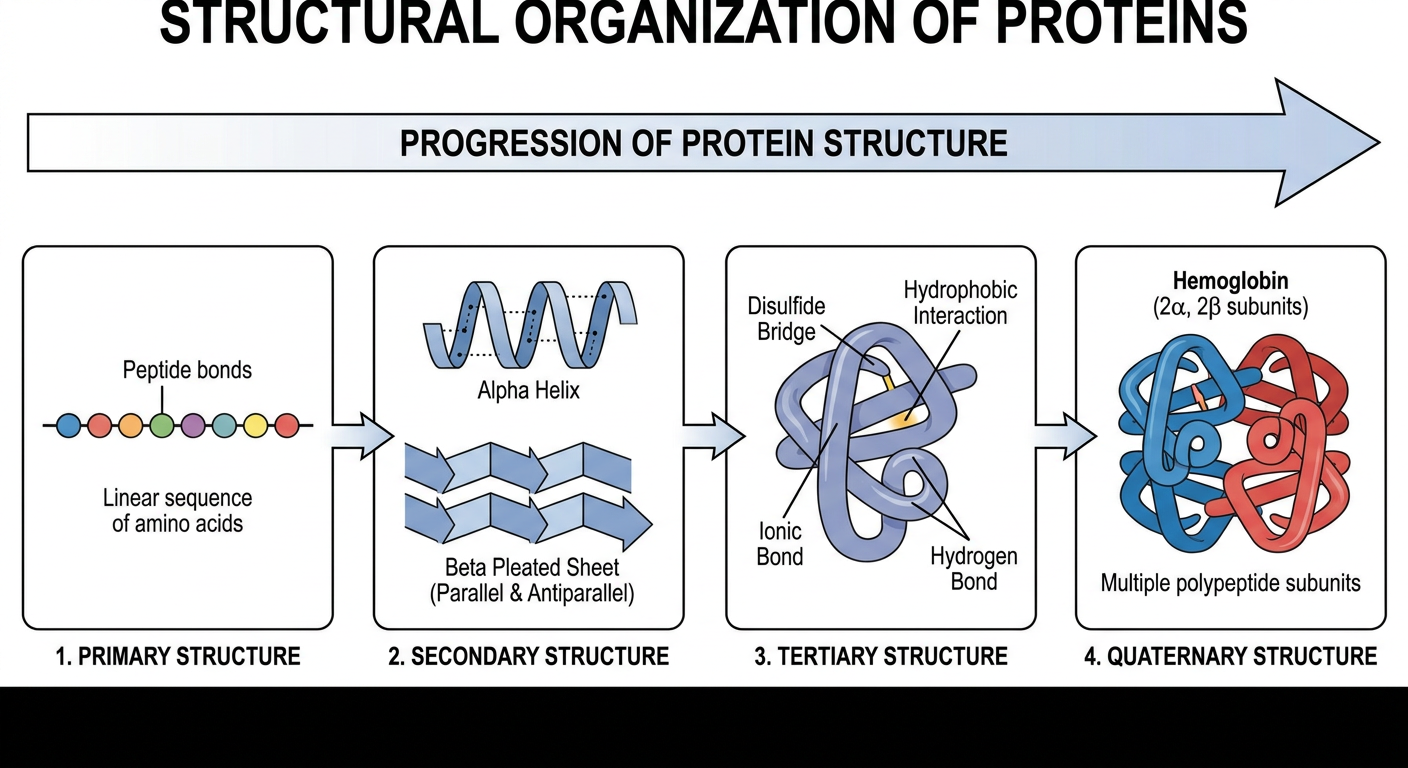
Levels of Protein Structure
1. Primary Structure (1°)
- The linear sequence of amino acids in a polypeptide chain
- Amino acids are linked by peptide bonds (covalent bonds between -COOH of one AA and -NH₂ of next)
- Sequence is read from N-terminus (amino end) to C-terminus (carboxyl end)
- Determined by the gene (DNA sequence)
- Importance: A single change in primary structure can cause disease (e.g., sickle cell anemia - Val replaces Glu at position 6 of beta-globin)
2. Secondary Structure (2°)
- Local folding of the polypeptide backbone due to hydrogen bonds between NH and C=O groups
- Two main types:
a. Alpha (α) Helix:
- Right-handed spiral; 3.6 amino acids per turn
- Hydrogen bonds between residues 4 positions apart (i to i+4)
- Stabilized by H-bonds parallel to helix axis
- Example: Myoglobin, Collagen (triple helix)
b. Beta (β) Pleated Sheet:
- Adjacent strands aligned laterally with H-bonds between them
- Can be parallel (strands run same direction) or antiparallel (strands run opposite)
- More rigid than alpha helix
- Example: Silk fibroin, immunoglobulins
c. Beta Turns: Reverse turns allowing the chain to fold back on itself; connect beta sheets.
d. Random Coil: No regular repeating pattern.
