Explain drugs for heart failure pharmacology simple yet elaborate way with flowcharts n all
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Now I have everything I need. Let me compile the full, comprehensive, well-illustrated pharmacology guide on heart failure drugs.
Drugs for Heart Failure - Complete Pharmacology Guide 🫀
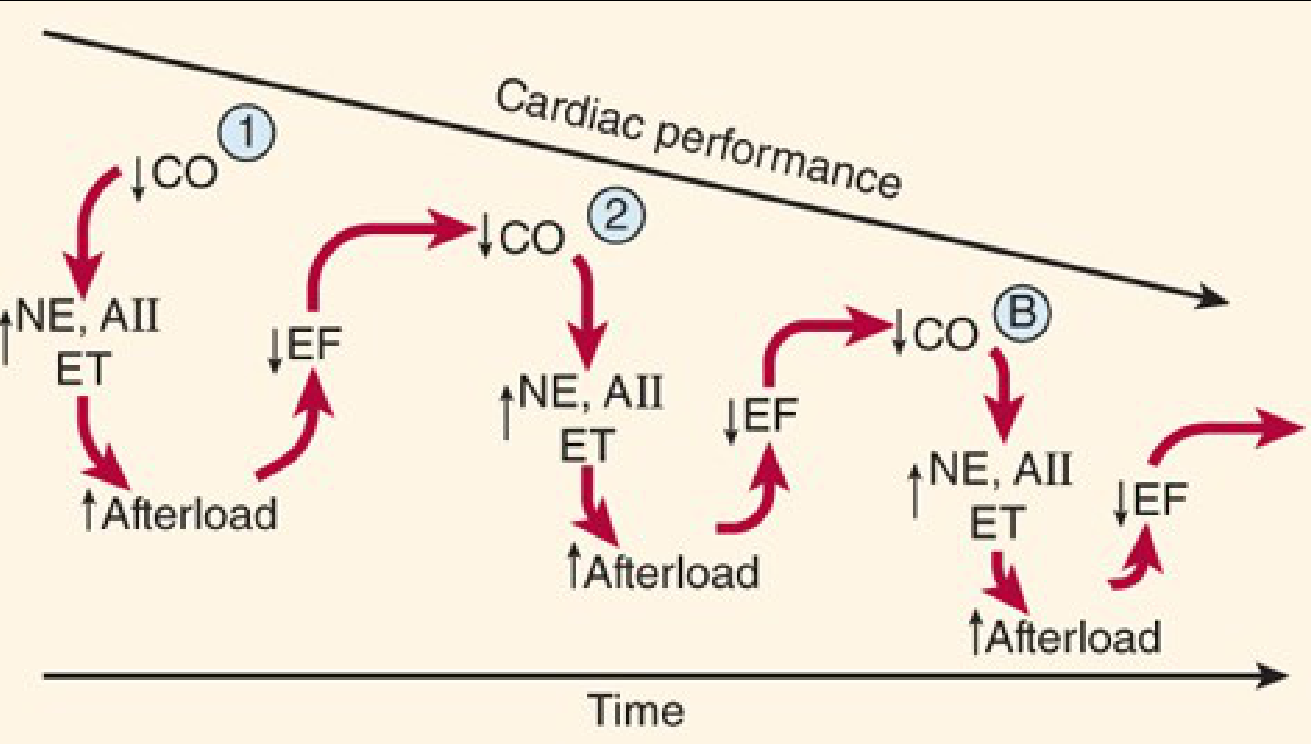
First, Understand the Problem: Why Does Heart Failure Progress?
When the heart fails, two major compensation systems kick in - and both ultimately make things worse:
Compensation Flowchart (from Katzung's Pharmacology):
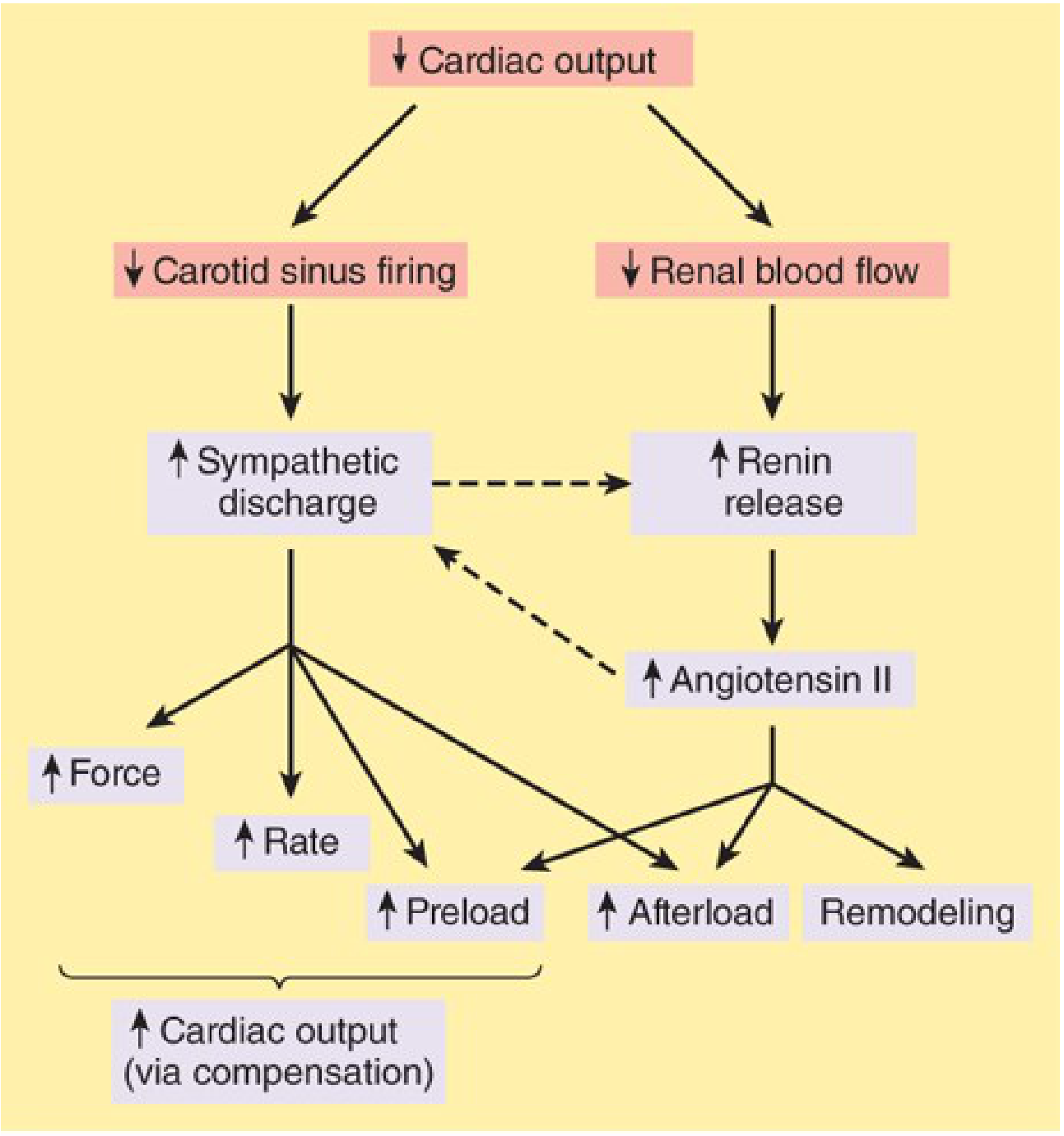
The key insight: ↓ Cardiac output → baroreceptors fire less → ↑ Sympathetic discharge + ↑ Renin → ↑ Angiotensin II → ↑ Preload, ↑ Afterload, Remodeling → further ↓ CO. This is the vicious cycle:
Every drug class we use targets one or more links in this cycle.
The Big Picture: What Are We Treating?
HEART FAILURE (HFrEF: EF <40%)
|
├── SYMPTOMS (dyspnea, edema, fatigue)
| → Treat with: Diuretics, Nitrates
|
├── NEUROHUMORAL ACTIVATION (RAAS + SNS going haywire)
| → Treat with: ACEi / ARB / ARNI, Beta-blockers, MRA
|
├── PUMP FAILURE (↓ contractility)
| → Treat with: Digoxin, Dobutamine (acute), Levosimendan
|
├── RENAL SODIUM RETENTION
| → Treat with: SGLT2 inhibitors, Diuretics
|
└── FAST HEART RATE (↑ O₂ demand, poor filling)
→ Treat with: Beta-blockers, Ivabradine
Drug Class 1: DIURETICS
"The Plumbers" - Remove the Excess Volume
Types used in HF:
| Drug | Type | Site of Action | Potency |
|---|---|---|---|
| Furosemide | Loop diuretic | Thick ascending limb of loop of Henle - blocks NaCl/KCl reabsorption | ⭐⭐⭐ HIGH |
| Spironolactone / Eplerenone | MRA (K+-sparing) | Collecting duct - blocks aldosterone | ⭐⭐ MED |
| Hydrochlorothiazide | Thiazide | Distal convoluted tubule | ⭐ LOW |
