Imaging findings of acute appendicitis for postgraduate surgery
Reading File
Finding Sources
Finding Sources
Searching PubMed
"appendicitis"[MeSH Terms] AND "diagnostic imaging"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative surgical textbooks with actual radiological images. Let me compile the complete answer.
Imaging Findings of Acute Appendicitis
Sources: Maingot's Abdominal Operations, Schwartz's Principles of Surgery (11e), Mulholland & Greenfield's Surgery (7e), Yamada's Textbook of Gastroenterology (7e), Sabiston Textbook of Surgery, Rosen's Emergency Medicine
Overview and Indications for Imaging
Imaging is not mandatory in every patient with classic appendicitis. The general indications are:
- Atypical or equivocal clinical presentation
- High operative risk (elderly, pregnant, multiple comorbidities)
- Female patients of reproductive age (to exclude gynaecological pathology)
- Children (to reduce radiation exposure and negative appendectomy rate)
A negative appendectomy rate of <10% in males and <20% in females is considered acceptable; routine cross-sectional imaging reduces this rate further. - Schwartz's Principles of Surgery, p. 1360
1. Plain Abdominal Radiograph
Role: Minimal - not recommended as a primary diagnostic tool.
- A right lower quadrant faecolith (appendicolith) is present in only 10.5% of patients with appendicitis and in 3.3% without appendicitis - it is neither pathognomonic nor sufficiently sensitive
- Present in 9% of non-perforated and 21% of perforated appendicitis specimens
- Plain films are indicated only in elderly patients where a perforated viscus must be excluded - an erect chest X-ray looks for free subdiaphragmatic air - Maingot's Abdominal Operations, p. 646
2. Ultrasound (Graded Compression Ultrasound)
First-line modality in: thin patients, children, pregnant women, young women of reproductive age.
Sensitivity: 76-86% | Specificity: 81-91% (meta-analysis of 14 prospective studies)
Positive Findings
| Finding | Significance |
|---|---|
| Non-compressible tubular structure in RLQ | Primary criterion - the appendix does not collapse on probe pressure |
| Diameter >6 mm (outer wall to outer wall) | Key threshold - distended lumen |
| Target sign (thick-walled, fluid-filled, blind-ending tube) | Characteristic cross-sectional appearance |
| Loss of wall compressibility | Indicates transmural inflammation |
| Increased echogenicity of periappendiceal fat | Indicates surrounding inflammation |
| Loculated pericaecal fluid | Associated finding |
| Hyperaemia on Colour Doppler | Increased mural vascularity |
| Appendicolith with acoustic shadowing | When present, increases specificity |
The collapsed normal appendix is ≤6 mm. A distended but otherwise normal appendix can measure up to 10 mm in healthy patients, so diameter alone is not diagnostic. - Yamada's Gastroenterology, p. 2722
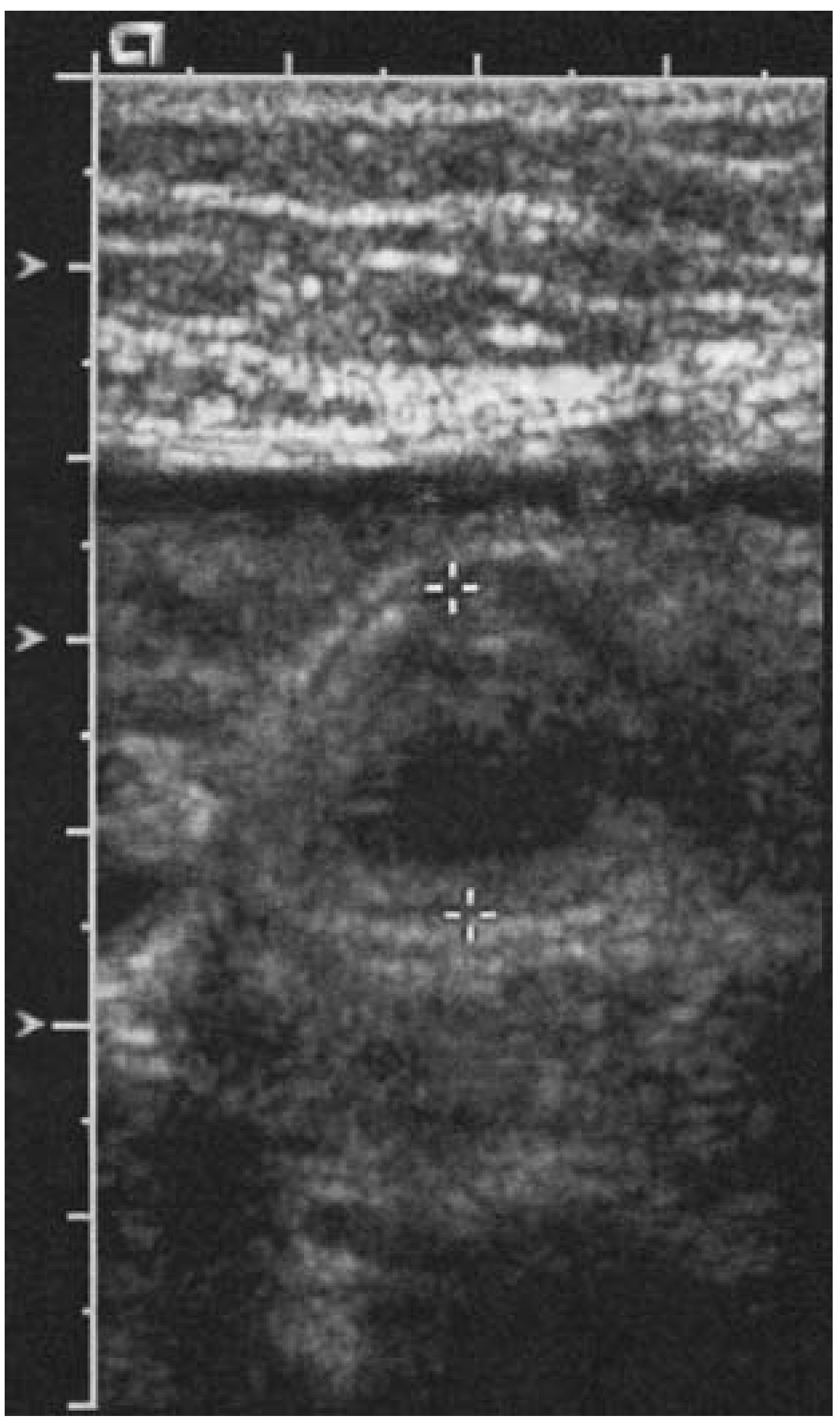
Figure: Appendiceal ultrasound showing a distended, non-compressible appendix - Maingot's Abdominal Operations
Limitations
- Highly operator-dependent
- Cannot visualise the appendix in up to 30-40% of cases (gas, obesity, retrocaecal position)
- Limited in obese patients
- Poor negative predictive value if appendix not visualised
