Parapharyngeal space in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
parapharyngeal space tumor surgery
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
PARAPHARYNGEAL SPACE - 20 MARKS ANSWER
(RGUHS Postgraduate ENT Examination Standard)
1. INTRODUCTION / DEFINITION
The Parapharyngeal Space (PPS) is a potential space in the deep neck, filled with fat and areolar tissue. It is also called the lateral pharyngeal space, pharyngomaxillary space, pterygomaxillary space or pterygopharyngeal space - but the term "parapharyngeal space" is universally preferred (Scott-Brown's Otorhinolaryngology, 8th Ed.).
It functions as the central anatomic hub of the suprahyoid neck. Because it is surrounded by almost all other deep neck spaces, it serves as a marker/pivotal space - displacement patterns of the PPS fat help localize the origin of deep neck masses (Cummings Otolaryngology).
2. ANATOMY
Shape and Extent
The PPS is classically described as an inverted pyramid (Olsen 1994; Scott-Brown's):
| Feature | Detail |
|---|---|
| Shape | Inverted pyramid / cone |
| Base | Superiorly - sphenoid + temporal bones (includes jugular canal, hypoglossal canal, foramen lacerum) |
| Apex | Inferiorly - greater cornu of the hyoid bone |
| Vertical extent | Skull base to level of hyoid bone |
| Axial cross-section | Triangular (bilateral symmetry) |
| Coronal cross-section | Hourglass shape (thicker at skull base and hyoid, thinner in middle) |
DIAGRAM 1: Inverted Pyramid of the PPS
(Scott-Brown's Otorhinolaryngology, Figure 11.1)
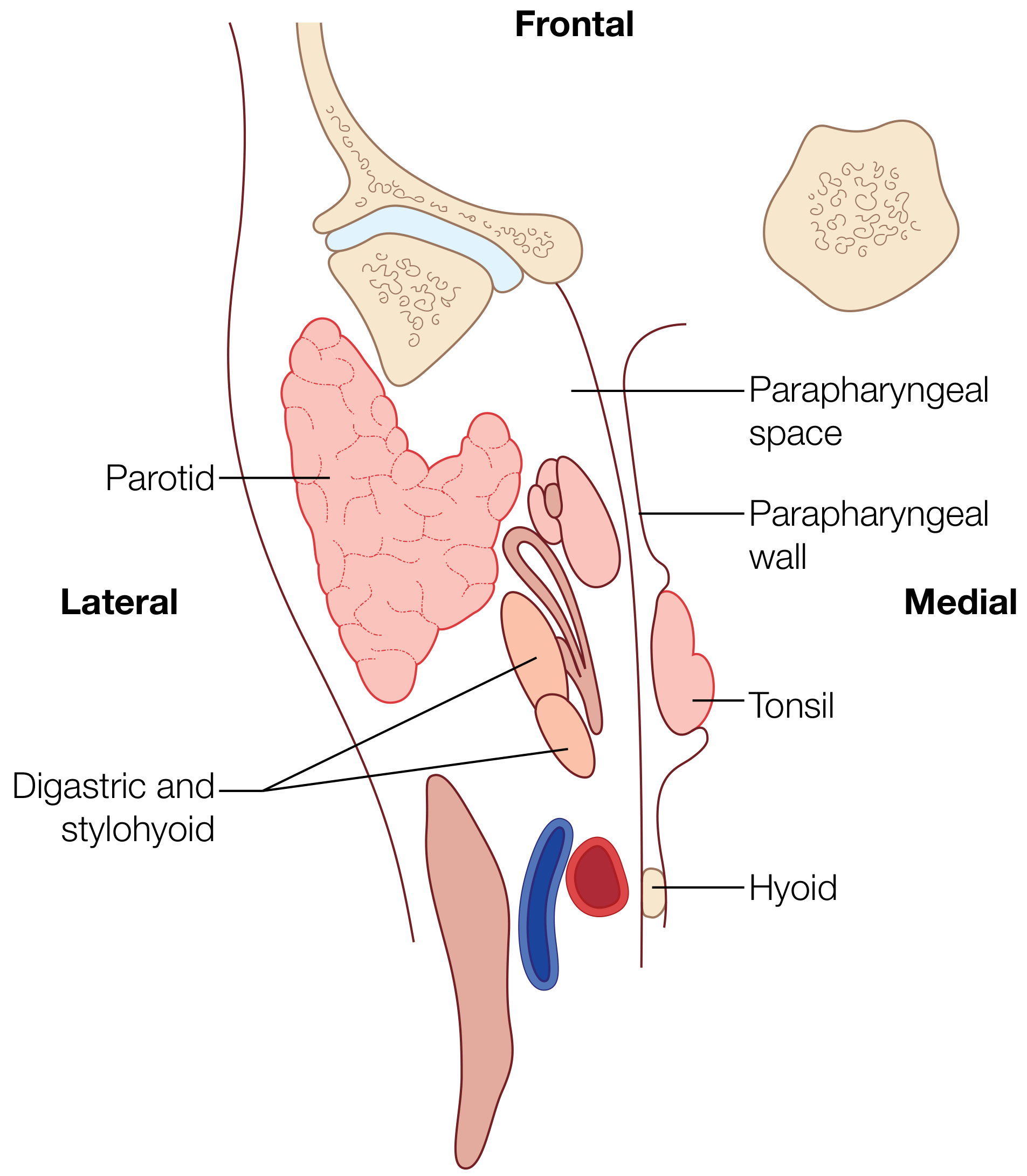
Boundaries
| Wall | Boundary |
|---|---|
| Medial | Superior pharyngeal constrictor + buccopharyngeal fascia (distensible) |
| Lateral | Medial pterygoid muscle, ramus of mandible, deep lobe of parotid gland; below mandible - fascia of posterior belly of digastric (relatively immobile) |
| Posterior | Prevertebral fascia; posterolateral - carotid sheath; posteromedial - retropharyngeal space |
| Anterior | Pterygomandibular raphe |
| Superior | Skull base (sphenoid + temporal bones) |