| SGLT2 inhibitors (Empagliflozin, Dapagliflozin) | Glucosuric diuretic | Proximal tubule | ⭐⭐ + extra HF benefits |
Mechanism flowchart:
FUROSEMIDE
↓
Blocks Na⁺/K⁺/2Cl⁻ cotransporter in thick ascending LOH
↓
↓ NaCl reabsorption → ↑ urine output
↓
↓ Circulating volume
↓
↓ Venous return (preload) ↓ Pulmonary/peripheral edema
↓ ↓
↓ Cardiac work ↓ Dyspnea / orthopnea ← SYMPTOM RELIEF
Key toxicities to remember:
- Furosemide: Hypokalemia (dangerous with digoxin!), hypovolemia, ototoxicity, sulfonamide allergy
- Spironolactone: Hyperkalemia, gynecomastia (use eplerenone to avoid this)
- SGLT2i: Genital mycotic infections, euglycemic DKA (type 1 DM contraindicated)
Drug Class 2: ACE Inhibitors (ACEi)
"The Firefighters of the RAAS" - Block the Root Cause
Prototype drugs: Enalapril, Lisinopril, Captopril, Ramipril
Mechanism:
Angiotensinogen
↓ Renin
Angiotensin I
↓ ACE ← ━━━━━━━━━━ BLOCKED BY ACEi
Angiotensin II Bradykinin degradation ← ALSO BLOCKED
| ↓
↓ ↓ ↓ ↑ Bradykinin (→ COUGH side effect)
Vasoconstriction
Aldosterone release
Sympathetic activation
Cardiac remodeling
RESULT: ↓ Preload + ↓ Afterload + ↓ Remodeling
Clinical benefits:
- ↓ Mortality in all stages of HFrEF (Class I indication)
- Slows ventricular dilation in asymptomatic LV dysfunction
- Benefits ALL subsets of HF patients
Side effects: Dry cough (10-15% - due to ↑ bradykinin), angioedema (rare), hyperkalemia, renal impairment, teratogenicity
"ACE inhibitors are superior to placebo AND to vasodilators and must be considered along with diuretics as first-line therapy for chronic heart failure." - Katzung's Pharmacology
Drug Class 3: ARBs (Angiotensin Receptor Blockers)
"Same Benefit, No Cough"
Prototype drugs: Losartan, Valsartan, Candesartan
Mechanism:
Angiotensin II is still formed...