- If ultrasound is negative or inconclusive but clinical suspicion persists, proceed to CT - Rosen's Emergency Medicine
3. Computed Tomography (CT)
Gold-standard modality for most adults.
Sensitivity: 94-97% | Specificity: 89-100% (multiple prospective studies; Schwartz cites 0.96/0.96 from meta-analysis of 12 studies)
Protocol
- IV contrast is essential - highlights mural hyperaemia and periappendiceal inflammation
- Oral/rectal contrast: not required; adds no significant diagnostic benefit and causes delay - Yamada's, Mulholland's
- Low-dose CT is non-inferior to standard dose in young adults (RCT, 891 patients) - Mulholland & Greenfield, p. 3610
- MDCT with multiplanar reconstruction (axial + coronal) is standard
Positive CT Findings - Uncomplicated Appendicitis
| CT Finding | Threshold |
|---|---|
| Enlarged appendiceal lumen | Outer diameter >6 mm (Maingot); some cite >10-13 mm (Mulholland) |
| Wall thickening | >3 mm wall thickness |
| Failure to fill with oral contrast or air | Obstruction of lumen - key finding |
| Periappendiceal fat stranding | Surrounding inflammatory change - most important associated sign |
| Mucosal hyperenhancement on contrast | Prominent in early/moderate disease |
| Appendicolith | Calcified density within the lumen; increases risk of perforation |
| Periappendiceal fluid | Localised free fluid adjacent to appendix |
Appendicitis is effectively excluded when: oral contrast fills the appendiceal lumen and there is no surrounding inflammation. - Maingot's, p. 647
Caveat: CT performed very early in the disease course (<12h of symptoms) may not yet show characteristic findings. In confusing cases, repeat CT after 24h of observation is reasonable. - Maingot's
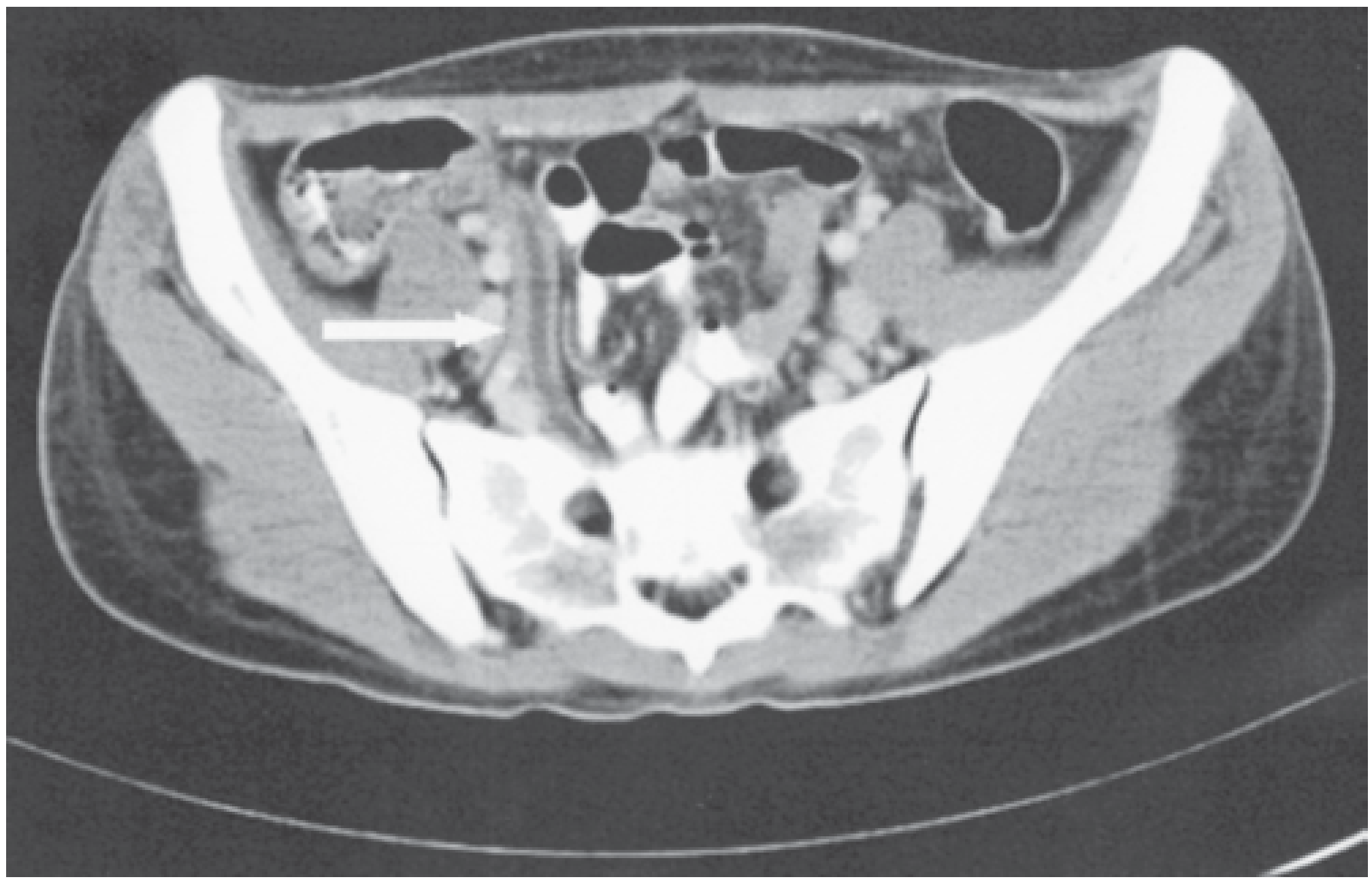
Figure: Axial CT - enlarged, fluid-filled appendix with wall hyperaemia not filling with oral contrast (Maingot's Abdominal Operations)
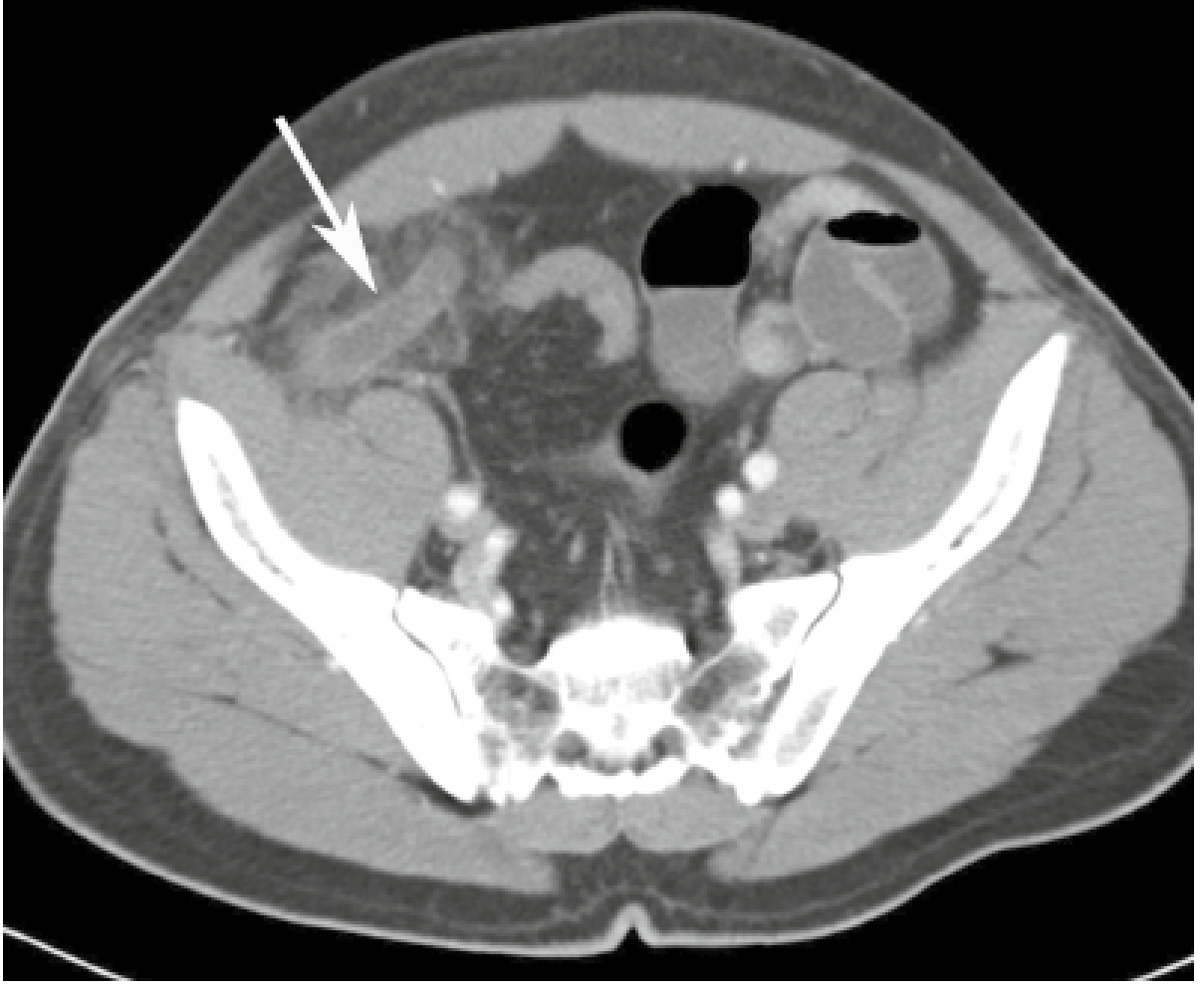
Figure: MDCT - dilated appendix with periappendiceal stranding (Yamada's Gastroenterology, p. 2722)
CT Findings - Complicated Appendicitis (Perforation/Abscess/Phlegmon)
Complicated appendicitis (gangrene, phlegmon, abscess) occurs in up to 10% of acute cases.
| CT Finding | Interpretation |
|---|---|
| Periappendiceal gas | Perforation (extraluminal air) |
| Periappendiceal abscess | Walled-off collection with enhancing rim and central fluid/gas |
| Phlegmon | Inflammatory mass - poorly-defined soft tissue density with fat stranding |
| Free intraperitoneal air | Free perforation |
| Free intraperitoneal fluid | Peritonitis |
| Loss of appendiceal wall integrity | Gangrenous/perforated appendix |
| Appendicolith outside the appendix | Extraluminal appendicolith - confirms perforation |
CT also better visualises abscesses and phlegmons than ultrasound, and provides alternative diagnoses (Crohn's disease, ovarian pathology, Meckel's diverticulitis, right-sided colon cancer). - Maingot's, p. 647
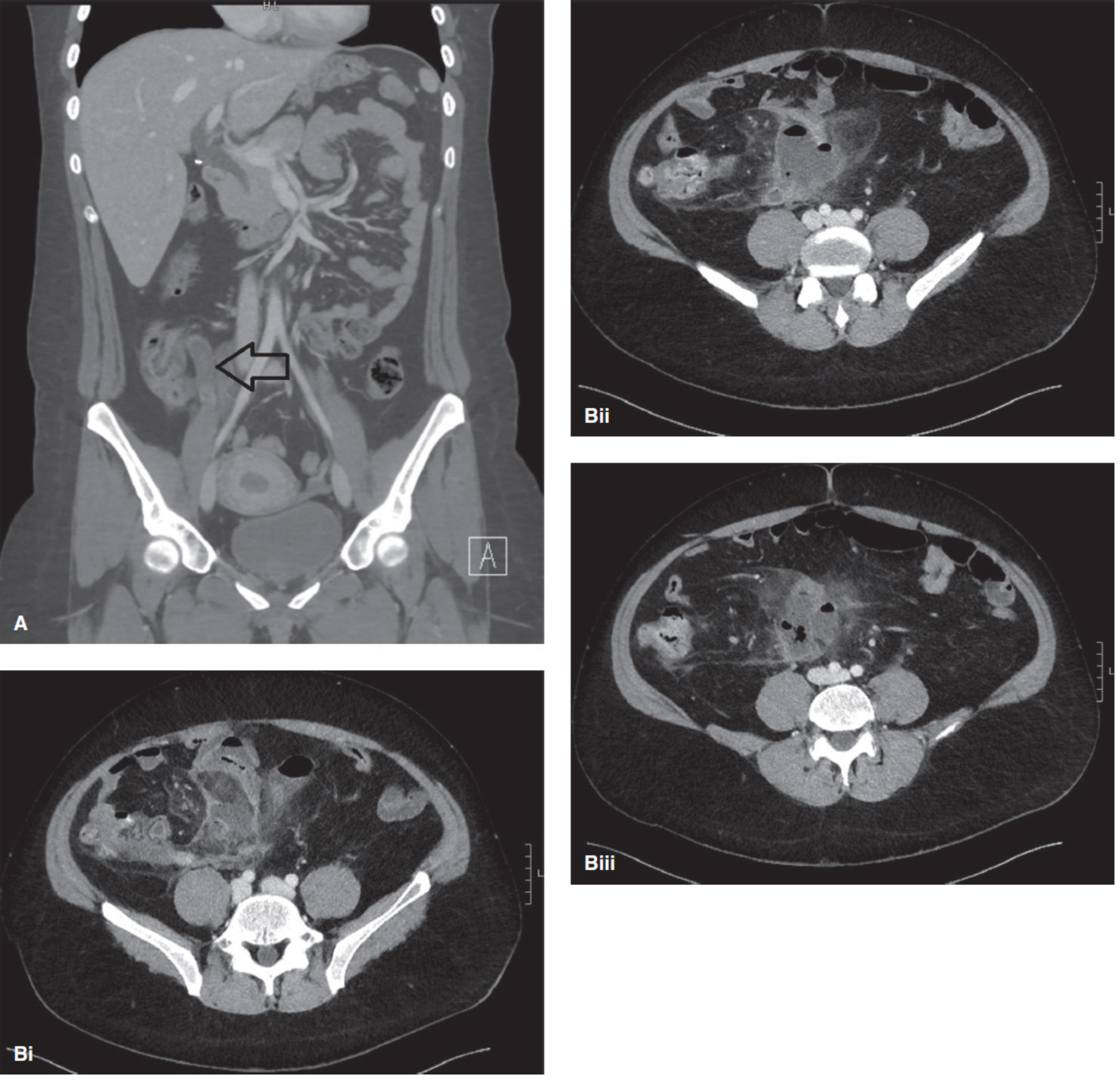
Figure: CT - (A) nonperforated appendicitis with distended thick-walled appendix; (B) perforated appendicitis with adjacent abscess (Mulholland & Greenfield's Surgery, p. 3611)
4. Magnetic Resonance Imaging (MRI)
Preferred in: pregnant patients (when ultrasound is non-diagnostic), children (when radiation must be avoided).
