Inguinal canal anatomy. Inguinal hernia. Surgical treatment of hernia
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Searching PubMed
"inguinal hernia"[MeSH Terms] AND "herniorrhaphy"[MeSH Terms]
I now have all the material needed for a comprehensive answer. Let me compile it.
Inguinal Canal Anatomy, Inguinal Hernia, and Surgical Treatment
Sources: Bailey and Love's Short Practice of Surgery, 28th Ed.; Schwartz's Principles of Surgery, 11th Ed.; Fischer's Mastery of Surgery, 8th Ed.
1. Anatomy of the Inguinal Canal
The inguinal canal is an oblique passage through the lower abdominal wall, approximately 4 cm long, running downward and medially from the deep (internal) inguinal ring to the superficial (external) inguinal ring.
Boundaries
| Wall | Structure |
|---|---|
| Anterior | Aponeurosis of external oblique muscle |
| Posterior | Transversalis fascia (reinforced medially by conjoint tendon) |
| Roof | Arching fibres of internal oblique and transversus abdominis - forming the conjoint tendon |
| Floor | Inguinal (Poupart's) ligament - the thickened, inrolled inferior edge of the external oblique aponeurosis |
Rings
- Deep inguinal ring: A defect in the transversalis fascia, located midway between the anterior superior iliac spine (ASIS) and the pubic tubercle, approximately 2-3 cm above the femoral artery pulse. The inferior epigastric vessels run just medial to this ring - this landmark is critical for distinguishing direct from indirect hernias.
- Superficial inguinal ring: An inverted V-shaped defect in the external oblique aponeurosis, just above and medial to the pubic tubercle.
Contents
In males: testicular artery, pampiniform venous plexus, lymphatics, vas deferens, and cremasteric muscle fibres.
In females: the round ligament descends through the canal to the labia majora.
Three nerves pass through or near the canal in both sexes:
- Ilioinguinal nerve
- Iliohypogastric nerve
- Genital branch of the genitofemoral nerve

Figure: Close relationships of direct inguinal, indirect inguinal, and femoral hernias (Bailey & Love)
Developmental Background
As the testis descends from the retroperitoneum into the scrotum, it passes through the transversalis fascia at the deep ring, dragging a tube of peritoneum - the processus vaginalis - which normally obliterates before birth. The testicular vessels, vas deferens, and their coverings form the spermatic cord within the canal. Failure of the processus to obliterate is the anatomical basis of congenital indirect inguinal hernia.
The posterior wall has an inherent weakness below the conjoint tendon arch (between the deep ring and pubic tubercle) where only transversalis fascia and external oblique aponeurosis are present - this corresponds to Hesselbach's triangle and is the site of direct hernias.
2. Inguinal Hernia
Inguinal hernia is the most common hernia in both sexes, and is approximately 10 times more common in men. There are two fundamentally different types.