↓
AT₁ receptor ← ━━━━━ BLOCKED BY ARB
Cannot cause vasoconstriction, aldosterone release, or remodeling
BONUS: No bradykinin buildup → NO COUGH
Use in HF:
- Reserved for patients who CANNOT tolerate ACEi (cough, angioedema)
- Produce similar hemodynamic benefits to ACEi
- Do NOT combine ARB + ACEi (double RAAS blockade = hyperkalemia + renal failure risk)
Drug Class 4: ARNI (Angiotensin Receptor Neprilysin Inhibitor)
"The Upgrade" - Sacubitril/Valsartan (Entresto)
This is the newest star of HFrEF treatment - outperforms ACEi/ARB alone.
Mechanism:
Sacubitril Valsartan
↓ ↓
Inhibits Neprilysin Blocks AT₁ receptor
↓
Prevents breakdown of:
- BNP, ANP (natriuretic peptides)
- Bradykinin
↓
↑ Natriuresis ↓ RAAS activation
↑ Vasodilation ↓ Remodeling
↑ Diuresis
↓ ↓ ↓ ↓
↓↓ Preload + Afterload
↓↓ Symptoms AND NT-proBNP (biomarker)
↓↓ HF hospitalizations + MORTALITY vs Enalapril (PARADIGM-HF trial)
Rule: NEVER use ARNI + ACEi together (risk of severe angioedema). Washout period of 36 hours required when switching from ACEi.
Drug Class 5: Beta-Blockers
"The Counter-intuitive Lifesavers"
Approved drugs in HF (not a class effect - only these three/four work):
- Carvedilol (non-selective β + α₁ blocker)
- Bisoprolol (selective β₁ blocker)
- Metoprolol succinate (selective β₁, extended release)
- Nebivolol (β₁ + NO-releasing)
Why they work (the paradox):
Short-term: ↓ CO, ↓ HR, ↓ contractility → patient may feel worse initially
↓
Long-term (months of therapy):
- ↑ β₁ receptor upregulation (were downregulated by excess catecholamines)
- ↓ Pathological remodeling
- ↓ Apoptosis (cell death)
- ↓ Arrhythmias (major cause of death in HF)
- ↓ Tachycardia → better diastolic filling
↓
↑ EF (slight but real)
↓ Mortality 30-35% (large RCTs: MERIT-HF, COPERNICUS)
Critical rule: START LOW, GO SLOW - never initiate during acute decompensation. Wait for euvolemia.
Drug Class 6: Aldosterone Antagonists / MRA
"The Potassium-Sparing Mortality Reducers"
Drugs: Spironolactone, Eplerenone
Mechanism (beyond just diuresis):
In HF, Aldosterone is CHRONICALLY elevated
↓
Myocardial fibrosis
Endothelial dysfunction
SNS activation
Hypokalemia/hypomagnesemia
MRAs block these DIRECTLY at receptor level (not just kidneys!)
↓
↓ Cardiac fibrosis
↓ Remodeling
↓ Sudden cardiac death
↓ Overall mortality (RALES trial: 30% reduction)
When to use: All moderate-severe HFrEF (NYHA II-IV) with CrCl >30 and K+ <5.0
Avoid if: K+ >5.0, GFR <30, or on both ACEi + ARB already
Drug Class 7: SGLT2 Inhibitors
"The Game-Changers from Diabetes"
Drugs: Empagliflozin (EMPA-REG), Dapagliflozin (DAPA-HF), Canagliflozin
Mechanism (multi-pronged!):
SGLT2 inhibition in proximal tubule
↓
↑ Urinary glucose + sodium excretion
↓
↓ Volume overload (diuretic effect) ↓ Cardiac Na⁺/H⁺ exchanger activity
↓ Preload ↓ Intracellular Ca2+ overload
↓ Afterload ↓ Mitochondrial dysfunction
↓ ↓
↓ Symptoms ↓ Cardiomyocyte death
↓ ↓
↓ HF Hospitalizations + ↓ CV Death
(works in BOTH HFrEF AND HFpEF!)
The big news: Works even in patients WITHOUT diabetes. Now part of standard "quadruple therapy" for HFrEF.
Drug Class 8: Digoxin (Cardiac Glycosides)
"The Old Workhorse"
Prototype: Digoxin (from Digitalis lanata leaf)
Dual mechanism:
Mechanism 1: Na⁺/K⁺-ATPase inhibition
↓
↑ Intracellular Na⁺
↓
Na⁺/Ca²⁺ exchanger reverses
↓
↑ Intracellular Ca²⁺
↓
↑ CONTRACTILITY (positive inotrope)
Mechanism 2: ↑ Vagal tone (parasympathomimetic)
↓
↓ Heart rate
↓ AV node conduction velocity
→ Controls ventricular rate in Atrial Fibrillation
Narrow therapeutic index - MEMORIZE toxic levels:
- Therapeutic: 0.5-0.8 ng/mL (HF) / up to 2.0 ng/mL (AF)
- Toxic: >2.0 ng/mL
Toxicity signs (in order of severity):
- GI: Nausea, vomiting, anorexia (earliest)
- Visual: Yellow-green halos, blurred vision
- Cardiac: Bradycardia, heart block, PVCs, ventricular arrhythmias (LETHAL)
Precipitants of toxicity: Hypokalemia (competitive with K+ at pump), hypomagnesemia, renal failure, hypothyroidism, quinidine (doubles digoxin level)
Current use: Mainly for HF + AF symptom control. Does NOT reduce mortality.