High sensitivity and specificity comparable to CT, without ionising radiation.
Protocol
- T2-weighted sequences are most informative
- Gadolinium contrast is generally avoided in pregnancy (first trimester)
- If used in pregnancy, perform with minimal sequences and patient consent regarding minimal fetal risks
MRI Findings
- Thickened, fluid-filled appendix (T2 hyperintense lumen)
- Periappendiceal oedema (T2 signal in surrounding fat)
- Wall oedema and thickening
- Restricted diffusion on DWI correlates with gangrenous change
Algorithm for pregnant patients: Graded compression ultrasound → if negative/inconclusive → MRI → if MRI unavailable and clinical suspicion high → limited CT with radiation-dose minimisation - Rosen's Emergency Medicine; Sabiston
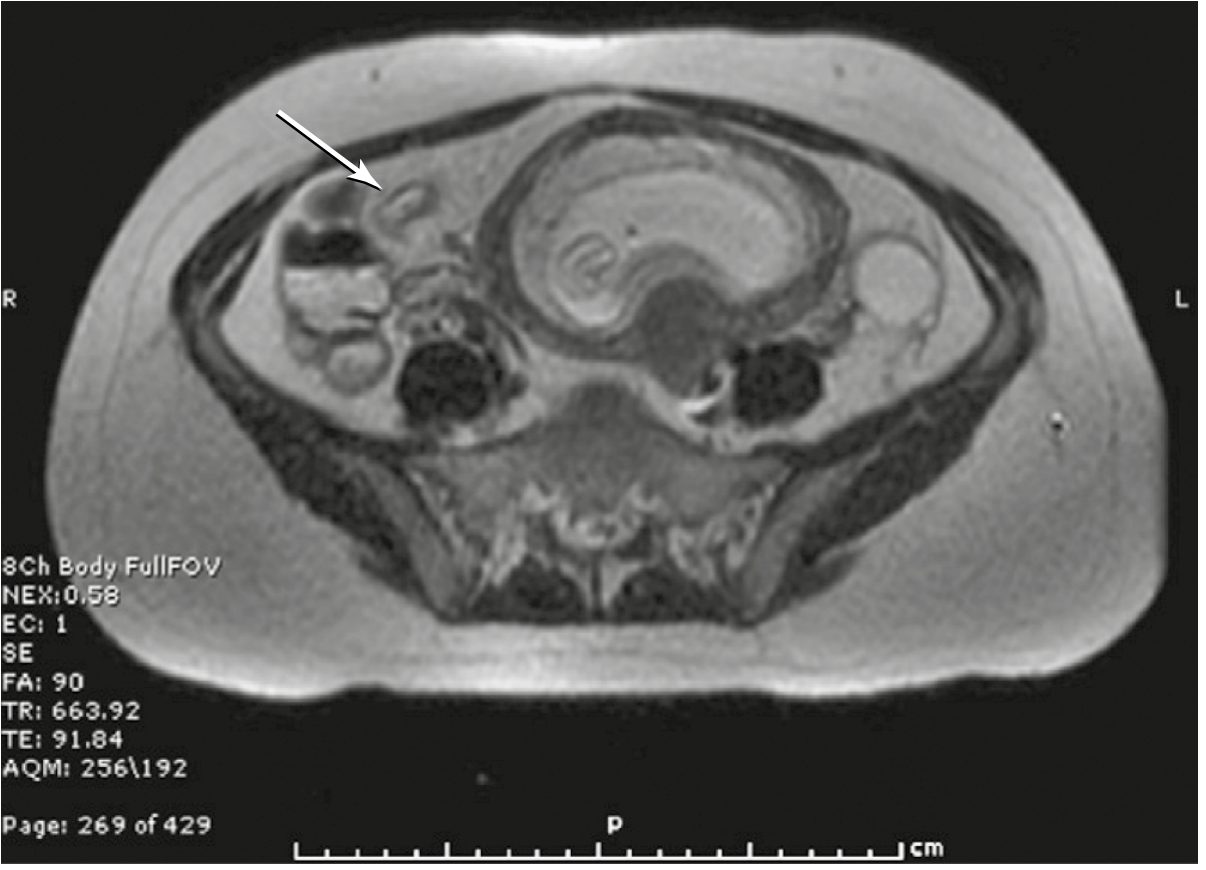
Figure: MRI T1-weighted axial - thickened appendix (arrow) in a gravid patient (Sabiston Textbook of Surgery, p. 2047)
5. Comparative Accuracy
| Modality | Sensitivity | Specificity | Accuracy | Key Advantage |
|---|---|---|---|---|
| CT (contrast) | 94-97% | 89-100% | 94% | Highest accuracy; alternative diagnoses |
| Ultrasound | 76-86% | 81-91% | 83% | No radiation; first-line in pregnancy/children |
| MRI | High (comparable to CT) | High | High | No radiation; pregnant patients |
| Plain X-ray | Poor | Poor | - | Only for free air exclusion |
Data from Balthazar et al. and Horton et al. (Maingot's Table 31-1) and meta-analyses cited in Schwartz's.
6. Recommended Imaging Strategy
Suspected appendicitis
↓
Is the diagnosis clinically clear in a young male?
→ YES: proceed to OR (imaging optional)
→ NO or equivocal: imaging indicated
↓
Pregnant patient? → Graded compression US → MRI if US non-diagnostic
Children? → Graded compression US first → CT if US negative/equivocal
Adult, non-pregnant → CT abdomen/pelvis with IV contrast (no oral/rectal contrast needed)
↓
CT negative, clinical suspicion persists → repeat CT at 24h or diagnostic laparoscopy
High-risk features on imaging that favour surgery over non-operative management:
- Faecolith present
- Abscess or phlegmon
- Appendiceal diameter >11 mm
- Free fluid collection
- Suspected tumour - Rosen's Emergency Medicine
7. Key Points for Postgraduate Surgery Examination
- CT is the gold standard in adults - sensitivity/specificity ~96%/96%; no oral/rectal contrast required
- Ultrasound first-line in children, pregnant women, and thin adults - operator-dependent; if non-diagnostic, proceed to CT
- MRI is the preferred study in pregnancy when ultrasound is equivocal - no ionising radiation
- Plain X-ray has no routine role; indicated only to exclude free perforation in elderly patients
- Appendiceal diameter >6 mm on any modality is the primary threshold (some texts cite 10-13 mm for CT)
- Periappendiceal fat stranding on CT is the most important associated finding
- Appendicolith is neither pathognomonic nor reliably sensitive but increases risk of perforation
- Failure to fill with contrast or air on CT makes appendicitis highly likely
- Extraluminal gas or fluid, abscess, phlegmon = complicated appendicitis on CT
- Low-dose CT is non-inferior to standard dose in young adults - relevant for radiation-conscious practice
- CT performed very early (<12h) may be falsely negative - repeat at 24h is appropriate
Recent evidence note: A 2025 meta-analysis (PMID 40346255) and a 2026 systematic review (PMID 41106830) both confirm CT and MRI have superior sensitivity to ultrasound in children and adolescents, reinforcing the sequential US-then-CT/MRI approach. Point-of-care ultrasound sensitivity for paediatric appendicitis is moderately high but variable by operator.
Imaging finding of acute pancreatitis for postgraduate surgery
Imaging finding of acute pancreatitis for postgraduate surgery
Finding Sources
Finding Sources
Searching PubMed
"pancreatitis"[MeSH Terms] AND "diagnostic imaging"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full answer.
Imaging Findings of Acute Pancreatitis
Sources: Grainger & Allison's Diagnostic Radiology, Yamada's Textbook of Gastroenterology (7e), Harrison's Principles of Internal Medicine (22e), Sleisenger & Fordtran's Gastrointestinal & Liver Disease, Rosen's Emergency Medicine
Diagnostic Criteria for Acute Pancreatitis
Diagnosis requires two of three criteria:
- Typical epigastric pain radiating to the back
- Serum lipase or amylase ≥3× upper limit of normal
- Confirmatory imaging findings on contrast-enhanced CT, MRI, or ultrasound
Imaging is not required when the diagnosis is established by clinical and biochemical criteria alone. - Harrison's Principles of Internal Medicine 22e, p. 2789
1. Plain Abdominal Radiograph
Low yield for diagnosis but may show indirect signs:
| Sign | Significance |
|---|---|
| Sentinel loop | Localised ileus of proximal jejunum or duodenum adjacent to inflamed pancreas |
| Colon cut-off sign | Spasm of transverse colon at the splenic flexure from spread of inflammation |
| Obscured psoas shadow | Retroperitoneal fluid/inflammation |
| Pancreatic calcification | Suggests underlying chronic pancreatitis |
| Pleural effusion (left > right) | Reactive/sympathetic; correlates with severe disease |
Plain X-ray is useful mainly to exclude other causes (perforated viscus, bowel obstruction) in equivocal presentations.
2. Ultrasound
First-line modality - recommended as initial imaging in ALL patients.
Primary role: evaluate biliary aetiology (gallstones, CBD dilation) and assess for early complications.
Findings
| US Finding | Interpretation |
|---|---|
| Hypoechoic, heterogeneous, enlarged pancreas | Inflammation/oedema |
| Anechoic peripancreatic fluid | Acute peripancreatic fluid collection |
| Echoes within fluid collection | Suggests necrotic material |
| Gallstones in gallbladder | Biliary aetiology (sensitivity 67-87% in acute setting - reduced by overlying gas/pain-related guarding) |
| Dilated common bile duct | Biliary obstruction - can suggest choledocholithiasis |
| Pancreatic duct dilation | Variable; may suggest obstructive pancreatitis |
Limitations
- Sensitivity for pancreatitis itself is limited - bowel gas and ileus often obscure the pancreas
- Cannot visualise the distal body and tail reliably (retroperitoneal, gas overlay)
- Cannot reliably detect necrosis - this is a critical limitation
- Cannot visualise distal CBD stones reliably in acute setting
Contrast-enhanced ultrasound (CEUS): An alternative to CT when IV contrast is contraindicated (e.g. renal failure). CEUS can delineate necrotic areas (non-enhancing) and is recommended in EFSUMB guidelines for follow-up to reduce repeated CT exposure. - Grainger & Allison's Diagnostic Radiology, p. 681
3. Contrast-Enhanced Computed Tomography (CECT)
The gold standard imaging modality for staging and complications.