| Inferior | Hyoid bone (apex) |
DIAGRAM 2: Axial Cross-Section of the PPS - Pre-styloid and Post-styloid Compartments
(Scott-Brown's Otorhinolaryngology, Vol 2 - Figure 98.6)
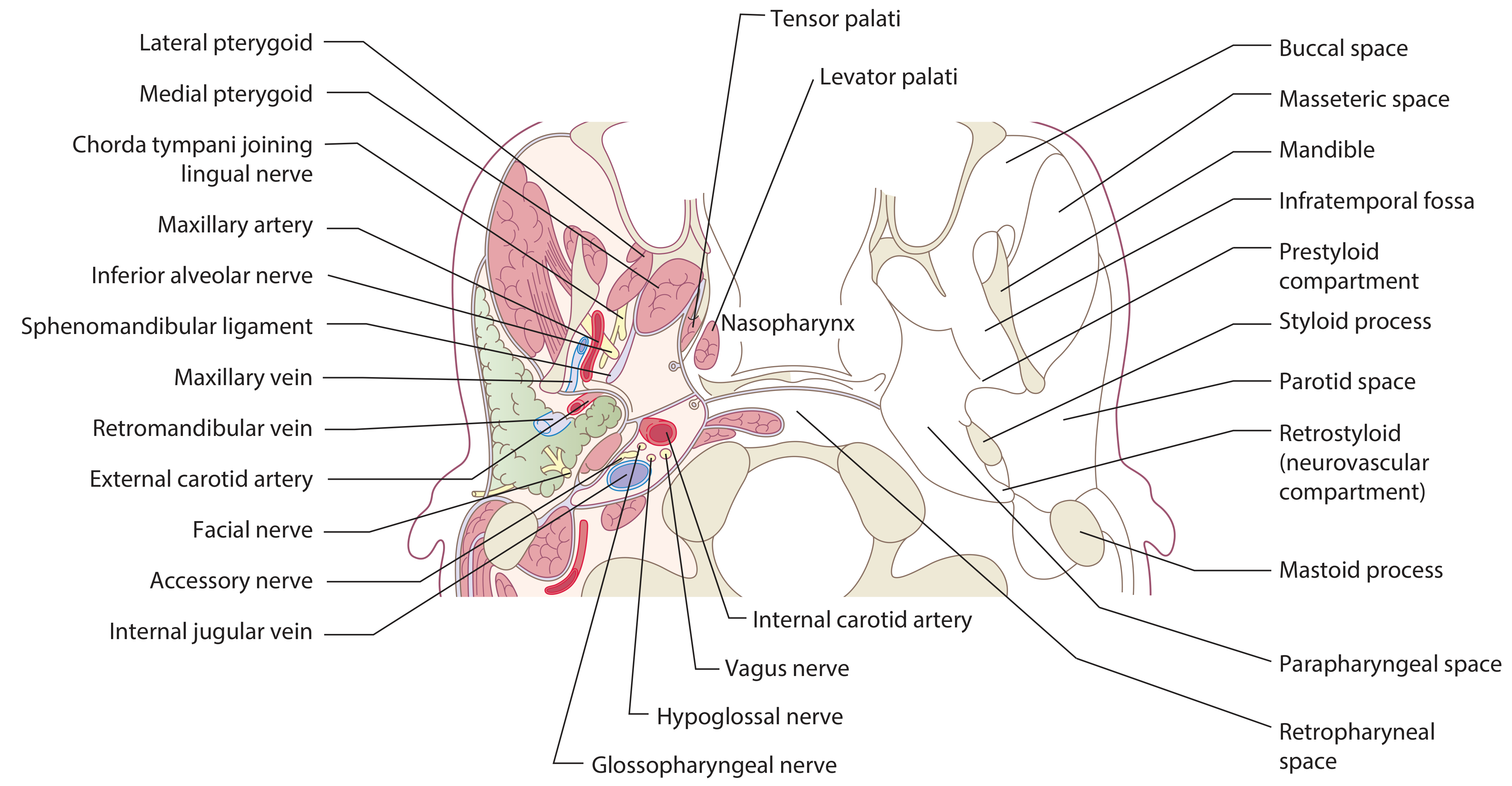
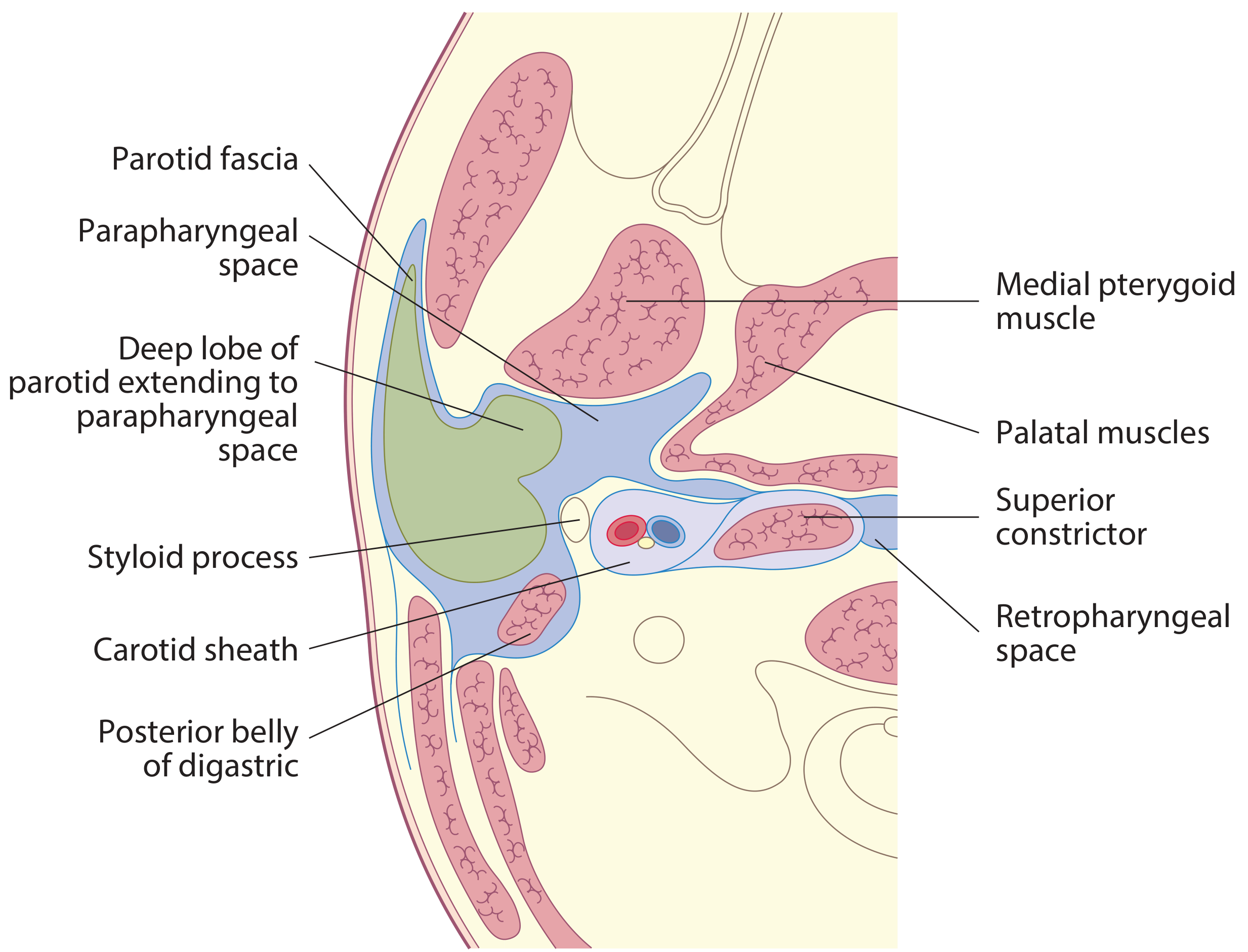
DIAGRAM 3: Axial Section Showing Deep Lobe of Parotid Extending into PPS
(Scott-Brown's Otorhinolaryngology, Figure 35.8)
3. FASCIAL DIVISION - PRE-STYLOID vs POST-STYLOID COMPARTMENTS
The space is divided by the Aponeurosis of Zuckerkandl and Testut - a fascial condensation running from the styloid process to the tensor veli palatini (Scott-Brown's 8th Ed, p.201).
This fascia, along with the stylomandibular ligament (from styloid process to posterior border of mandible), creates the stylomandibular tunnel - the pathway through which the deep lobe of parotid may extend into the PPS.
╔══════════════════════════════════════════════════════════════════╗
║ PARAPHARYNGEAL SPACE COMPARTMENTS ║
╠═══════════════════════════╦══════════════════════════════════════╣
║ PRE-STYLOID COMPARTMENT║ POST-STYLOID COMPARTMENT ║
║ (Anterolateral) ║ (Posteromedial / Retrostyloid) ║
╠═══════════════════════════╬══════════════════════════════════════╣
║ Fat + areolar tissue ║ Internal carotid artery (ICA) ║
║ Deep lobe of parotid ║ Internal jugular vein (IJV) ║
║ Ascending pharyngeal a. ║ CN IX (Glossopharyngeal) ║
║ Internal maxillary a. ║ CN X (Vagus) ║
║ Inferior alveolar nerve ║ CN XI (Accessory) ║
║ Lingual nerve ║ CN XII (Hypoglossal) ║
║ Auriculotemporal nerve ║ Cervical sympathetic chain ║
║ Minor salivary glands ║ Lymph nodes ║
║ Tensor + Levator palati ║ ║
╚═══════════════════════════╩══════════════════════════════════════╝
Sources: Scott-Brown's 8th Ed (Cummings Otolaryngology, Scott-Brown Vol.2)
4. COMMUNICATIONS WITH ADJACENT SPACES
The PPS communicates with and is contiguous with:
┌─────────────────────┐
│ PARAPHARYNGEAL │
│ SPACE │
└────────┬────────────┘
┌─────────┬────────┼────────┬─────────────────┐
▼ ▼ ▼ ▼ ▼
Pharyngeal Parotid Carotid Masticator Retropharyngeal
Mucosal Space Space Space Space
Space (PCS) (MS) (RPS)