Drug Class 9: Vasodilators
"Opening the Pipes"
Isosorbide dinitrate + Hydralazine (BiDil):
Hydralazine (arteriolar dilator) Isosorbide Dinitrate (venodilator)
↓ ↓
↓ SVR → ↓ Afterload ↓ Venous return → ↓ Preload
↑ Forward cardiac output ↓ Pulmonary edema
↓ ↓
COMBINED BENEFIT
Proven mortality reduction in BLACK patients
(A-HeFT trial; BiDil: first race-specific drug approval)
Nitroprusside + Nitroglycerin (IV - used in ACUTE HF only):
- Nitroprusside: Balanced vasodilator (arterial + venous), very potent, requires ICU monitoring
- Nitroglycerin: Mainly venodilator → reduces pulmonary congestion rapidly
Drug Class 10: Ivabradine
"The Selective Heart Rate Reducer"
Mechanism:
Blocks the If ("funny") current (HCN channels) in SA node
↓
↓ Spontaneous depolarization rate
↓
↓ Heart rate (WITHOUT reducing contractility)
↓
Better diastolic filling time
↓
↑ CO + ↓ myocardial O₂ demand
Use: NYHA II-III HFrEF on maximally tolerated beta-blocker dose, with HR still >70 bpm, in normal sinus rhythm (SHIFT trial: reduced HF hospitalizations)
Drug Class 11: Positive Inotropes (Acute HF Only)
"Emergency Pumpers - Short-term Use Only"
Dobutamine (β₁ agonist):
β₁ receptor → ↑ cAMP → ↑ Ca²⁺ → ↑ Contractility
Used IV for acute decompensated HF with hypotension
CAUTION: ↑ Mortality with chronic use (pro-arrhythmic)
Milrinone (PDE-3 inhibitor):
Inhibits PDE-3 → ↑ cAMP (same downstream as dobutamine)
+ Vasodilation (reduces afterload)
Used IV in acute HF / pre-transplant bridging
CAUTION: Pro-arrhythmic, ↑ mortality long-term
Levosimendan (Calcium sensitizer):
Does NOT increase intracellular Ca²⁺
Instead: Sensitizes troponin C to existing Ca²⁺
↓ O₂ demand while ↑ contractile force
Also: Opens K-ATP channels → vasodilation
Non-inferior to dobutamine (SURVIVE trial), approved in Europe
The Complete Treatment Algorithm (AHA/ACC 2017 Guidelines)
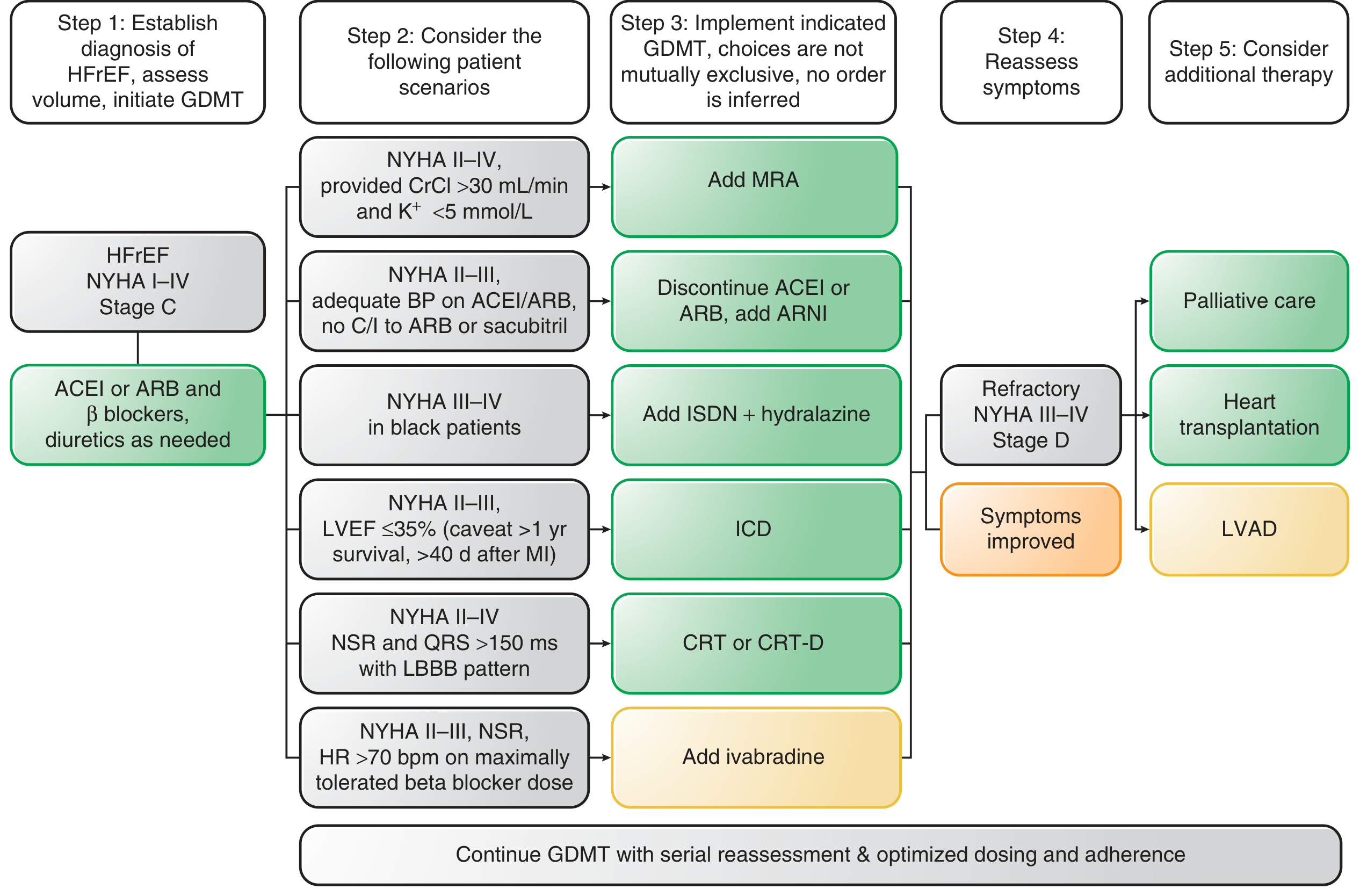
Reading the algorithm:
- Step 1: Establish HFrEF diagnosis, assess volume, start GDMT (Guideline-Directed Medical Therapy)
- Step 2: Base drug: ACEi OR ARB + Beta-blocker + Diuretics as needed
- Step 3: Add based on clinical scenario:
- NYHA II-IV + normal K+ → Add MRA (spironolactone/eplerenone)