When to perform CT
CT is not indicated in all patients on admission:
- Mild pancreatitis with prompt clinical improvement: CT is not required
- CT performed in the first 24 hours may underestimate necrosis (which takes 2-3 days to develop fully)
- Optimal timing: 3-7 days after onset, when necrosis is fully demarcated
- Indications for urgent CT:
- Diagnostic uncertainty
- Failure to improve in 48-72h
- New/persisting organ failure
- Signs of sepsis
- Clinical deterioration
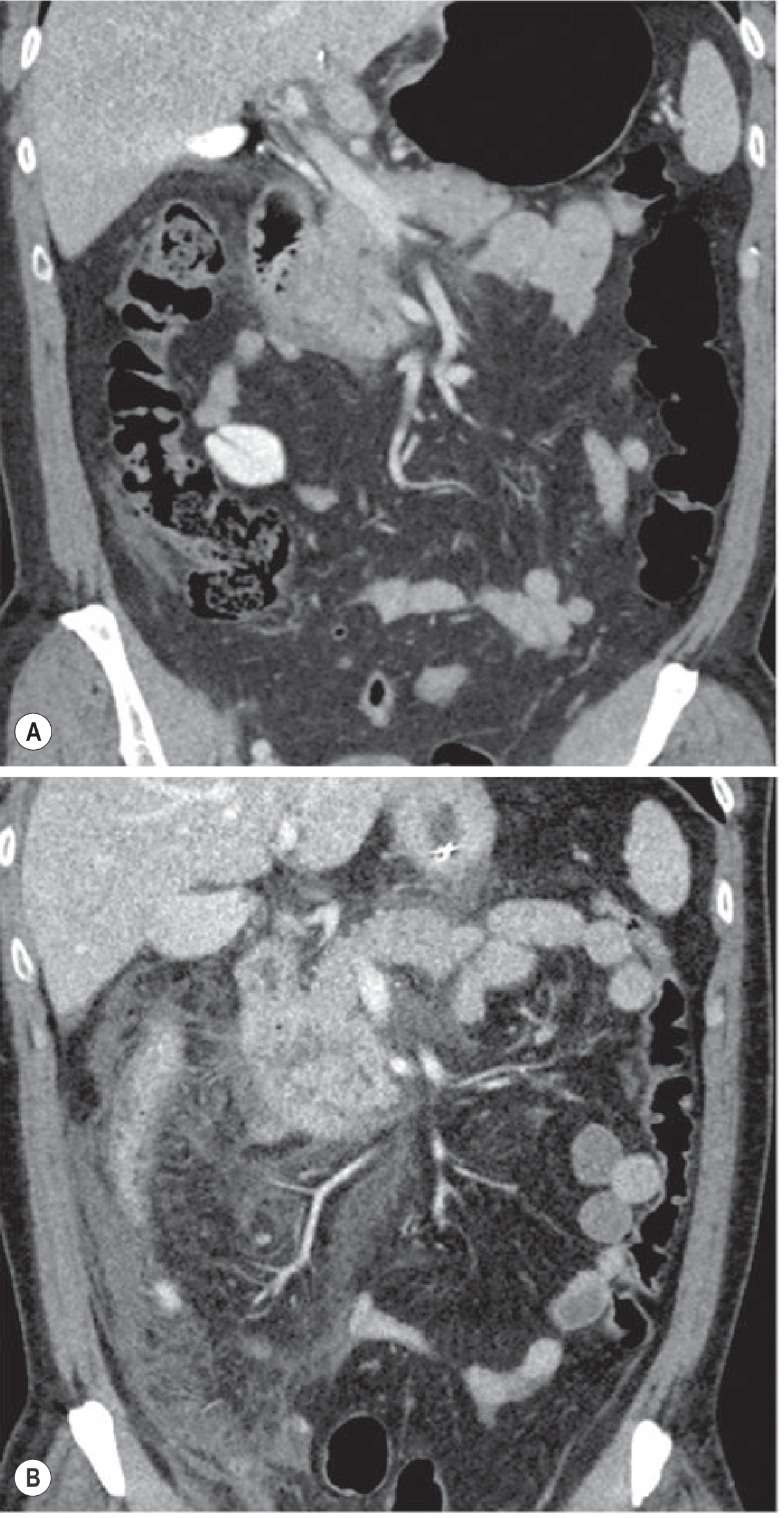
Figure: Appropriate timing of CT - (A) CT at 12h shows minimal pancreatitis; (B) same patient on day 3 shows severe inflammation with fluid collections (Grainger & Allison, p. 681)
CT Protocol
- IV contrast is mandatory - single portal venous phase at 70s (1.5-2 mL/kg at 4 mL/s)
- Arterial phase is not routinely needed unless vascular complication suspected
- Unenhanced images not required routinely
- Radiation dose minimisation is important (young patients may need multiple studies)
CT Findings - Interstitial Oedematous Pancreatitis (IEP)
IEP constitutes 70-80% of all acute pancreatitis cases.
| CT Finding | Description |
|---|---|
| Pancreatic enlargement | Diffuse or focal; loss of normal lobulated contour |
| Normal or near-normal parenchymal enhancement | Uniform IV contrast uptake (distinguishes IEP from NP) |
| Peripancreatic fat stranding | "Mistiness" or streaky high-attenuation in peripancreatic fat |
| Acute Peripancreatic Fluid Collection (APFC) | Homogeneous fluid density, no wall, confined by fascial planes, immediately adjacent to pancreas; no solid material |
| Thickening of Gerota's fascia | Anterior pararenal space fluid tracking |
| Fluid in omental bursa / lesser sac | Common in pancreatic body/tail inflammation |
| Mild gland heterogeneity | Difficult to differentiate from early necrosis - follow-up CT resolves uncertainty |
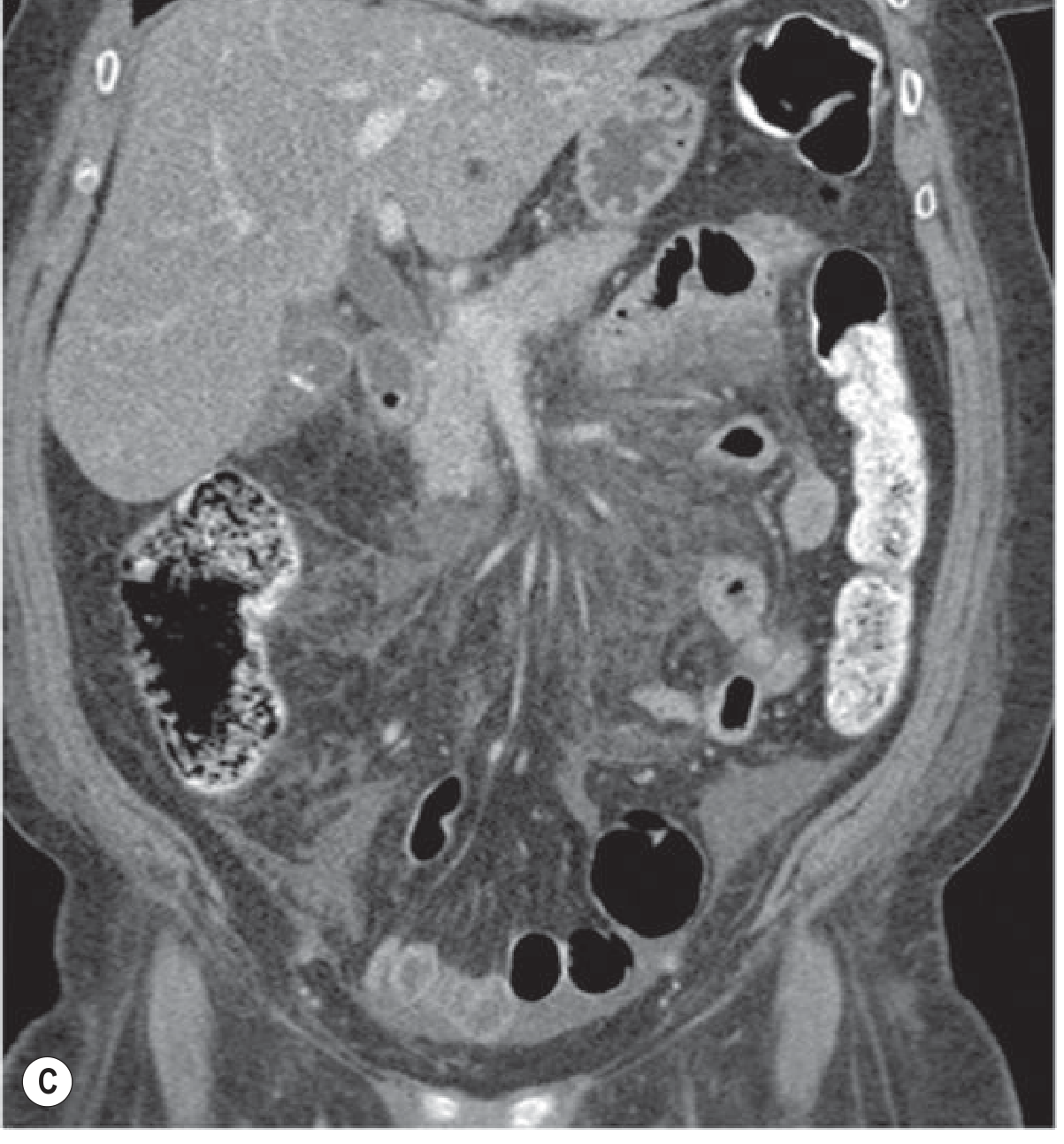
Figure: CT of acute interstitial oedematous pancreatitis - severe form with fluid in paracolic gutter and pelvis (Grainger & Allison, p. 682)
CT Findings - Necrotising Pancreatitis (NP)
The single most important CT finding in acute pancreatitis is detection of necrosis, which determines morbidity, mortality, and management. Necrosis develops in 20-30% of patients.