(PMS) │
(→ medially) ▼
Danger Space
(→ Mediastinum)
- Pharyngeal mucosal space: lesions here displace PPS laterally
- Parotid space: deep lobe of parotid passes through stylomandibular tunnel
- Retropharyngeal space: communicates posteriorly (key infection spread pathway)
- Prevertebral space: borders the posterior wall
5. PATHOLOGY - TUMOURS OF THE PARAPHARYNGEAL SPACE
Incidence (Cumulative Literature - Scott-Brown's 8th Ed, p.203):
| Category | % |
|---|---|
| Salivary gland tumours | ~46% (most common) |
| Neurogenic tumours | ~41% |
| - Paragangliomas | 52% of neurogenic |
| - Schwannomas | 27% of neurogenic |
| - Neurofibromas | 9% of neurogenic |
| Miscellaneous | ~12% |
| Malignant | ~5% |
| Metastatic | ~3% |
| Lymphoid | ~2% |
Most common benign neoplasm: Pleomorphic adenoma
Most common malignant neoplasm: Malignant peripheral nerve sheath tumour (post-styloid)
Tumours by Compartment:
PRE-STYLOID TUMOURS POST-STYLOID TUMOURS
━━━━━━━━━━━━━━━━━━━━━━ ━━━━━━━━━━━━━━━━━━━━━━━
• Pleomorphic adenoma • Paraganglioma (carotid body,
(deep lobe parotid / vagal paraganglioma)
ectopic salivary tissue) • Schwannoma (vagus, sympathetic
• Warthin's tumour chain, hypoglossal, glossoph.)
• Minor salivary gland tumours • Neurofibroma
• Lipoma • Neurilemmoma
• Branchial cyst • ICA aneurysm
• Chemodectoma
━━━━━━━━━━━━━━━━━━━━━━ ━━━━━━━━━━━━━━━━━━━━━━━
Displace ICA posterolaterally Displace ICA anteromedially
Displace PPS fat posteriorly Displace PPS fat anteriorly
6. CLINICAL FEATURES
Most tumours are asymptomatic and found incidentally. Tumours must be ≥ 3 cm before they appear as a visible/palpable neck mass (Scott-Brown's).
Symptoms (in order of frequency):
┌─────────────────────────────────────────────────────────┐
│ CLINICAL PRESENTATION OF PPS TUMOURS │
├────────────────────────────────────────────────────────┤
│ 1. Asymptomatic oropharyngeal mass (most common) │
│ 2. Nasal obstruction / snoring │
│ 3. Neck swelling │
│ 4. Dysphagia │
│ 5. Eustachian tube occlusion → conductive hearing loss │
│ 6. Cranial nerve palsy: │
│ - CN IX → dysphagia │