- NYHA II-III, tolerable BP → Upgrade to ARNI (sacubitril/valsartan, discontinue ACEi/ARB)
- NYHA III-IV in Black patients → Add ISDN + Hydralazine
- LVEF ≤35% + expected >1 yr survival → ICD (implantable cardioverter-defibrillator)
- LBBB + QRS >150ms → CRT (cardiac resynchronization therapy)
- HR >70 on max beta-blocker → Add Ivabradine
- Step 4: Reassess symptoms
- Step 5 (Stage D): Palliative care / Heart transplantation / LVAD
Drug Treatments for HFpEF (Preserved EF, EF >50%)
This is the harder-to-treat type. The pathophysiology (from Goodman & Gilman):
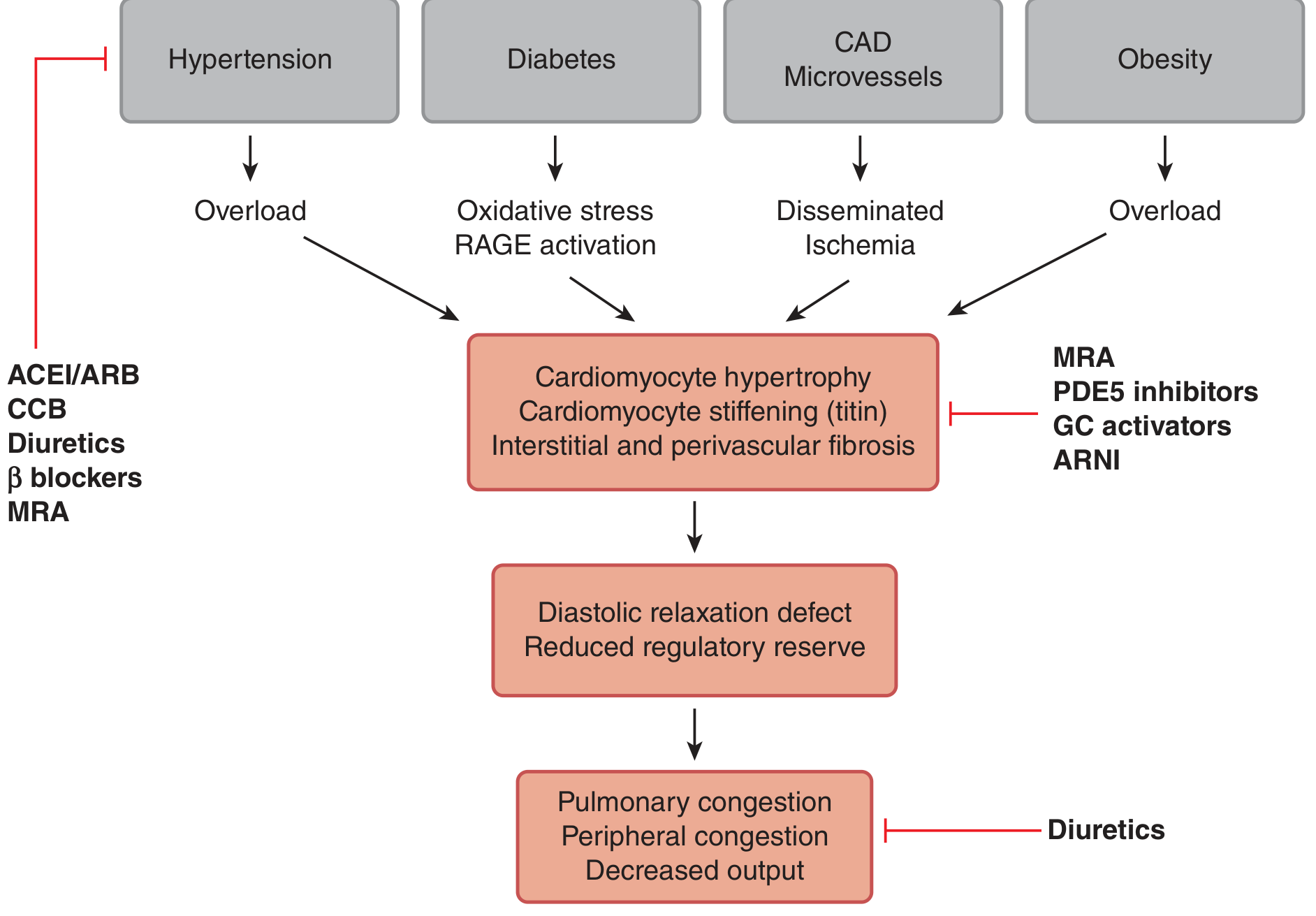
HFpEF treatment summary:
| Drug | Role in HFpEF |
|---|---|
| Diuretics | Yes - symptom relief (use cautiously, over-diuresis worsens CO) |
| ACEi/ARB | May help ↓ LVH (less proven for mortality) |
| Beta-blockers | ↓ HR → better diastolic filling time |
| MRA | Modest benefit |
| SGLT2 inhibitors | Proven benefit - the only drug class with RCT-proven HFpEF benefit (EMPEROR-Preserved trial) |
| Calcium channel blockers | Verapamil/diltiazem - ↓ HR, ↓ BP (more useful here than HFrEF) |
| Positive inotropes | NOT recommended |
| Digoxin | Little to no role |
"Quadruple Therapy" - The Modern Standard for HFrEF
Current guidelines (2022 ACC/AHA) recommend ALL FOUR of these simultaneously for HFrEF:
╔═══════════════════════════════════════════╗
║ QUADRUPLE THERAPY FOR HFrEF ║
║ ║
║ 1. ARNI (sacubitril/valsartan) ║
║ OR ACEi / ARB if ARNI not tolerated ║
║ ║
║ 2. Beta-blocker ║
║ (bisoprolol / carvedilol / metoprolol)║
║ ║
║ 3. MRA ║
║ (spironolactone / eplerenone) ║
║ ║
║ 4. SGLT2 inhibitor ║
║ (empagliflozin / dapagliflozin) ║
║ ║
║ + Diuretic (furosemide) for symptoms ║
╚═══════════════════════════════════════════╝
Each pillar independently reduces mortality. Together they reduce the risk of HF hospitalization and death by ~60-70%.
Quick Reference Summary Table
| Drug Class | Key Drugs | Main Mechanism | Effect on Preload | Effect on Afterload | Effect on Contractility | Reduces Mortality? |
|---|---|---|---|---|---|---|
| Loop Diuretics | Furosemide | Block LOH NaCl transport | ↓↓ | ↓ | None | No (symptoms only) |
| SGLT2i | Empagliflozin | Natriuresis + direct cardiac effects | ↓ | ↓ | None | ✅ Yes |