3. Tertiary Structure (3°)
- Overall 3-dimensional folding of the entire polypeptide chain
- Maintained by multiple non-covalent interactions:
- Hydrophobic interactions (most important - non-polar side chains cluster inside)
- Hydrogen bonds
- Ionic bonds (salt bridges) between oppositely charged R groups
- Van der Waals forces
- One covalent bond: Disulfide bonds (-S-S-) between cysteine residues
- Results in a specific functional 3D shape (native conformation)
- Example: Myoglobin (single chain, 153 AA), enzymes
4. Quaternary Structure (4°)
- Association of two or more polypeptide subunits to form a functional protein
- Same types of bonds as tertiary structure (no covalent bonds between subunits except in some cases)
- Subunits may be identical (homomeric) or different (heteromeric)
- Example:
- Hemoglobin: 2α + 2β chains (heterotetramer)
- Collagen: triple helix of 3 alpha chains
- DNA polymerase: multiple subunits
Flowchart: Forces Stabilizing Protein Structure
Primary → Peptide bonds (covalent)
Secondary → Hydrogen bonds (between backbone NH and C=O)
Tertiary → Hydrophobic interactions + H-bonds + Ionic bonds + Disulfide bonds
Quaternary → Non-covalent interactions between subunits
Note on Disorders Associated with Misfolded Proteins (Conformational Diseases / Proteopathies)
When proteins misfold, they lose normal function and may aggregate into toxic forms. These are called protein folding disorders or proteopathies.
Mechanism of Misfolding:
Normal protein → Stress/Mutation/Aging → Misfolding → Aggregation → Amyloid fibrils or toxic oligomers → Cell death / organ dysfunction
| Disease | Misfolded Protein | Clinical Features |
|---|
| Alzheimer's Disease | Amyloid-beta (Aβ) plaques + Tau tangles | Progressive dementia, memory loss |
| Parkinson's Disease | Alpha-synuclein (Lewy bodies) | Tremor, rigidity, bradykinesia |
| Huntington's Disease | Mutant huntingtin (polyglutamine expansion) | Chorea, cognitive decline |
| Prion Disease (Creutzfeldt-Jakob) | PrPSc (misfolded prion protein) | Rapidly progressive dementia, fatal; transmissible |
| Sickle Cell Anemia | HbS (Val6Glu substitution in beta-globin) | Sickling of RBCs, hemolytic anemia, vaso-occlusion |
| Cystic Fibrosis | CFTR protein misfolding (ΔF508 mutation) | Thick mucus, recurrent lung infections |
| Alpha-1-Antitrypsin Deficiency | Polymerization of AAT in liver | Liver cirrhosis + emphysema |
| Amyloidosis | Amyloid fibrils (various proteins - AL, AA, ATTR) | Multi-organ deposits; Congo red staining (apple-green birefringence) |
| Type 2 Diabetes | IAPP (Islet Amyloid Polypeptide) aggregation | Destruction of pancreatic beta cells |
Role of Chaperones (HSPs):
- Heat shock proteins (HSP70, HSP90, HSP60) are molecular chaperones that help correct protein folding
- Mutated/overwhelmed chaperones → misfolding accumulates
- Unfolded Protein Response (UPR) in ER is triggered; if overwhelmed → apoptosis
Question 8 - Describe the Functions of Plasma Proteins. Add a Note on Clinical Significance of Acute Phase Proteins.