| CT Finding | Description |
|---|---|
| Focal or diffuse non-enhancement of parenchyma | Defining criterion for necrosis - areas that fail to enhance after IV contrast |
| Liquefaction or severe hypoenhancement | Progressive necrosis of glandular tissue |
| Heterogeneous, phlegmonous retroperitoneum | Severe peri-glandular inflammatory change accompanies significant necrosis |
| Extrapancreatic fat necrosis | "Mass-like" fat-density collections (denser than simple oedema/stranding) |
| Acute Necrotic Collection (ANC) | Heterogeneous collection (fluid + solid necrotic debris); no wall; intra- and/or extrapancreatic |
Three forms of NP (Revised Atlanta):
- Pancreatic + peripancreatic necrosis - most common (75-80%)
- Peripancreatic fat necrosis alone - better prognosis than parenchymal necrosis
- Pancreatic parenchymal necrosis alone - rarest (5%)
Two CT features that correlate with mortality:
- Necrosis of more than one anatomical segment (head, body, or tail)
- Distant fluid collections (posterior pararenal space, paracolic gutter)
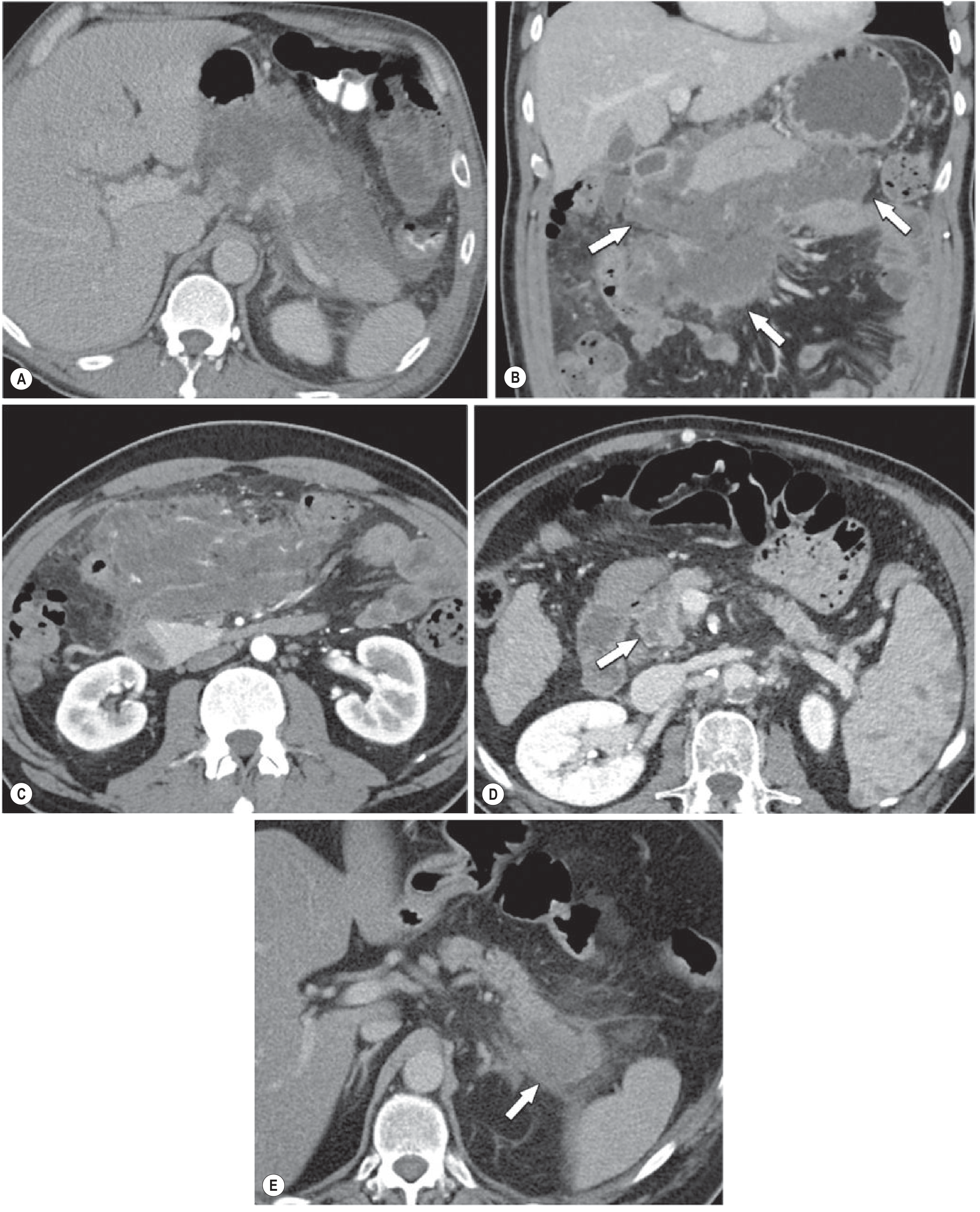
Figure: Different morphological types of necrotising pancreatitis on CT (Grainger & Allison, p. 685)
4. CT Severity Scoring Systems
A. Balthazar Grading (Original - 1985)
Grades based on CT appearance of the pancreas and fluid collections:
| Grade | CT Findings | Points |
|---|---|---|
| A | Normal pancreas | 0 |
| B | Focal or diffuse enlargement; contour irregularities; no peripancreatic inflammation | 1 |
| C | Grade B + peripancreatic inflammation | 2 |
| D | Grade C + single associated fluid collection | 3 |
| E | Grade C + 2 or more fluid collections, or gas in pancreas/retroperitoneum | 4 |
Prognostic correlation: 5/37 patients (13.5%) with Grade D or E died vs. none of 51 patients with Grades B or C. - Sleisenger & Fordtran, p. 2489
B. CT Severity Index (CTSI) - Balthazar + Necrosis Score
CTSI = Balthazar Grade Points + Necrosis Points
| Degree of Necrosis | Points |
|---|---|
| None | 0 |
| Up to 33% | 2 |
| 33-50% | 4 |
| >50% | 6 |
Total CTSI score: 0-10
- Local complications developed in 54% of Grade D/E patients vs. 3.9% of Grades A-C
C. Modified CTSI (MCTSI) - Current Preferred
Based on Revised Atlanta Classification - simplified but better outcome correlation:
| Prognostic Indicator | Points |
|---|---|
| Pancreatic inflammation | |
| Normal pancreas | 0 |
| Intrinsic pancreatic abnormalities ± peripancreatic fat changes | 2 |
| Pancreatic/peripancreatic fluid or fat necrosis | 4 |
| Pancreatic necrosis | |
| None | 0 |
| ≤30% | 2 |
| >30% | 4 |
| Extrapancreatic complications (pleural effusion, ascites, vascular/parenchymal/GI complications) | 2 |
Severity classification:
- Mild: 0-2 points
- Moderate: 4-6 points
- Severe: 8-10 points
- Organ failure incidence: 6% (mild), 9% (moderate), 50% (severe) - Grainger & Allison, p. 681
5. Revised Atlanta Classification - CT Morphological Definitions
The 2012 Revised Atlanta Classification is the current international standard for reporting CT findings in acute pancreatitis:
| Entity | CT Features | Timing |
|---|---|---|
| Interstitial pancreatitis | Normal parenchymal enhancement; no peripancreatic necrosis | Early |
| Necrotising pancreatitis | Lack of parenchymal enhancement; and/or peripancreatic necrosis | Early |
| APFC (Acute Peripancreatic Fluid Collection) | Homogeneous fluid density; no wall; no solid component; confined by fascial planes; adjacent to pancreas | <4 weeks after IEP |
| Pancreatic pseudocyst | Well-circumscribed; round/oval; homogeneous fluid density; no solid component; well-defined wall (completely encapsulated); matures >4 weeks after IEP | >4 weeks |
| ANC (Acute Necrotic Collection) | Heterogeneous; liquid + solid density; no definitive wall; intra- and/or extrapancreatic | <4 weeks after NP |
| WON (Walled-Off Necrosis) | Heterogeneous (liquid + solid); well-defined encapsulating wall; intra- and/or extrapancreatic | >4 weeks after NP |
Key distinction for management: Liquid-only collections (APFC, pseudocyst) can be drained; non-liquid collections (ANC, WON) require endoscopic/surgical necrosectomy for the solid component. - Harrison's 22e, p. 2789
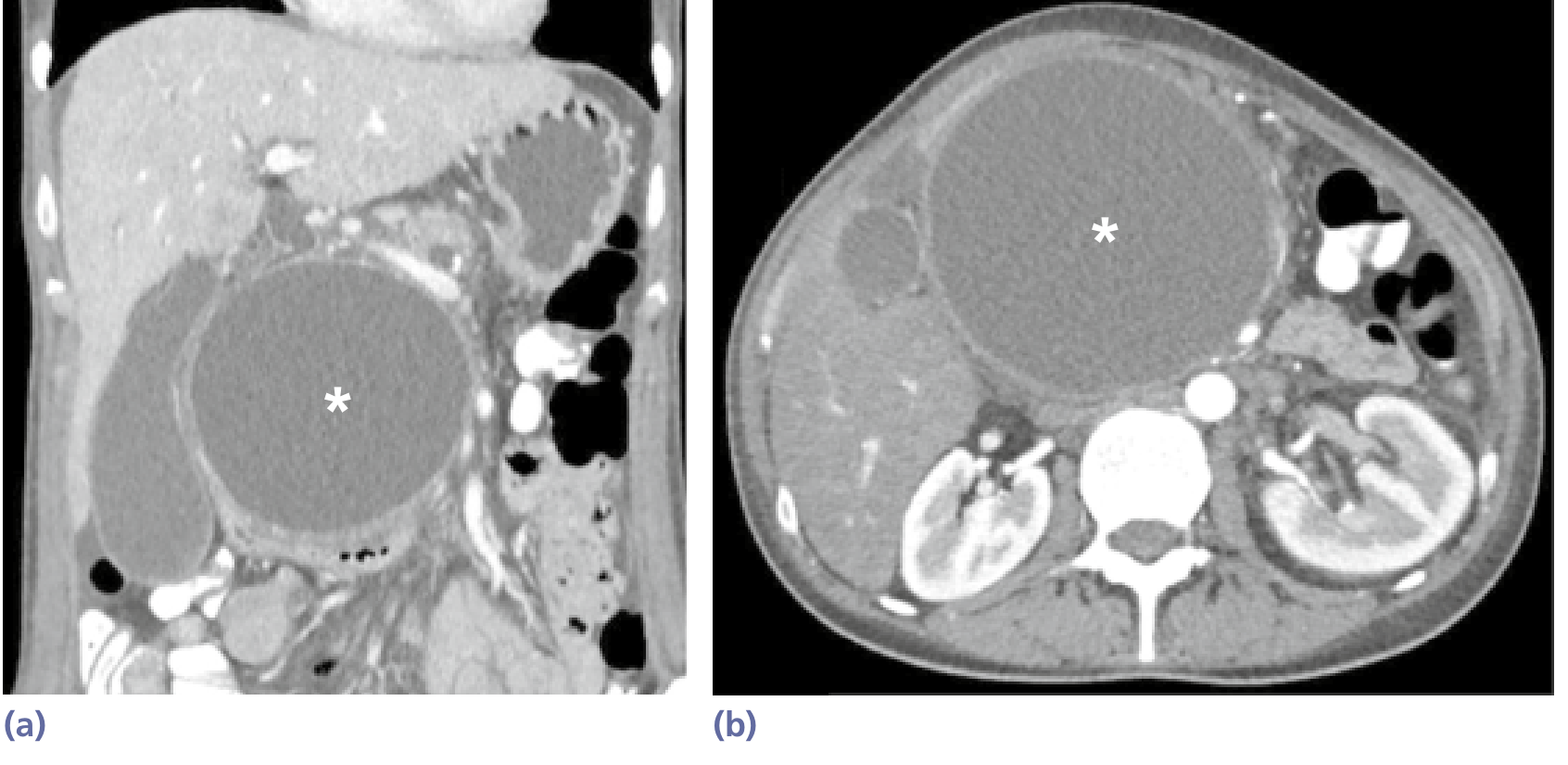
Figure: Pancreatic pseudocyst () - well-defined capsule, homogeneous fluid, no solid debris. Coronal (a) and axial (b) reconstruction 6 weeks after acute pancreatitis (Yamada's Gastroenterology, p. 1641)*
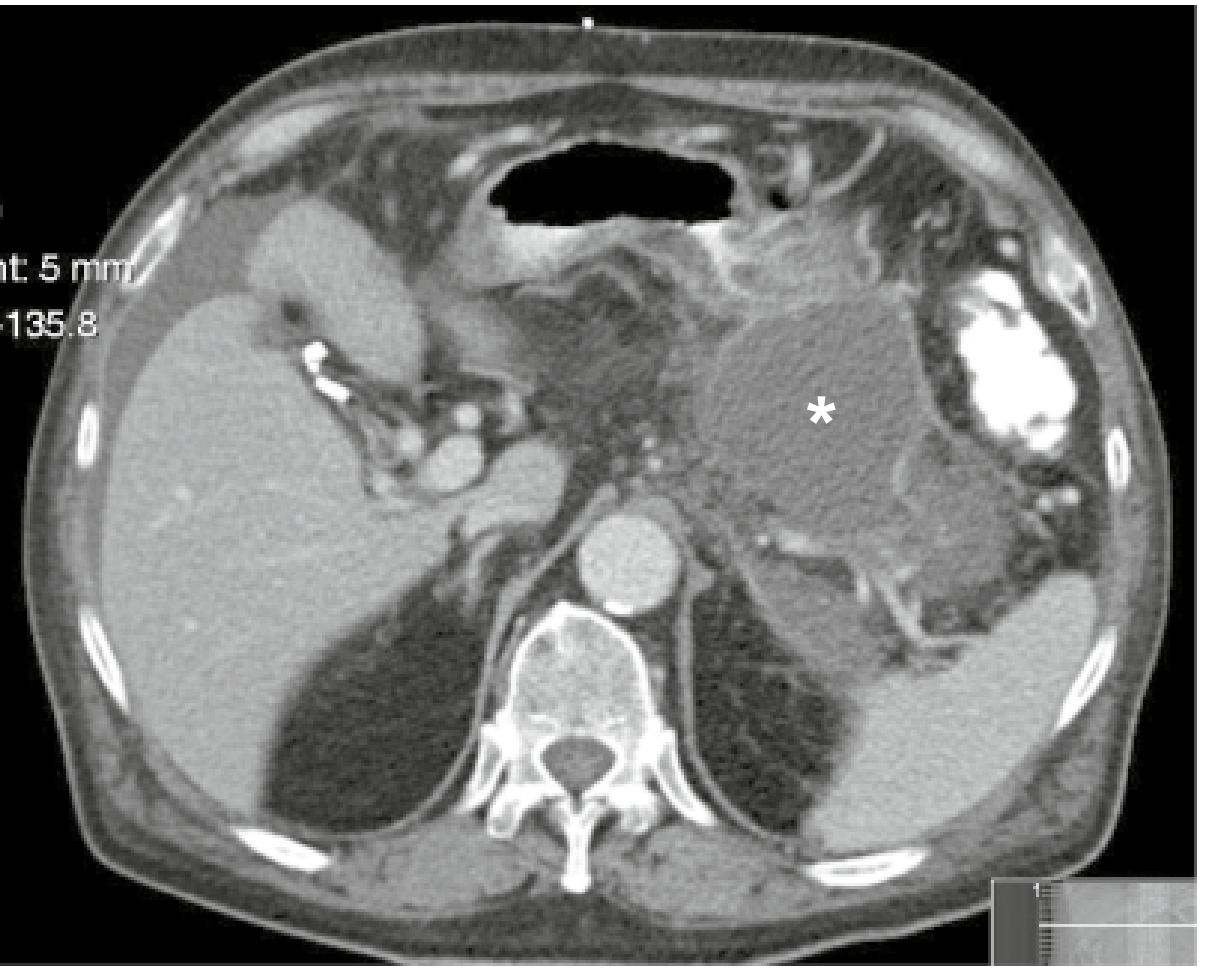
Figure: CT of walled-off necrosis () at 5 weeks - heterogeneous content distinguishes it from a pseudocyst (Yamada's Gastroenterology, p. 1642)*
6. MRI and MRCP
MRI
- Excellent alternative to CT when IV contrast is contraindicated (renal failure) or to reduce radiation in young patients
- Superior to CT for: detecting solid debris within collections (distinguishing pseudocyst from WON), detecting pancreatic ductal disruption, and identifying haemorrhage