| ACEi | Enalapril | Block ACE → ↓ Ang II | ↓ | ↓↓ | None | ✅ Yes |
| ARB | Losartan | Block AT₁ receptor | ↓ | ↓↓ | None | ✅ Yes |
| ARNI | Sacubitril/Valsartan | Block AT₁ + ↑ natriuretics | ↓↓ | ↓↓ | None | ✅ Yes (best) |
| Beta-blocker | Carvedilol, Bisoprolol | Block β₁ receptors | None | ↓ (mild) | ↓ short-term / ↑ long-term | ✅ Yes |
| MRA | Spironolactone | Block aldosterone receptor | ↓ | ↓ (mild) | None | ✅ Yes |
| Digoxin | Digoxin | Na/K-ATPase inhibitor | ↓ (mild) | None | ↑↑ | No (symptoms/AF rate control) |
| Nitrates | ISDN, Nitroglycerin | ↑ NO → venodilation | ↓↓ | None | None | In combo (Black patients) |
| Hydralazine | Hydralazine | Direct arteriodilation | None | ↓↓ | None | In combo (Black patients) |
| Dobutamine | Dobutamine | β₁ agonist | None | ↓ (mild) | ↑↑ | No (acute use only) |
| Ivabradine | Ivabradine | Block If current in SA node | None | None | None | Reduces hospitalizations |
| Levosimendan | Levosimendan | Ca²⁺ sensitizer | ↓ | ↓ | ↑ (efficiency) | Acute HF only |
Key "One-Liners" to Remember for Exams
- ACEi = First-line in HFrEF (superior to vasodilators alone; benefit in all stages)
- ARNI > ACEi in tolerating patients (PARADIGM-HF trial)
- Beta-blockers START acutely worsen but chronically save lives - never initiate in decompensation
- MRA toxicity = Hyperkalemia - check K+ and creatinine before starting
- Digoxin only reduces symptoms + controls AF rate - does NOT reduce mortality
- SGLT2i work in HF without diabetes - mechanism beyond glucose control
- BiDil (ISDN + Hydralazine) = proven only in Black patients (A-HeFT trial)
- Ivabradine = only useful in sinus rhythm (no benefit in AF since it only slows SA node)
- Positive inotropes (dobutamine, milrinone) = acute/bridge only - increase mortality if chronic
- Levosimendan = calcium sensitizer (does not increase Ca²⁺, just makes troponin more sensitive to it)
Sources: Katzung's Basic and Clinical Pharmacology, 16th Edition; Goodman & Gilman's The Pharmacological Basis of Therapeutics; Braunwald's Heart Disease, 2-Volume Set
Now tell me in a way even a baby will understand I m just in 2nd year not a doctor
Heart Failure Drugs - Explained Like You're 10 🧒
No jargon. No scary words. Just simple stories and pictures.