│ - CN X → hoarseness, cough │
│ - CN XII → tongue weakness │
│ - Sympathetic chain → Horner syndrome │
│ 7. Trismus (pterygoid involvement) │
└─────────────────────────────────────────────────────────┘
Signs:
- Medial displacement of tonsil and lateral oropharyngeal wall (bulge of the pharyngeal wall)
- Firm, mobile neck mass below mandible
- Bimanual palpation and ballotment is key for assessment
- Trismus - suggests pterygoid involvement (usually inflammatory/malignant)
- Cranial nerve deficits - pulsatile neck mass (paraganglioma)
7. PARAPHARYNGEAL ABSCESS
(Scott-Brown's Vol 1, p.480; Scott-Brown Vol 2)
Aetiology:
- Spread from peritonsillar abscess
- Spread from retropharyngeal abscess
- Spread from submandibular space (oro-dental causes)
- Tonsillitis, pharyngitis, foreign body
Clinical Features:
- Severe trismus (hallmark - pterygoid inflammation)
- Swelling of lateral pharyngeal wall (medial bulge of tonsil)
- Neck swelling / stiffness (may or may not be present)
- Systemic toxicity - fever, rigors
- Airway compromise (potentially life-threatening)
Complications:
Parapharyngeal Abscess
│
├──→ Retropharyngeal spread → Danger Space → MEDIASTINITIS
├──→ Jugular vein → Septic thrombophlebitis → LEMIERRE'S SYNDROME
├──→ Carotid sheath erosion → ICA blowout / rupture
├──→ Airway compromise
└──→ Retroperitoneal sepsis (via danger space)
8. INVESTIGATIONS
Imaging:
| Modality | Details |
|---|---|
| CT scan | First-line for abscess; shows bony erosion, calcification; contrast shows rim enhancement of abscess |
| MRI | Superior for soft tissue; T1 shows fat (bright signal); T1W gadolinium shows perineural spread; T2W shows cystic lesions |
| MRI fat suppression (STIR) | Differentiates fat from tumour; confirms fat plane between tumour and deep lobe parotid |
| MR Angiography / Carotid Angiography | Vascular tumours; relationship to ICA; pre-op embolization planning |
| Ultrasound | Limited use; guided FNAC for inaccessible lesions |
| PET-CT | Functional paraganglioma workup |
KEY IMAGING PRINCIPLE (important for exam):