- T2-weighted sequences: pancreatic oedema appears hyperintense; necrosis is heterogeneous with low T2 areas
- Gadolinium-enhanced sequences: necrosis appears as non-enhancing zones (same principle as CT)
- DWI (diffusion-weighted imaging): restricted diffusion in gangrenous/infected areas
MRCP (Magnetic Resonance Cholangiopancreatography)
- Gold standard non-invasive test for biliary pancreatitis - identifies CBD stones, ductal disruption
- Sensitivity and negative predictive value of 100% for ruling out CBD stones in resolving gallstone pancreatitis - patients with negative MRCP do not need preoperative ERCP - Grainger & Allison, p. 681
- Identifies disconnected pancreatic duct syndrome (duct disruption in necrotising pancreatitis)
- Avoids risks of ERCP (post-ERCP pancreatitis)
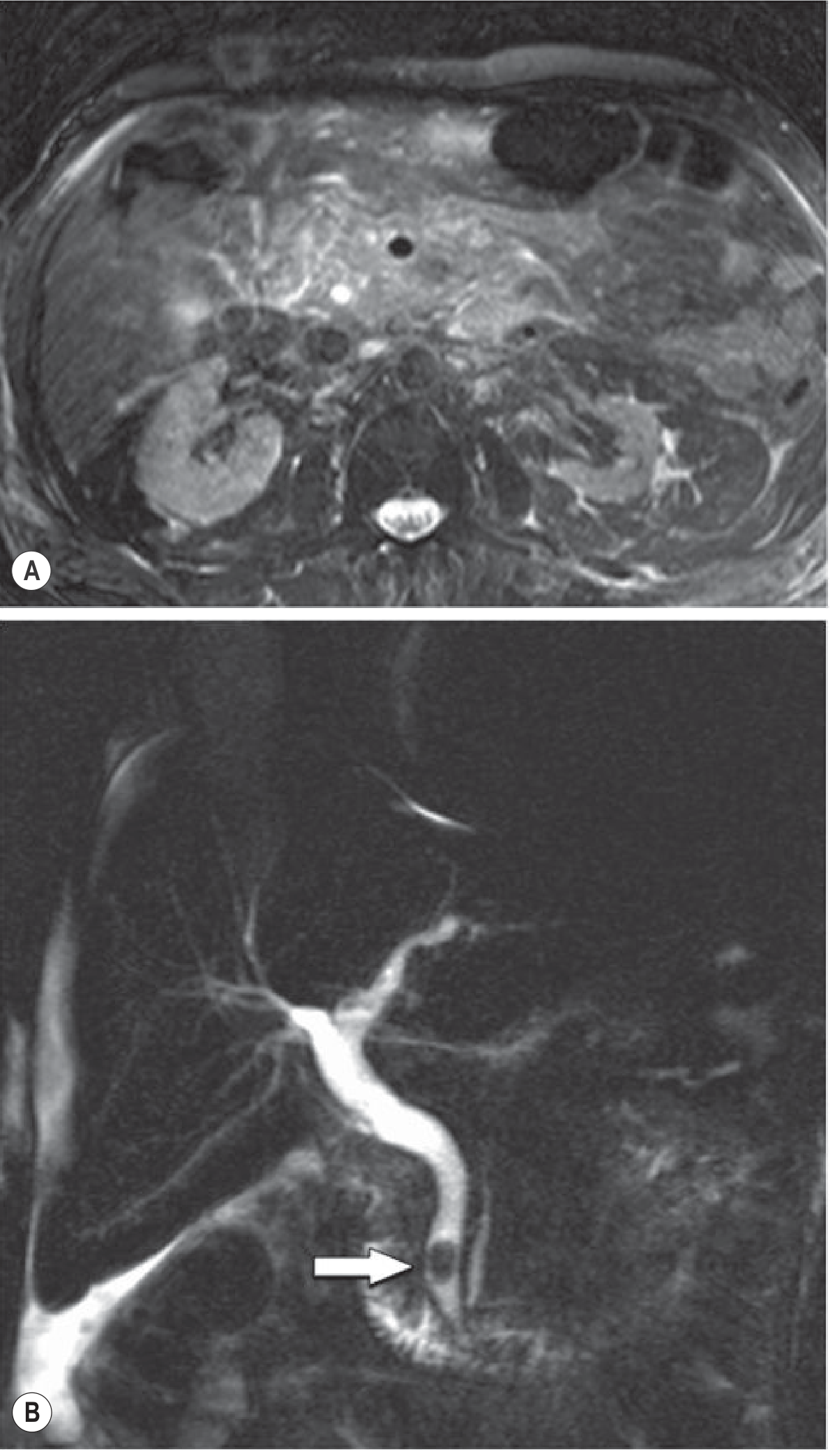
Figure: MRCP in biliary pancreatitis - (A) severe pancreatic oedema on T2; (B) large distal CBD stone (arrow) (Grainger & Allison, p. 682)
7. Imaging of Complications
Local Complications
| Complication | CT/Imaging Features |
|---|---|
| Infected necrosis | Gas bubbles within ANC or WON on CT (highly specific - "mottled gas pattern"); thick-walled; clinical correlation essential |
| Pancreatic abscess | Thick-walled fluid collection (from infected pseudocyst); gas bubbles; occurs in ~3% of severe pancreatitis |
| Pseudoaneurysm | Enhancing arterial structure within or adjacent to pancreatic collection on CECT; splenic artery and gastroduodenal artery most common; confirmed by CT angiography |
| Splenic/portal vein thrombosis | Non-enhancing vein; most common: splenic vein → sinistral (left-sided) portal hypertension |
| Splenic infarction/haemorrhage | Hypoenhancing wedge in spleen; haemoperitoneum |
| Bowel involvement | Wall thickening, oedema of duodenum/transverse colon; necrosis/perforation in severe cases |
| Biliary obstruction | CBD dilation on CT/US; requires MRCP or EUS for stone detection |
Infected necrosis occurs in 20-70% of patients with pancreatic necrosis and is responsible for an estimated 80% of deaths from acute pancreatitis. - Grainger & Allison, p. 683
Systemic Complications on Imaging
| Finding | Modality |
|---|---|
| Left-sided pleural effusion | CXR/CT - correlates with severity; within 72h predicts severe disease |
| Pulmonary infiltrates/ARDS | CXR - bilateral diffuse infiltrates |
| Ascites | US/CT - free peritoneal fluid |
| Pericardial effusion | Rare; CT/echo |
8. Imaging Algorithm for Clinical Practice
Suspected Acute Pancreatitis
↓
Step 1: Establish diagnosis
→ Abdominal US (all patients, on admission)
- Confirms gallstones/biliary aetiology
- Detects early fluid collections
- LIMITED for pancreatic assessment
↓
Step 2: Clinical assessment 48-72h
→ Mild, improving: NO CT required
→ Equivocal, non-improving, deteriorating:
CECT at 72h-7 days (optimal timing)
↓
Step 3: Complications / Etiology workup
→ Biliary aetiology uncertain: MRCP (or EUS)
→ Suspected infection in necrosis: CECT ± CT-guided FNA
→ Suspected vascular complication: CT angiography
→ Ductal disruption / WON: MRI/MRCP
→ Renal failure (contrast-contraindicated): CEUS or MRI
9. Key Points for Postgraduate Surgery Examination
- Ultrasound first in all patients - primarily to detect biliary aetiology, not to diagnose pancreatitis
- CT is NOT needed on admission in mild, resolving pancreatitis - clinical + biochemical diagnosis suffices
- Optimal CT timing is 3-7 days - necrosis takes 48-72h to fully develop; early CT underestimates severity
- IV contrast is mandatory for CT - without it, necrosis cannot be assessed
- Necrosis = non-enhancing parenchyma on CECT - the critical finding that determines severity
- Balthazar grading A-E + necrosis score = CTSI (0-10) - correlates with local complications better than mortality
- Revised Atlanta 2012 defines 6 morphological entities: IEP, NP, APFC, pseudocyst, ANC, WON
- Key distinction: APFC → pseudocyst (>4wks, IEP); ANC → WON (>4wks, NP)
- WON vs pseudocyst: Both have a wall at >4 weeks, but WON is heterogeneous (solid debris) - MRI/EUS distinguishes them better than CT
- Gas in a collection = infected WON/ANC until proved otherwise
- MRCP NPV of 100% for CBD stones in resolving biliary pancreatitis - negative MRCP avoids ERCP
- Pseudoaneurysm: Splenic artery > gastroduodenal artery; 2-5% incidence; managed by angioembolisation
- Splenic vein thrombosis → sinistral portal hypertension → gastric varices
- Infected necrosis accounts for 80% of deaths from acute pancreatitis
Recent guideline note: The 2026 Ibero-Latin American Guidelines on Acute Pancreatitis (PMID 42216617) reinforce the Revised Atlanta Classification and confirm CECT as the standard for staging, with MRCP recommended for biliary aetiology evaluation.