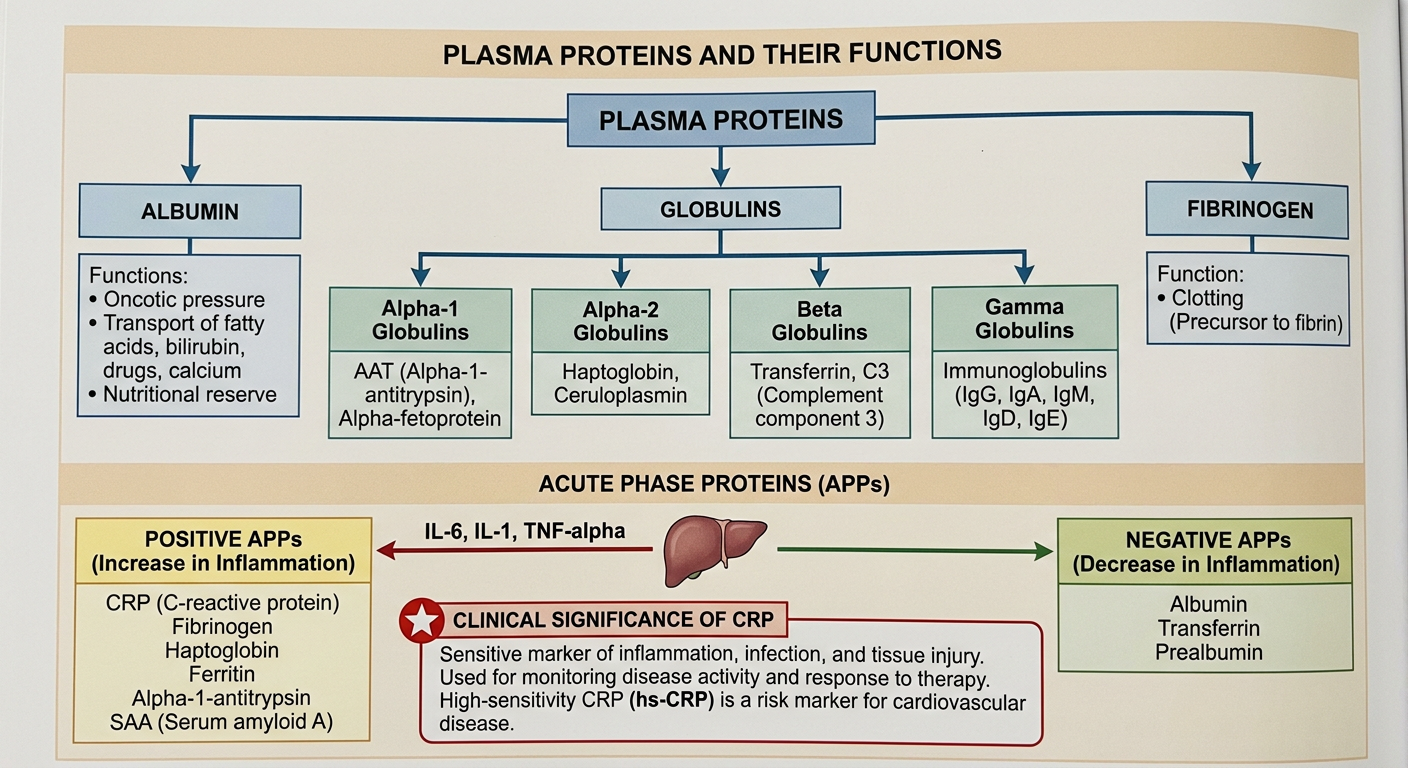
Plasma Proteins: Overview
Plasma proteins are a complex mixture of proteins found in blood plasma. Normal total plasma protein = 6.5-8.5 g/dL. Synthesized mainly by the liver (except immunoglobulins - synthesized by plasma cells).
Plasma Proteins Diagram
Separation by Serum Protein Electrophoresis (SPE)
On electrophoresis (pH 8.6), proteins separate into 5 bands:
Albumin > Alpha-1 globulin > Alpha-2 globulin > Beta globulin > Gamma globulin
| Fraction | Normal % | Key Proteins |
|---|
| Albumin | 50-60% | Albumin |
| Alpha-1 | 3-5% | Alpha-1-antitrypsin (AAT), AAG (orosomucoid), alpha-fetoprotein |
| Alpha-2 | 8-12% | Haptoglobin, ceruloplasmin, alpha-2-macroglobulin |
| Beta | 10-15% | Transferrin, C3, C4, beta-lipoprotein (LDL), fibrinogen |
| Gamma | 15-22% | Immunoglobulins (IgG, IgA, IgM, IgD, IgE) |
Functions of Major Plasma Proteins
1. Albumin (Most abundant - 3.5-5.0 g/dL)
- Osmotic pressure (oncotic pressure) - maintains plasma volume, prevents edema
- Transport: Fatty acids, bilirubin, bile salts, drugs (penicillin, aspirin, warfarin), Ca²⁺, hormones (T3, T4), metals
- Buffer function: Acts as plasma buffer
- Nutritional reservoir: Source of amino acids
- Clinical: Hypoalbuminemia → edema, ascites (seen in nephrotic syndrome, liver cirrhosis, malnutrition)
2. Globulins - Alpha Fraction
- Alpha-1-antitrypsin (AAT): Inhibits neutrophil elastase; protects lung tissue; deficiency → emphysema
- Haptoglobin (alpha-2): Binds free hemoglobin; prevents renal loss of iron; decreased in hemolysis
- Ceruloplasmin (alpha-2): Copper transport; ferroxidase activity; decreased in Wilson's disease
- Alpha-2-macroglobulin: Broad-spectrum protease inhibitor
3. Globulins - Beta Fraction
- Transferrin: Iron transport (Fe³⁺ form); decreased in iron deficiency anemia
- Complement proteins (C3, C4): Part of immune defense
- Beta-lipoprotein: Lipid transport
4. Globulins - Gamma Fraction
- Immunoglobulins (IgG, IgA, IgM, IgD, IgE): Antibodies; immune defense
- Polyclonal increase in chronic infections; monoclonal spike in myeloma
5. Fibrinogen
- Clotting factor; converted to fibrin by thrombin during coagulation