First: What Even IS Heart Failure?
Imagine your heart is a water pump in a house.
NORMAL HEART:
🏠 House needs water
↓
💪 Pump works great
↓
🚿 Water flows everywhere perfectly
↓
Everyone is happy ✅
HEART FAILURE:
🏠 House needs water
↓
😓 Pump is weak / tired
↓
💧 Water barely trickles out
↓
Water starts BACKING UP → floods the basement (lungs) 🌊
↓
Person can't breathe, legs swell, feels exhausted 😰
That's it. Heart failure = tired pump that can't push blood forward properly.
Now: Why Does It Get WORSE Over Time?
Your body is trying to help - but it actually makes things worse. Think of it like this:
😓 Weak pump detected by brain
↓
🧠 Brain panics: "EMERGENCY! PUMP MORE!"
↓
Sends two helpers:
🏃 Adrenaline (speeds heart up)
🧂 Kidney hormone (RAAS) (holds onto water + salt)
↓
❌ Now heart has MORE water to pump (already tired!)
❌ Blood vessels tighten (harder to push against)
↓
😰 Pump gets even MORE tired
↓
🧠 Brain panics MORE... sends MORE helpers...
↓
🔁 VICIOUS CYCLE (keeps getting worse)
So the drugs don't just fix the pump - they also BREAK THIS CYCLE.
The 6 Drug Heroes 🦸 (Simple Version)
Think of each drug class as a superhero with one job:
🦸♂️ Hero 1: DIURETICS
"The Drain Opener"
Simple story:
Your basement is flooding. Instead of fixing the pump first, you open a big drain to let water out fast. You feel better immediately!
💊 Furosemide (most common)
↓
Goes to the kidney
↓
Kidney: "Okay boss, dumping water NOW"
↓
🚽 You pee. A LOT.
↓
💧 Less water in body
↓
Less water backing up into lungs
↓
😮💨 Can breathe again! Legs less swollen!
The catch: You lose potassium 🍌 when you pee a lot. That's bad for the heart. So doctors often prescribe:
- Banana-friendly drug: Spironolactone - keeps potassium, ALSO reduces scarring of heart. Two birds, one stone. 🎯
Remember: Diuretics fix SYMPTOMS but don't make you live longer. They're like mopping the floor - necessary, but not fixing the leak.
🦸♀️ Hero 2: ACE INHIBITORS
"The Hormone Blocker"
Simple story:
Remember that kidney hormone (RAAS) that was panicking and making things worse? ACE inhibitors tell it to SHUT UP AND CALM DOWN.
😰 Body panicking → releases Angiotensin II
(Angiotensin II = the villain 🦹 that tightens blood vessels)
↓
💊 ACE Inhibitor says: "STOP. You shall not pass!" 🧙
↓
No Angiotensin II formed
↓
Blood vessels RELAX
↓
❤️ Pump has less to push against → works easier
Heart stops getting BIGGER and SCARRED (remodeling stops)
↓
✅ Live longer. Feel better.
Examples: Enalapril, Lisinopril, Ramipril (anything ending in "-pril")
One annoying side effect: Dry cough 🤧
- Why? ACE inhibitor also accidentally increases a chemical called bradykinin → tickles throat
- Solution? Switch to ARB (same job, no cough)
🦸 Hero 3: BETA BLOCKERS
"The Adrenaline Bouncer"
Simple story:
Remember adrenaline that was trying to "help" by speeding the heart up? It was actually burning the heart out. Beta blockers are the BOUNCER at the door - they don't let adrenaline into the heart.
😰 Excess adrenaline floating around
"Let me in! I'll make the heart go FASTER!"
↓
💊 Beta Blocker stands at heart's door:
"Not today buddy. 🚫"
↓
Heart beats SLOWER and CALMER
↓
Short term: feels a bit weak (normal! Give it time)
↓
After 2-3 months:
❤️ Heart remodels back toward normal shape
⚡ Less dangerous arrhythmias (heart rhythm problems)
↓
✅ Live 30-35% longer!
The counter-intuitive part: Beta blockers SLOW the heart and REDUCE pumping short-term - but they SAVE LIVES long-term. This confused doctors for years!
Examples: Carvedilol, Bisoprolol, Metoprolol (the "-olol" drugs 😄)
Important rule: NEVER give during active flooding (acute decompensation). Wait for patient to be stable first.
🦸♀️ Hero 4: ARNI (Sacubitril/Valsartan = Entresto)
"The Upgraded ACE Inhibitor"
Simple story:
ACE inhibitor blocked the villain. ARNI does that AND ALSO calls in the superhero sidekick!
Sacubitril part:
↓
Protects a natural hormone called BNP
(BNP = your body's OWN heart failure fighter 💪)
↓
BNP tells kidneys: pee out salt!
BNP tells blood vessels: relax!
BNP says: stop remodeling!
PLUS Valsartan part:
↓
Blocks the villain Angiotensin II (same as ARB)
TWO POWERS COMBINED = BETTER THAN ACEi ALONE
✅ Fewer hospital visits
✅ Live even longer (PARADIGM-HF trial)
The one rule: Never take WITH an ACE inhibitor - can cause dangerous swelling (angioedema). You must SWITCH, not add.