Ct image of necrotizing pancreatitis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Here are all the CT images of necrotising pancreatitis from authoritative surgical and radiology textbooks, with annotations explaining the key findings:
CT Images of Necrotising Pancreatitis
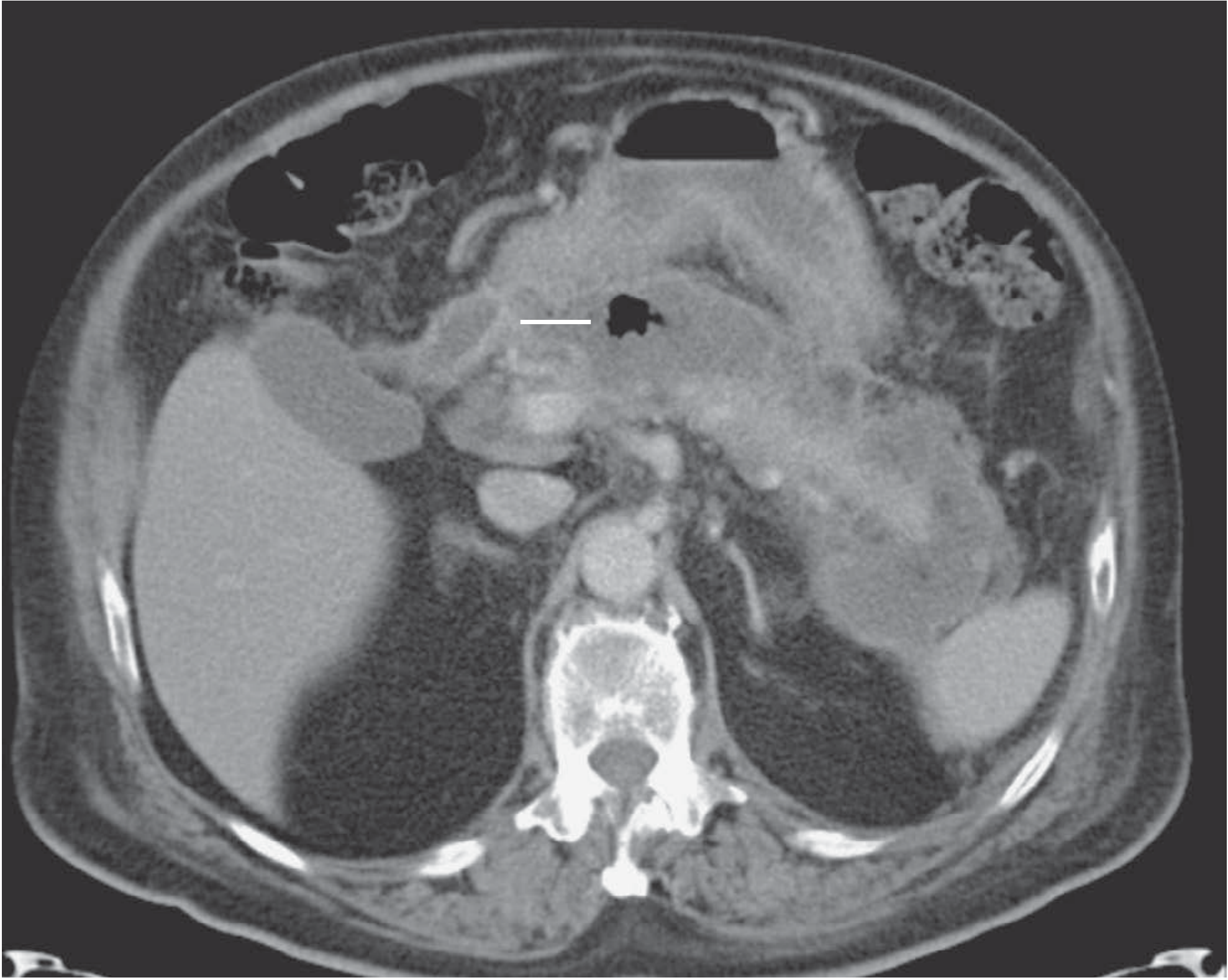
Image 1 - Acute Necrotising Pancreatitis (Classic Axial CECT)
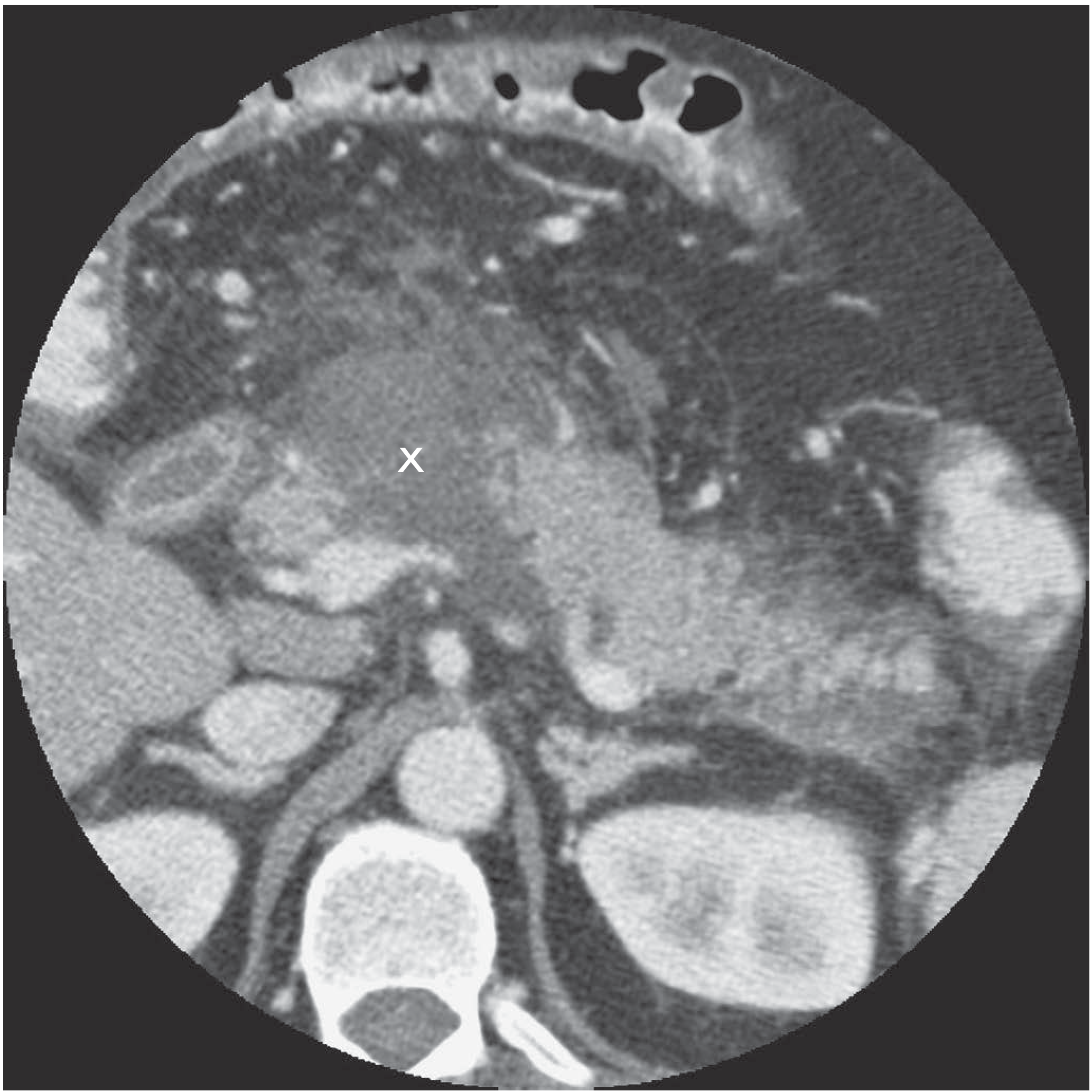
What you are seeing: The marker X points to a large area of reduced/absent parenchymal enhancement in the pancreatic body and tail. The normal pancreas enhances brightly with IV contrast; the non-enhancing zone represents ischaemic/necrotic parenchyma. The surrounding tissue shows fat stranding and peripancreatic oedema.