- Normal: 200-400 mg/dL; absent in serum (present in plasma)
6. Other Transport Proteins
- Thyroxine-binding globulin (TBG): Transports T3 and T4
- Corticosteroid-binding globulin (CBG/Transcortin): Carries cortisol
Note on Acute Phase Proteins (APPs) and Their Clinical Significance
Definition
Acute phase proteins are plasma proteins whose concentration changes by at least 25% during inflammatory states. They are part of the acute phase response, triggered by infection, trauma, surgery, or inflammation.
Trigger
Cytokines (IL-6, IL-1, TNF-alpha) released from macrophages and monocytes stimulate the liver to alter production of APPs.
Types:
Positive APPs (increase during inflammation):
| Protein | Normal | Rise | Clinical Use |
|---|
| C-reactive protein (CRP) | <1 mg/L | 1000-fold! | Best marker of inflammation/infection; monitoring treatment |
| Serum Amyloid A (SAA) | Low | 1000-fold | Precursor of AA amyloid |
| Fibrinogen | 200-400 mg/dL | 2-3 fold | Basis of elevated ESR |
| Haptoglobin | 30-200 mg/dL | 2-3 fold | Hemolysis marker |
| Alpha-1-antitrypsin | 90-200 mg/dL | 2-4 fold | Protease inhibitor |
| Ferritin | 20-250 ng/mL | 3-4 fold | Iron storage; elevated in inflammation |
| Complement proteins (C3, C4) | Normal | Increase | Immune activation |
Negative APPs (decrease during inflammation):
| Protein | Clinical Significance |
|---|
| Albumin | "Negative" marker; malnutrition, chronic inflammation |
| Transferrin | Decreases; iron redistribution |
| Prealbumin (Transthyretin) | Short half-life (2 days); sensitive marker of nutritional status |
| Retinol-binding protein | - |
Clinical Significance of CRP:
- Diagnostic: Distinguishes bacterial (high CRP) from viral infection (low CRP)
- Monitoring: Treatment response in rheumatoid arthritis, IBD, sepsis
- Cardiac risk: High-sensitivity CRP (hsCRP) >3 mg/L = increased cardiovascular risk
- Neonatal sepsis: CRP is early reliable marker
- Not useful for: Distinguishing disease types (non-specific)
Question 9 - Describe the Structure of Immunoglobulin. Classify Immunoglobulins Along with Their Functions. Explain Paraproteinemias in Brief.