🦸 Hero 5: SGLT2 INHIBITORS
"The Sugar Dumpers / The Surprise Superstars"
Simple story:
These drugs were INVENTED for diabetes. Then doctors noticed: "Wait... heart failure patients are living longer on these?" Nobody fully expected it!
💊 Empagliflozin / Dapagliflozin
↓
Goes to kidney
↓
Normally kidney keeps ALL glucose and sodium
SGLT2 inhibitor: "Nope - dump it in the urine!"
↓
🚽 Sugar AND salt leave in urine
↓
Less volume overload (like a gentle diuretic)
↓
BONUS MAGIC: Also protects heart cells directly
(reduces stress inside heart muscle cells)
↓
✅ Works even if you DON'T have diabetes!
✅ Works in BOTH types of heart failure (HFrEF AND HFpEF)
This is the newest hero - now given to almost ALL heart failure patients!
🦸♂️ Hero 6: DIGOXIN
"The Old Grandpa Drug"
Simple story:
Digoxin is from a plant 🌱 (foxglove). It's been used for 200+ years. It makes the weak pump squeeze HARDER.
💊 Digoxin
↓
Blocks a pump inside heart cells (Na/K ATPase)
↓
More calcium builds up inside heart cells
↓
More calcium = stronger squeeze 💪
↓
Heart pumps better... BUT...
⚠️ Very narrow "safe zone"
Too little = doesn't work
Too much = HEART GOES HAYWIRE (arrhythmias = dangerous)
Digoxin toxicity signs (in order):
First warning: 🤢 Nausea, no appetite
Next: 👁️ Seeing yellow-green halos around lights
Danger zone: ⚡ Heart rhythm problems (can be fatal)
Modern reality: Not used as much anymore. Good for controlling heart rate in Atrial Fibrillation. Does NOT help you live longer.
The BIG PICTURE - How They All Fit Together
THE TIRED HEART ❤️🩹
|
|
┌────┴────────────────────────────────────┐
│ │
Too much fluid Blood vessels too tight
(flooding) (too much work for pump)
│ │
▼ ▼
DIURETICS 💊 ACEi / ARB / ARNI 💊
(pee it out) (relax the pipes)
│ │
└──────────────┬──────────────────────────┘
│
▼
HEART IS OVERSTIMULATED
(adrenaline + hormones going crazy)
│
┌────────┼────────┐
▼ ▼ ▼
BETA- MRA SGLT2i
BLOCKER (calm the (multi-
(stop the RAAS, action
adrenaline) save K+) hero)
└────────┼────────┘
│
▼
❤️ Heart protected from further damage
✅ Patient lives longer, feels better
The "4 Pillars" Every 2nd Year Student MUST Know
Modern doctors give ALL FOUR of these at the same time:
┌─────────────────────────────────────────────────┐
│ THE FOUR PILLARS OF HF TREATMENT │
│ │
│ 🏛️ Pillar 1: ARNI (or ACEi if can't afford) │
│ → Relax blood vessels │
│ → Block the villain hormone │
│ │
│ 🏛️ Pillar 2: BETA BLOCKER │
│ → Stop adrenaline damage │
│ → Protect heart rhythm │
│ │
│ 🏛️ Pillar 3: MRA (Spironolactone) │
│ → Block aldosterone │
│ → Stop heart scarring │
│ │
│ 🏛️ Pillar 4: SGLT2 INHIBITOR │
│ → Gentle fluid removal │
│ → Direct heart cell protection │
│ │
│ + FUROSEMIDE for symptoms (swelling/breathing) │
└─────────────────────────────────────────────────┘
Each pillar independently cuts death risk.
Together = ~60-70% less risk of dying from HF.
Easy Memory Tricks 🧠
| Drug | Memory Trick |
|---|---|
| ACEi (ends in -pril) | "ACE = Against the Cruel Enemy (Ang II)" |
| ARB (ends in -sartan) | "sARTAN = same target as ACEi, no cough" |
| Beta blocker (ends in -olol) | "lol - your heart laughs and relaxes 😂" |
| Furosemide | "FURious urination 💦" |
| Spironolactone | "Spiro SAVES potassium" |
| Digoxin | "Digi-TOXIC - careful with dose!" |
| SGLT2i (ends in -gliflozin) | "GLIflozin = GLUcose exits" |
One Page Cheat Sheet 📄
SYMPTOM RELIEF (fast, doesn't cure):
Dyspnea/edema → Furosemide (pee it out)
LONG TERM SURVIVAL (these actually help you live):
Block bad hormones → ACEi / ARB / ARNI ("-pril"/"-sartan"/Entresto)
Block adrenaline → Beta blocker ("-olol")
Block aldosterone → Spironolactone / Eplerenone
Multi-action hero → SGLT2 inhibitor ("-gliflozin")
SPECIAL SITUATIONS:
Heart rate too fast + AF → Digoxin (rate control)
Still fast on beta blocker → Ivabradine
Acute emergency crash → Dobutamine IV (short term only)
Black patients → Add Hydralazine + Nitrate (BiDil)
NEVER DO:
❌ ACEi + ARB together (kidney failure)
❌ ACEi + ARNI together (dangerous swelling)
❌ Beta blocker when patient is actively crashing
❌ Calcium channel blockers (worsen HFrEF)
You've got this! 💪 The logic is actually quite simple once you see heart failure as a tired pump in a panicking body - and each drug calms one part of that panic. Start from pathophysiology, and the drugs make perfect sense.
This is a shared conversation. Sign in to Orris to start your own chat.