2a. Indirect (Lateral/Oblique) Inguinal Hernia
- Enters the canal through the deep inguinal ring, lateral to the inferior epigastric vessels
- Follows the oblique path of the processus vaginalis through the canal
- Can pass all the way to the scrotum
- May be congenital (patent processus vaginalis) or acquired
- All congenital hernias in children are indirect by definition
2b. Direct (Medial) Inguinal Hernia
- Protrudes through the posterior wall of the canal in Hesselbach's triangle, medial to the inferior epigastric vessels
- Always acquired - results from stretching and weakening of the abdominal wall
- Broadly based, therefore less likely to strangulate
- More common in elderly patients
- The bladder may be drawn into a direct hernia sac
Hesselbach's triangle boundaries:
- Lateral: inferior epigastric vessels
- Medial: lateral edge of rectus abdominis
- Inferior: inguinal ligament (iliopubic tract)
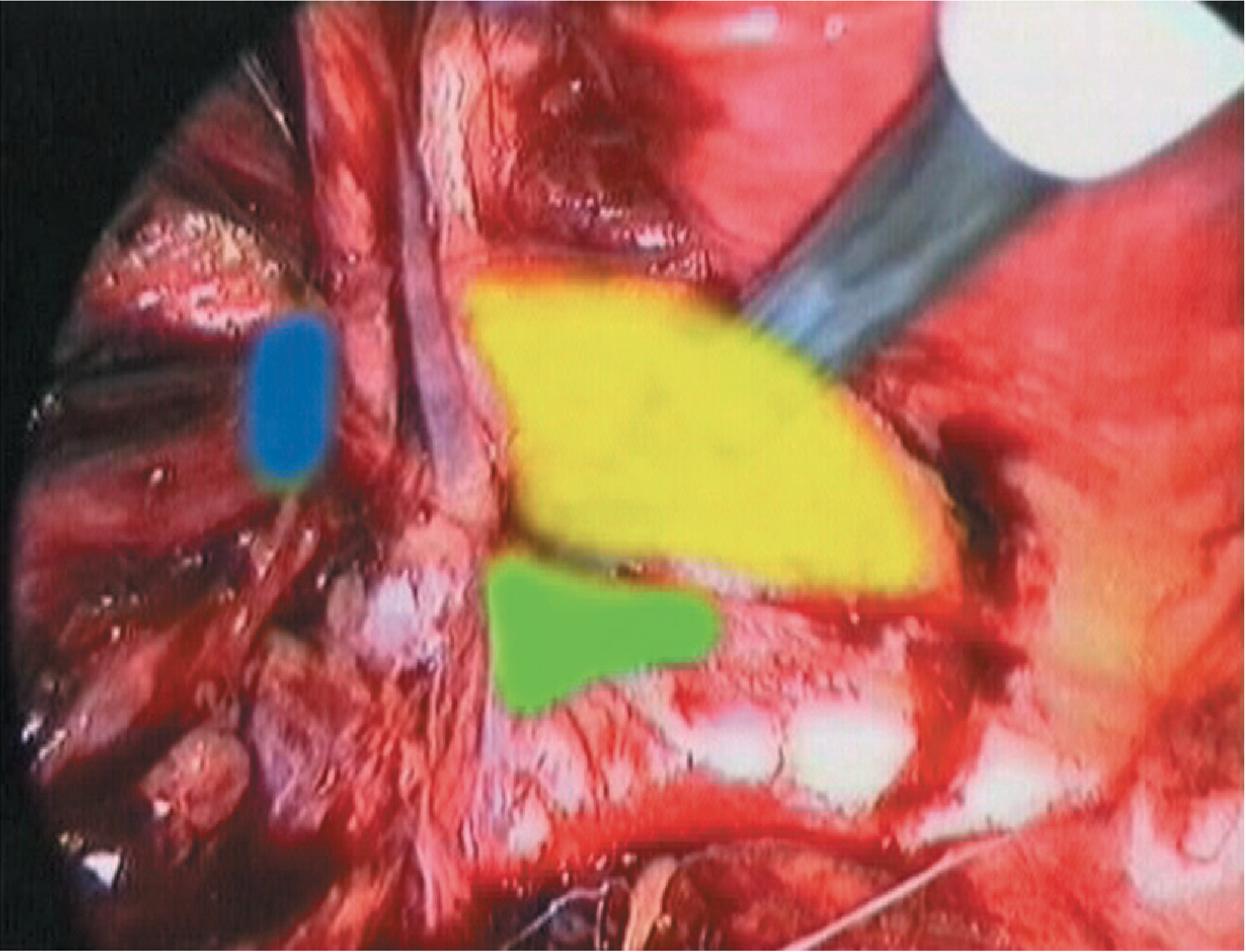
Figure: Laparoscopic view highlighting hernia defects - yellow (direct/Hesselbach's), blue (indirect/lateral), green (femoral) (Bailey & Love)
2c. Sliding Hernia
An acquired indirect hernia where retroperitoneal fatty tissue is pushed down the canal. As more tissue enters, peritoneum is dragged secondarily to form a sac. Sigmoid colon may slide in on the left; caecum on the right. The bowel wall forms part of the sac itself - surgeons must exercise caution to avoid bowel injury during dissection.