Immunoglobulin Structure Diagram
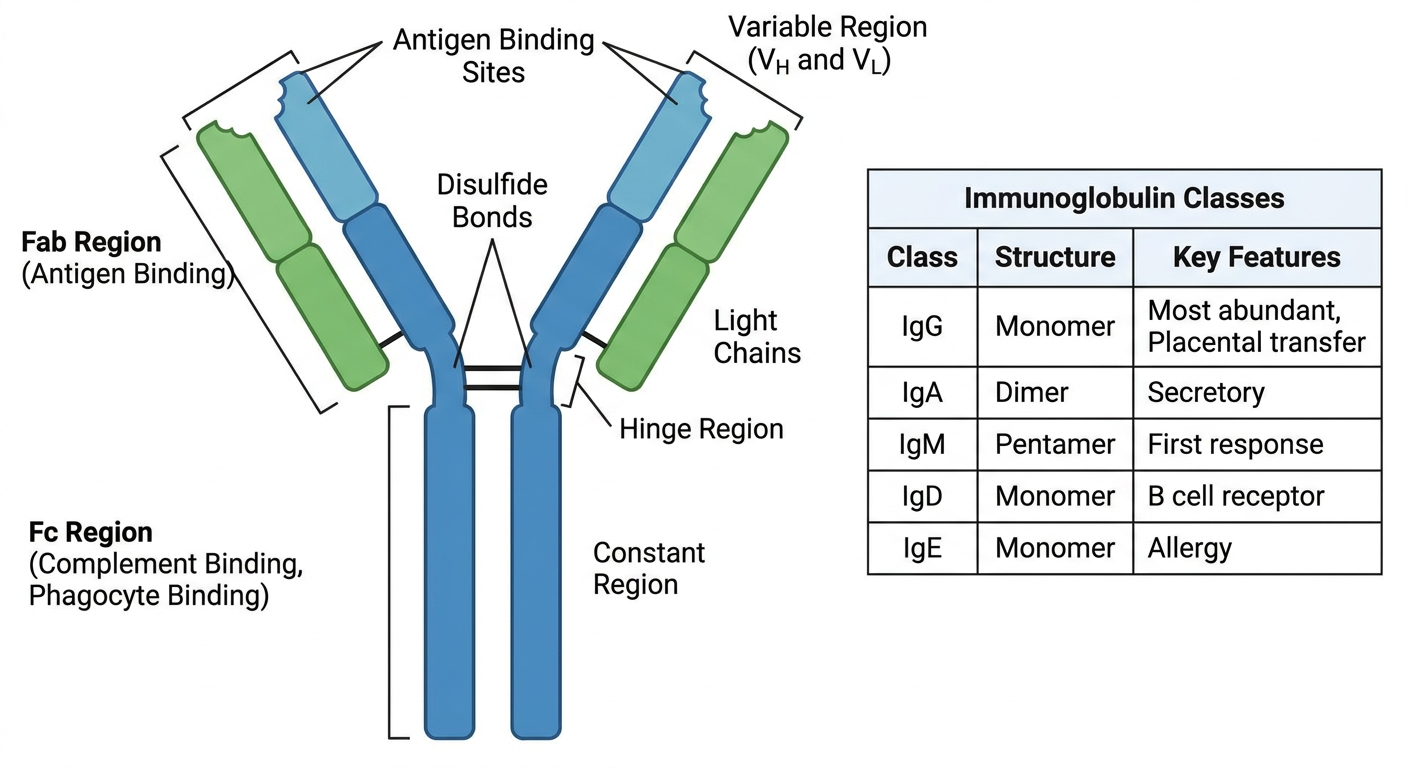
Structure of Immunoglobulin (IgG as prototype)
Immunoglobulins are glycoproteins produced by plasma cells (differentiated B lymphocytes). Basic unit = monomer composed of 4 polypeptide chains.
Basic 4-Chain Structure:
1. Two Heavy (H) chains: ~50,000 Da each, larger chains
2. Two Light (L) chains: ~25,000 Da each - either Kappa (κ) or Lambda (λ) type (one type per antibody)
All chains are held together by disulfide bonds (-S-S-) and non-covalent forces.
Regions:
| Region | Location | Function |
|---|
| Variable Region (V) | N-terminal of both H and L chains | Antigen binding; highly variable = determines antibody specificity |
| Constant Region (C) | C-terminal of H and L chains | Determines Fc functions (complement activation, Fc receptor binding) |
| Hypervariable Regions (CDRs) | Within V region | Direct contact with antigen; 3 CDRs per chain = 6 total |
| Fab Fragment | 2 arms of Y | Antigen binding fragment (contains VH+VL+CH1+CL) |
| Fc Fragment | Stem of Y | Crystallizable fragment; mediates effector functions |
| Hinge Region | Between Fab and Fc | Flexibility; site of papain and pepsin cleavage; rich in proline and cysteine |
Enzyme Cleavage:
- Papain cleaves above hinge → 2 Fab + 1 Fc fragments
- Pepsin cleaves below hinge → 1 F(ab')₂ + pFc' (destroyed)
Classification of Immunoglobulins
| Class | Structure | Serum Level | Half-life | Key Functions |
|---|
| IgG | Monomer (4 subclasses: IgG1-4) | 8-16 mg/mL (most abundant ~75%) | 23 days | Crosses placenta (maternal-fetal immunity); secondary immune response; opsonization; neutralization; complement activation |
| IgA | Monomer in serum; Dimer in secretions (with secretory component) | 1.4-4 mg/mL (~15%) | 6 days | Secretory immunity (saliva, tears, breast milk, gut); first line defense at mucosal surfaces |
| IgM | Pentamer (10 antigen-binding sites) | 0.5-2 mg/mL (~10%) | 5 days | First antibody in primary response; most efficient complement activator; ABO blood group antibodies; cold agglutinins |
| IgD | Monomer | Very low trace | 3 days | B cell antigen receptor (BCR); involved in B cell activation and differentiation |
| IgE | Monomer | Trace (<0.0003 mg/mL) | 2-3 days | Allergy and anaphylaxis (binds mast cells and basophils via FcεR1); antiparasitic immunity; reaginic antibody |
Paraproteinemias (Monoclonal Gammopathies)
Definition
Paraproteinemias refer to conditions characterized by the presence of an abnormal monoclonal immunoglobulin (M-protein or paraprotein) in the blood and/or urine, produced by a single clone of plasma cells or B lymphocytes.