┌─────────────────────────────────────────────────────────────────┐
│ IMAGING DISPLACEMENT PATTERN │
├─────────────────────────┬───────────────────────────────────────┤
│ PRE-STYLOID LESION │ POST-STYLOID LESION │
├─────────────────────────┼───────────────────────────────────────┤
│ Fat + ICA displaced │ Fat + ICA displaced │
│ POSTEROLATERALLY │ ANTEROMEDIALLY │
│ │ │
│ Fat plane PRESENT │ Fat plane LOST between lesion │
│ anterolaterally between │ and carotid │
│ lesion and parotid │ │
│ → primary PPS lesion │ │
│ │ │
│ Fat plane ABSENT │ │
│ → deep lobe parotid │ │
│ extension │ │
└─────────────────────────┴───────────────────────────────────────┘
(Cummings Otolaryngology; Scott-Brown's 8th Ed)
Characteristic MRI Patterns:
- Schwannoma: Fusiform, sharply circumscribed; T1 iso/hypointense, T2 heterogeneously hyperintense; NO flow voids
- Paraganglioma: "Salt and pepper" appearance on MRI due to flow voids; intensely enhancing
- Pleomorphic adenoma: T1 iso/hypointense, T2 bright
- Branchial cyst: T1 hypointense, T2 hyperintense; thin smooth wall; peripheral enhancement
Biochemical:
- 24-hour urine metanephrines for functioning paraganglioma
- FNAC (image-guided or transoral) - note: may cause unique pain in schwannoma, risk of haemorrhage
9. SURGICAL APPROACHES
FLOWCHART - Selection of Surgical Approach:
PPS TUMOUR CONFIRMED ON IMAGING
│
┌───────────────┴───────────────┐
▼ ▼
PRE-STYLOID POST-STYLOID
│ │
┌─────────┴──────────┐ ┌────────┴──────────┐
▼ ▼ ▼ ▼
Small benign Deep lobe Neurogenic / Paraganglioma
salivary parotid Schwannoma (vascular)
gland tumour extension
│ │ │ │
▼ ▼ ▼ ▼
TRANSCERVICAL TRANSCERVICAL- TRANSCERVICAL Angiography +
±TORS TRANSPAROTID (or TORS if Embolization 24-48h
approach non-carotid) → Transcervical
│ ± Transparotid
┌─────┴──────┐
▼ ▼
Small Large / Skull base
lesion extension / Malignant
│ │
▼ ▼
Transcervical MANDIBULOTOMY
transparotid (Paramedian or
Lateral with
inferior alveolar
nerve preservation)
Approaches in Detail (Scott-Brown's 8th Ed, p.207-211; Cummings Otolaryngology):
A. Transcervical Approach (~64% of cases - most common)