Bailey & Love's Short Practice of Surgery, 28th Ed., Fig. 72.22 (courtesy Dr. Niall Power)
Image 2 - Infected Pancreatic Necrosis with Gas
What you are seeing: Non-enhancing necrotic pancreatic parenchyma surrounded by a large peripancreatic fluid/necrotic collection. The arrow points to gas bubbles (dark foci) within the collection - this is highly specific for infected necrosis. This patient was managed with percutaneous drainage and antibiotics.
Bailey & Love's Short Practice of Surgery, 28th Ed., Fig. 72.24
Image 3 - ANC Evolving into Walled-Off Necrosis (WON)
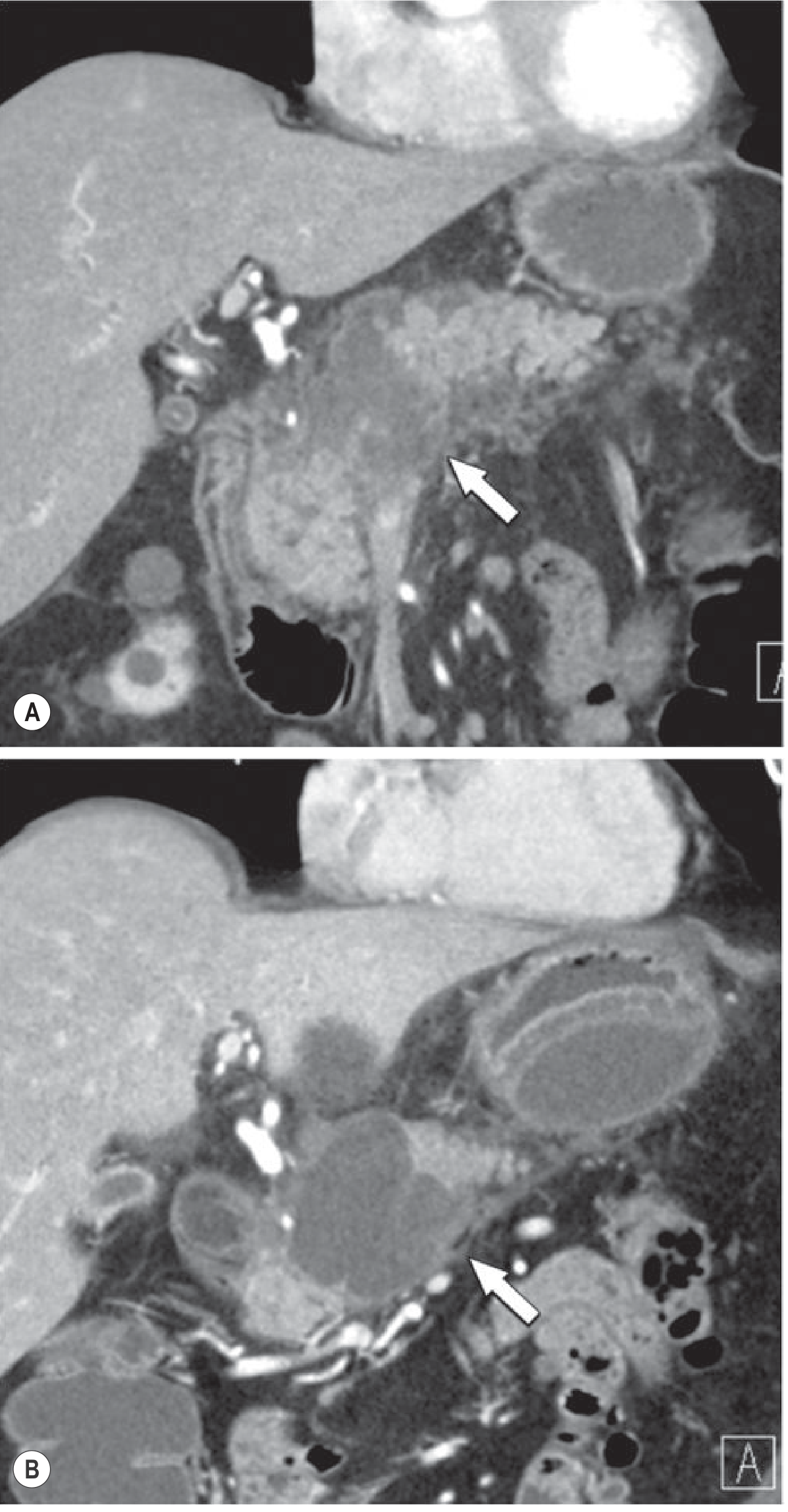
What you are seeing:
- (A - top): Early acute necrotic collection (ANC) in pancreatic head and body (arrow). The collection has no definable wall and contains heterogeneous necrotic material.
- (B - bottom): Follow-up CT at 4 weeks - the same collection has now developed a thick encapsulating wall = Walled-Off Necrosis (WON). The content remains heterogeneous with debris of fat attenuation.
This demonstrates the time-dependent evolution: ANC → WON (>4 weeks)
Grainger & Allison's Diagnostic Radiology, Fig. 25.15
Image 4 - Extensive Necrotising Pancreatitis (Severe Form - Panel B)
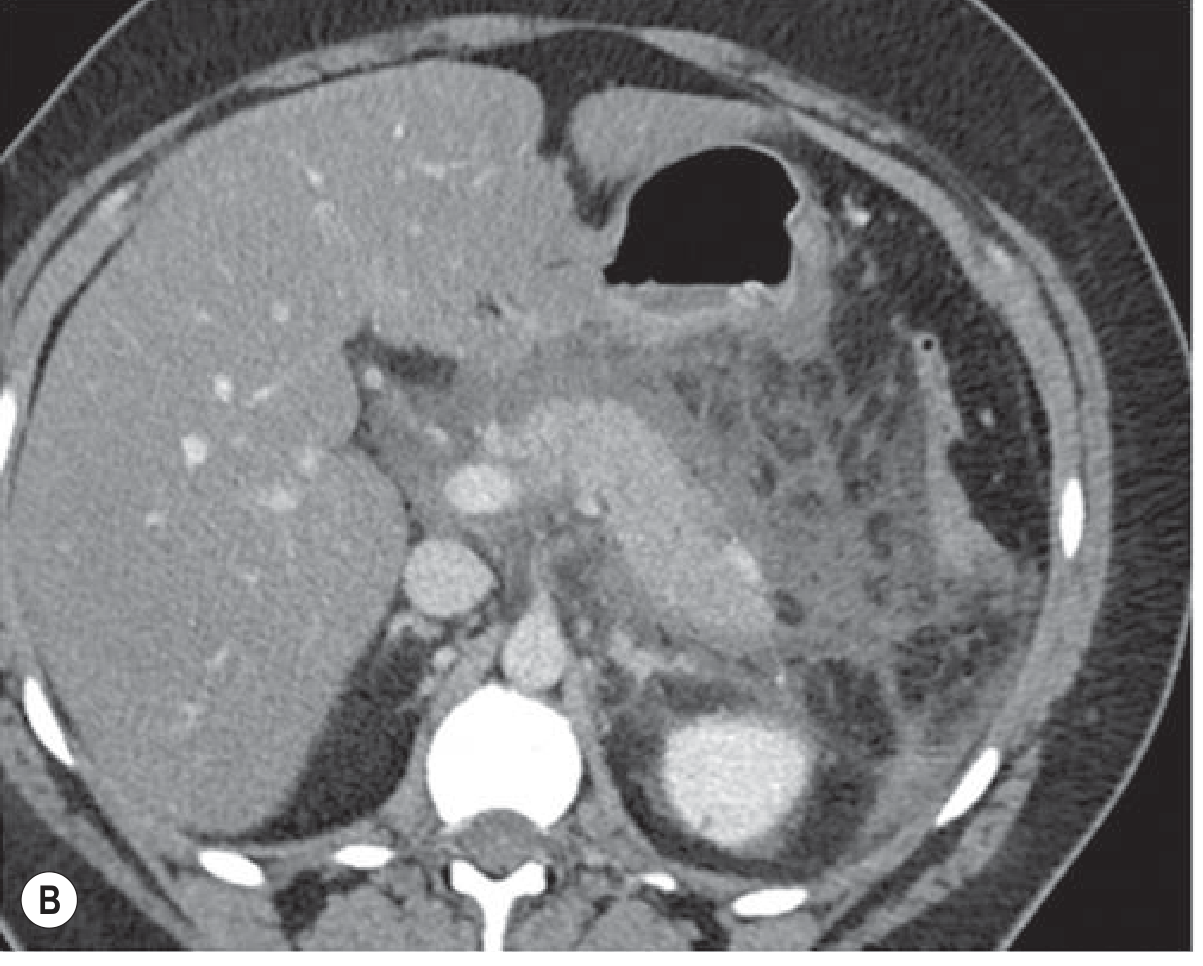
What you are seeing: Severe necrotising pancreatitis on axial CECT. The pancreatic parenchyma is almost completely non-enhancing (heterogeneous low attenuation throughout). Massive inflammatory reaction occupies the entire retroperitoneum and peripancreatic space. The hepatic parenchyma (top right) enhances normally, highlighting the contrast between viable and necrotic tissue.
Grainger & Allison's Diagnostic Radiology, Fig. 25.11B (severe form)
Image 5 - Different Morphological Types of Necrotising Pancreatitis
What you are seeing (Revised Atlanta Classification forms):
- (A): Combined intra- + extrapancreatic necrosis - most common type (75-80%); non-enhancing pancreatic parenchyma with adjacent fat necrosis
- (B & C): Extrapancreatic fat necrosis alone (arrows) - mass-like, dense fat collections distinguishable from simple oedematous stranding. Better prognosis than parenchymal necrosis
- (D): Intrapancreatic necrosis alone (arrow) - hypoenhancing focal zone without significant peripancreatic change
- (E): Tail necrosis alone (arrow) - localised non-enhancement confined to the pancreatic tail with minimal surrounding oedema
Grainger & Allison's Diagnostic Radiology, Fig. 25.14
Summary: Key CT Criteria for Necrotising Pancreatitis
| CT Finding | Significance |
|---|---|
| Focal or diffuse non-enhancement after IV contrast | Defines necrosis - the single most important finding |
| Heterogeneous parenchyma | Mixture of viable and necrotic tissue |
| Peripancreatic fat necrosis (mass-like dense fat collections) | Extrapancreatic necrosis - fulfils NP criteria even without parenchymal necrosis |
| ANC (no wall, heterogeneous, intra-/extrapancreatic) | Early necrotic collection <4 weeks |
| WON (well-defined encapsulating wall, heterogeneous content) | Matured ANC at >4 weeks |
| Gas bubbles within collection | Infected necrosis - high specificity; indicates need for drainage |
| Necrosis >30% on CTSI | High-risk feature; CTSI score ≥6 indicates severe disease |
Critical point: IV contrast is mandatory on CT to identify necrosis. Non-contrast CT cannot distinguish viable from non-viable pancreatic parenchyma.
This is a shared conversation. Sign in to Orris to start your own chat.