Types and Features:
| Condition | M-protein | Key Features |
|---|
| Multiple Myeloma | Usually IgG or IgA (whole Ig); Bence Jones proteins (free light chains) in urine | CRAB criteria: hyperCalcemia, Renal failure, Anemia, Bone lesions; lytic skull lesions on X-ray; "rouleaux formation" on blood smear |
| Waldenström's Macroglobulinemia | IgM (pentamer - large!) | Hyperviscosity syndrome (visual disturbances, headache, bleeding); lymphoplasmacytic lymphoma |
| Monoclonal Gammopathy of Undetermined Significance (MGUS) | Any class, small amount (<3g/dL) | Asymptomatic; no organ damage; may progress to myeloma (~1%/year) |
| Primary Amyloidosis (AL amyloidosis) | Free light chains (lambda > kappa) | Organ deposition as amyloid fibrils; Congo red staining; affects kidney, heart, liver |
| Heavy Chain Disease | Free heavy chains (gamma, alpha, mu) | Rare; Fc fragments in serum/urine |
Detection:
- Serum Protein Electrophoresis (SPEP): Narrow "M-spike" in beta or gamma region
- Immunofixation Electrophoresis: Confirms class of M-protein
- Urine Protein Electrophoresis (UPEP): Detects Bence Jones proteins
- Serum Free Light Chain Assay: Kappa/Lambda ratio abnormal
Question 10 - Define Lipids. Classify with Suitable Examples. Add a Note on Functions and Clinical Significance of Phospholipids.
Definition of Lipids
Lipids are heterogeneous group of naturally occurring organic molecules that are insoluble in water (hydrophobic) but soluble in non-polar organic solvents (chloroform, ether, benzene, acetone). They contain carbon, hydrogen, and oxygen, with a lower proportion of oxygen compared to carbohydrates.
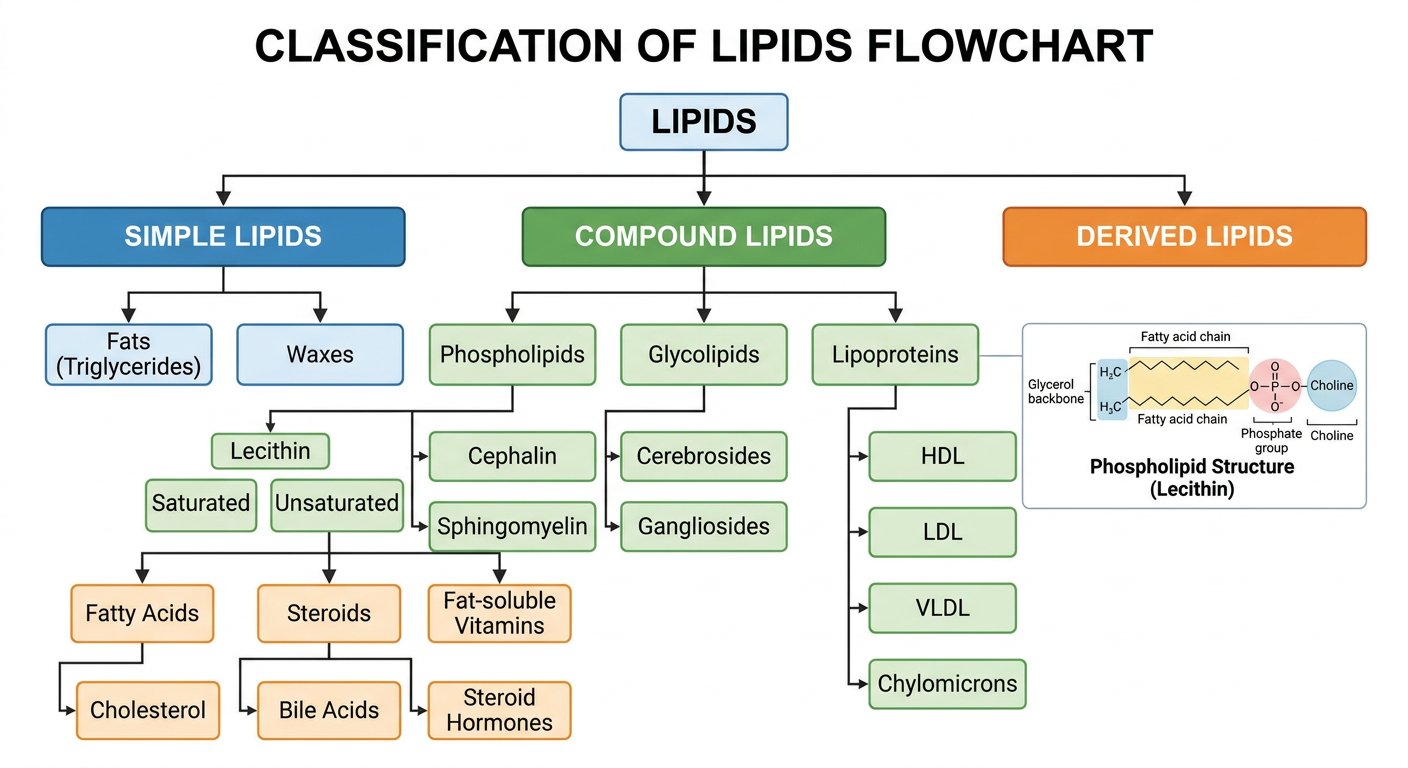
Classification Diagram
Detailed Classification
A. Simple Lipids (Esters of fatty acids with alcohol - yield only fatty acids on hydrolysis)
1. Triacylglycerols (Triglycerides / Fats & Oils):
- Glycerol + 3 Fatty acids
- Major storage form of energy in adipose tissue
- Oils = liquid at room temperature (unsaturated FA); Fats = solid (saturated FA)
- Examples: Olive oil (oleic acid), Lard (palmitic acid)
2. Waxes:
- Fatty acid + Long-chain alcohol
- Protective coating of skin, fur, leaves
- Examples: Beeswax (myricyl palmitate), Lanolin (wool wax), Cerumen (ear wax)
B. Compound Lipids (Complex lipids - contain additional non-lipid components)
1. Phospholipids:
- Glycerophospholipids (glycerol backbone):