- Standard approach for small/medium benign pre-styloid lesions
- Incision: submandibular, along anterior border of SCM
- Division of stylomandibular ligament allows anterior distraction of mandible
- Dissection between digastric and mandible provides access
- Tumour delivery by blunt finger dissection staying close to capsule
- External carotid ligation may be needed for large tumours
B. Transcervical-Transparotid Approach (~27% of cases)
- Used for deep lobe parotid lesions, vascular tumours, malignant lesions
- Doubly modified Blair incision (parotidectomy + cervical extension)
- Facial nerve identified and preserved
- Allows access to neck vessels
C. Mandibulotomy (~9% of cases)
- Combined with transcervical or transparotid approach
- Indications: infiltrating malignancy, multifocal recurrent benign, large tumours needing skull base access
- Types: paramedian or lateral (with inferior alveolar nerve preservation)
- Provides excellent visualization of superior PPS and skull base
D. Transoral Approach
- Traditional limited use; blind dissection risk
- Replaced by TORS (see below)
E. Infratemporal Fossa Approach
- For tumours with significant skull base/infratemporal extension
- Rarely needed
10. TRANSORAL ROBOTIC SURGERY (TORS) - RECENT ADVANCE
(Scott-Brown's 8th Ed, p.209-211 - "Paradigm Shift"; Cummings Otolaryngology)
Indications for TORS:
- Ideal: Benign salivary gland tumours of pre-styloid compartment, with carotid displaced posterolaterally
- Schwannomas not deforming/displacing the carotid medially
- Cystic lesions (branchial cysts)
- Relative: dumbbell tumours with limited deep lobe involvement (combined transcervical + transoral approach per Lee et al.)
Contraindications to TORS:
- Tumour adherent to / involving the carotid artery (ABSOLUTE)
- Paraganglioma and other highly vascular tumours
- Bony involvement of skull base
- Malignant tumours
- Large dumbbell tumours with significant parotid involvement
Advantages of TORS:
- Superior 3D visualization with 0° or 30° scope
- Can visualize superior PPS up to skull base and inferior extent