- Lecithin (Phosphatidylcholine): Most abundant; lung surfactant
- Cephalin (Phosphatidylethanolamine): Brain; thromboplastin activity
- Phosphatidylserine: Brain; apoptosis signal
- Phosphatidylinositol: Signal transduction (PIP2 → IP3 + DAG)
- Cardiolipin (Diphosphatidylglycerol): Inner mitochondrial membrane; Wassermann antigen in syphilis
- Plasmalogen (Ether phospholipids): Heart muscle
- Sphingophospholipids:
- Sphingomyelin: Myelin sheath; contains sphingosine instead of glycerol
2. Glycolipids (Glycosphingolipids):
- Ceramide + sugar moieties (no phosphate)
- Cerebrosides: Ceramide + one sugar (glucose or galactose); myelin sheath
- Gangliosides: Ceramide + oligosaccharide + sialic acid (NANA); brain synapses; Tay-Sachs disease (accumulation of GM2)
- Sulfatides: Galactocerebroside + sulfate; Metachromatic leukodystrophy
3. Lipoproteins: (covered below - transport forms)
C. Derived Lipids (Products of hydrolysis of simple/compound lipids, still classified as lipids)
1. Fatty Acids:
- Saturated FA (SFA): No double bonds; solid; palmitic (16:0), stearic (18:0)
- Monounsaturated FA (MUFA): One double bond; oleic acid (18:1, Δ9)
- Polyunsaturated FA (PUFA): Multiple double bonds; linoleic (18:2, Δ9,12 - omega-6), linolenic (18:3 - omega-3), arachidonic acid (20:4 - omega-6)
- Essential FA: Linoleic (omega-6), Alpha-linolenic (omega-3) - cannot be synthesized
2. Steroids:
- Cholesterol: Precursor of all steroids; membrane component; 7-dehydrocholesterol (Vit D precursor)
- Bile acids: Cholic, chenodeoxycholic, deoxycholic acid; emulsification of fats
- Steroid hormones: Cortisol, aldosterone, testosterone, estrogen, progesterone
- Vitamin D: Calcitriol (active form)
3. Fat-Soluble Vitamins: Vitamins A, D, E, K
4. Eicosanoids (from arachidonic acid):
- Prostaglandins, Thromboxanes, Leukotrienes, Lipoxins
- Powerful local mediators; role in inflammation, fever, clotting
Note on Functions and Clinical Significance of Phospholipids
Structure of a Phospholipid:
Polar head (hydrophilic) + Glycerol + 2 Fatty acid tails (hydrophobic)
- sn-1 position: Saturated fatty acid
- sn-2 position: Unsaturated fatty acid (more fluid)
- sn-3 position: Phosphate + specific head group (choline/ethanolamine/serine/inositol)
This amphipathic nature enables them to form bilayers - the structural basis of all biological membranes.