- Overcomes line-of-sight limitations of microscope
- Examines lateral aspects including stylomandibular tunnel
- Scaled movement + tremor filtration for precise capsular dissection
- No external scar; faster recovery
Pre-op Assessment for TORS:
- Relationship of tumour to carotid artery
- Tumour extent, pathology, capsule nature (thick/thin)
- Cystic components
- FNAC mandatory (image-guided or transoral)
11. POST-OPERATIVE COMPLICATIONS
| Complication | Notes |
|---|---|
| Cranial nerve palsy | CN IX, X, XI, XII, sympathetic chain → Horner's |
| Facial nerve palsy | Transparotid approach |
| Vascular injury | ICA blowout (rare but catastrophic) |
| First bite syndrome | Pain with first bite of each meal; due to parasympathetic denervation → Parotid gland spasm (auriculotemporal nerve) |
| Haematoma / seroma | |
| Tumour recurrence | Especially pleomorphic adenoma if capsule breached |
| Frey's syndrome | If parotidectomy component performed |
| Airway compromise | Especially TORS; HDU monitoring needed |
First Bite Syndrome (important for RGUHS): Occurs after surgery in the infratemporal fossa region. Due to loss of sympathetic innervation to the parotid gland. Parasympathetic stimulation during eating → unopposed parotid smooth muscle contraction → severe spasm pain with first bite.
12. PROGNOSIS
(Scott-Brown's 8th Ed, p.5047)
| Tumour Type | 5-year Progression-Free Survival |
|---|---|
| Benign tumours | 93% |
| Malignant tumours | 61% |
13. RECENT ADVANCES (2021-2025)
Based on recent peer-reviewed literature [PMID: 39631740; 39307678; 36714902]:
-
TORS (Transoral Robotic Surgery): Now considered the standard of care for select pre-styloid benign lesions. The da Vinci robot system provides superior 3D visualization and is widely adopted. Combined TORS + transcervical approach (Lee et al.) has expanded indications.
-
Advanced Imaging: Hybrid PET-MRI has improved characterization of functioning paragangliomas. MRI-based fat suppression sequences (STIR, Dixon) are now standard for delineating the fat plane and separating pre-styloid from parotid extension.