Functions of Phospholipids:
1. Structural (Primary function):
- Form the lipid bilayer of all cellular membranes (plasma membrane, nuclear membrane, ER, mitochondria)
- Provide a fluid mosaic matrix for membrane proteins
- Control membrane fluidity (unsaturated FA increases fluidity)
2. Pulmonary Surfactant:
- Lecithin (dipalmitoyl phosphatidylcholine - DPPC) is the main component of lung surfactant
- Reduces alveolar surface tension; prevents lung collapse
- Clinical: Lecithin:Sphingomyelin (L:S) ratio in amniotic fluid assesses fetal lung maturity
- L:S ratio >2.0 = fetal lungs mature (safe delivery)
- L:S ratio <1.5 = Neonatal Respiratory Distress Syndrome (NRDS/HMD) risk
- Deficiency in premature neonates → Hyaline Membrane Disease (HMD)
3. Signal Transduction:
- Phosphatidylinositol 4,5-bisphosphate (PIP₂) is cleaved by phospholipase C → IP₃ + DAG
- IP₃ → Ca²⁺ release from ER
- DAG → activates Protein Kinase C (PKC)
- Central to many hormone and growth factor signaling pathways
4. Platelet Activating Factor (PAF):
- A modified phospholipid; potent mediator of inflammation, allergy, anaphylaxis
- Activates platelets, neutrophils, and macrophages
5. Eicosanoid Precursor:
- Membrane phospholipids are reservoir for arachidonic acid (at sn-2 position)
- Released by phospholipase A₂ → arachidonic acid → prostaglandins, thromboxanes, leukotrienes
- NSAIDs (aspirin, ibuprofen) inhibit COX enzymes in this pathway
- Corticosteroids inhibit phospholipase A₂ (via lipocortin) - broader anti-inflammatory action
6. Lipoprotein Structure:
- Form the surface monolayer of all lipoprotein particles (chylomicrons, VLDL, IDL, LDL, HDL)
- Allow transport of hydrophobic lipids in aqueous blood
7. Blood Coagulation:
- Cephalin (phosphatidylserine + phosphatidylethanolamine) provides the phospholipid surface for clotting factor assembly
- Normally on inner leaflet; flips to outer leaflet during platelet activation
- Cardiolipin is the antigen in the VDRL test for syphilis
8. Apoptosis Signaling:
- Phosphatidylserine (PS) normally on inner membrane leaflet
- Externalization of PS = "eat me" signal for macrophages to phagocytose apoptotic cells
Clinical Significance Summary:
| Condition | Phospholipid Involved | Mechanism |
|---|
| NRDS/HMD (premature infant) | Deficient lecithin/surfactant | Alveolar collapse, respiratory failure |
| Niemann-Pick Disease | Sphingomyelin accumulation | Sphingomyelinase deficiency; hepatosplenomegaly, neurodegeneration |
| Gaucher's Disease | Glucocerebroside accumulation | Glucocerebrosidase deficiency; "crinkled paper" macrophages |
| Antiphospholipid Syndrome | Antibodies to phosphatidylserine/cardiolipin | Thrombosis, recurrent miscarriages, false-positive VDRL |
| Acute Pancreatitis | Phospholipase A₂ activation | Destruction of pancreatic acinar cell membranes |
| Syphilis (VDRL test) | Cardiolipin as reagin antigen | Basis of Wassermann test |
Sources: Biochemistry textbook content. Key references: Harper's Illustrated Biochemistry, Lippincott's Biochemistry (Lieberman), Basic Medical Biochemistry (Marks), Lehninger Principles of Biochemistry.