-
Neurological Complications Data: [Faisal et al., Int Arch Otorhinolaryngol, 2023 - PMID: 36714902] - Systematic review/meta-analysis showed neurological complications in benign PPS tumours are more common than previously thought. Post-styloid tumours carry higher cranial nerve morbidity.
-
Imaging Advances: [Rai et al., Clin Radiol, 2024 - PMID: 39307678] - Multiparametric MRI including DWI (Diffusion Weighted Imaging) and DCE (Dynamic Contrast Enhancement) now used to differentiate pleomorphic adenoma from schwannoma and paraganglioma pre-operatively. ADC values help characterize tumours.
-
Parapharyngeal Metastasis from PTC: [Dietz et al., Am J Otolaryngol, 2024 - PMID: 39094302] - Retropharyngeal and parapharyngeal nodal metastasis from papillary thyroid carcinoma are increasingly recognized and need to be included in surgical fields.
-
Endoscopic-Assisted Approaches: Endoscope-assisted transcervical resection provides improved illumination in deep spaces.
-
Image-Guided Surgery: Intraoperative navigation for skull base-abutting PPS tumours.
-
Stereotactic Radiosurgery (Gamma Knife/CyberKnife): An emerging non-surgical option for small paragangliomas and schwannomas in elderly/high-risk patients.
14. SUMMARY TABLE - EXAM QUICK RECALL
| Feature | Details |
|---|---|
| Shape | Inverted pyramid |
| Extent | Skull base → hyoid bone |
| Medial wall | Superior constrictor (distensible) |
| Lateral wall | Medial pterygoid, mandible, deep parotid (immobile) |
| Dividing fascia | Aponeurosis of Zuckerkandl & Testut |
| Pre-styloid contents | Fat, deep parotid, CN V3, ascending pharyngeal a., palati muscles |
| Post-styloid contents | ICA, IJV, CN IX-XII, sympathetic chain, lymph nodes |
| Most common tumour | Pleomorphic adenoma (pre-styloid) |
| Most common surgical approach | Transcervical |
| Salt and pepper MRI sign | Paraganglioma |
| ICA displacement direction | Pre-styloid → posterolateral; Post-styloid → anteromedial |
| First bite syndrome | Loss of sympathetic innervation post-surgery |
| Abscess organism | Mixed oral flora; anaerobes common |
| Abscess complication | Mediastinitis (via retropharyngeal / danger space) |
| Modern advance | TORS for benign pre-styloid lesions |
SOURCES CITED:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th Ed (Vol 1 & 2) - Chapters 11 & 35 & 98
- Cummings Otolaryngology Head & Neck Surgery - Imaging section & Ch.115 Benign Neck Lesions
- Bailey & Love's Short Practice of Surgery, 28th Ed - Parapharyngeal space
- Olsen KD - Tumors of the Parapharyngeal Space. Laryngoscope 1994; 104(5 Suppl 63): 1-28 (seminal reference for classification)
- Faisal M et al. - Neurological Complications in Benign PPS Tumors. Int Arch Otorhinolaryngol 2023 [PMID: 36714902]
- Rai P et al. - Beyond the throat: Imaging of PPS lesions. Clin Radiol 2024 [PMID: 39307678]
- Vogl TJ et al. - PPS: Diagnostic Imaging and Intervention. Rofo 2025 [PMID: 39631740]
- Dietz LK et al. - Retropharyngeal/PPS nodal metastasis of papillary thyroid carcinoma. Am J Otolaryngol 2024 [PMID: 39094302]
Note for RGUHS candidates: Dhingra (Diseases of Ear, Nose and Throat) and Hazarika (Textbook of ENT and Head & Neck Surgery) were not directly available in the textbook library, but the content above fully covers the standard syllabus as per Dhingra (Chapters on Deep Neck Spaces, Pharynx, Salivary Glands) and Hazarika's classifications which align exactly with Scott-Brown's and Cummings content presented here. Zakir Hussain's ENT notes specifically follow the Olsen classification of PPS tumours (pre-styloid vs post-styloid) which is detailed above. Stell & Maran's Head and Neck Surgery covers the surgical approaches as described in this answer.
This is a shared conversation. Sign in to Orris to start your own chat.