2d. "Pantaloon" Hernia
Both an indirect and direct hernia are present simultaneously on the same side, straddling the inferior epigastric vessels. Uncommon.
Classification (European Hernia Society)
- P = primary / R = recurrent
- L = lateral (indirect), M = medial (direct), F = femoral
- Defect size in fingerbreadths: 1 = ≤1 cm, 2 = 1-3 cm, 3 = ≥3 cm
Example: a primary indirect hernia with a 3-cm defect = PL2
2e. Complications
- Reducible - contents pass freely back into the abdomen
- Irreducible (incarcerated) - contents cannot be returned; risk of obstruction
- Strangulated - blood supply to the contents is compromised; emergency surgery required
- Direct hernias rarely strangulate (broad neck); indirect hernias at the narrow deep ring are much more prone
Diagnosis
Clinical in most cases. The patient is examined standing and asked to cough:
- Pressure applied at the deep inguinal ring (midpoint of inguinal ligament): if this controls the hernia on coughing = indirect; if it appears medial to this pressure point = direct
- Even experienced surgeons cannot always distinguish the two types with certainty preoperatively
Imaging (ultrasound, CT, MRI) is used for diagnostic uncertainty - but hernias may reduce spontaneously in supine patients, so scans can miss them.
3. Surgical Treatment
Surgery is indicated for symptomatic hernias, all hernias in children, and for incarcerated/strangulated hernias (emergency). Asymptomatic small direct hernias in elderly patients may be managed conservatively - surgical trusses are not recommended.
Operations - Summary (Bailey & Love Summary Box 64.9)
| Category | Operation |
|---|---|
| Herniotomy only | Children (sac excision and closure) |
| Open suture repair | Bassini, Shouldice, Desarda, Maloney darn |
| Open flat mesh repair | Lichtenstein (tension-free) |
| Open complex mesh | Mesh plug, hernia systems (not routinely recommended) |
| Open preperitoneal | Stoppa repair |
| Laparoscopic | TEP (totally extraperitoneal), TAPP (transabdominal preperitoneal) |
| Robotic-assisted | TAPP/TEP variant |
3a. Herniotomy (Children)
In children with a lateral hernia and patent processus vaginalis, it is sufficient to excise and close the sac only - no floor repair needed. In adults, herniotomy alone has a high recurrence rate and must be combined with a herniorrhaphy.
3b. Open Suture Repair (Bassini / Shouldice)
Bassini (1890): The landmark operation - opened the external oblique, dissected the spermatic cord, dealt with the sac, then placed sutures between the conjoint tendon superiorly and the inguinal ligament inferiorly from pubic tubercle to deep ring. Strengthens the posterior wall. Was the standard for over 100 years but has largely been replaced by mesh repairs due to tension-related recurrence and pain.
Shouldice repair: Four-layer imbrication of the posterior wall using continuous sutures. Excellent long-term results, particularly at dedicated hernia centres; recurrence rates around 1% in expert hands.
Desarda / Maloney darn: Use strips of external oblique aponeurosis or suture-darned repair respectively. Considered equivalent to Shouldice in current guidelines.
3c. Open Flat Mesh Repair - Lichtenstein
The most common operation for inguinal hernia in resource-rich countries. Described in the 1980s.
Steps:
- Open the external oblique aponeurosis - enter the canal
- Dissect the spermatic cord free
- Identify and deal with the hernia sac (excise lateral sac, invert medial sac)
- Place an 8 × 15 cm polypropylene mesh flat over the posterior wall, behind the cord
- The mesh is slit to wrap around the cord at the deep ring
- Fixed with loose sutures to the inguinal ligament inferiorly and the conjoint tendon superiorly
Key advantage: tension-free repair - removes the main driver of recurrence. Randomised trials show lower recurrence than suture repair at 2 years. However, chronic pain is the most significant complication, reported in up to 20% of patients, mainly due to mesh-nerve interaction (ilioinguinal, iliohypogastric, genitofemoral nerves).
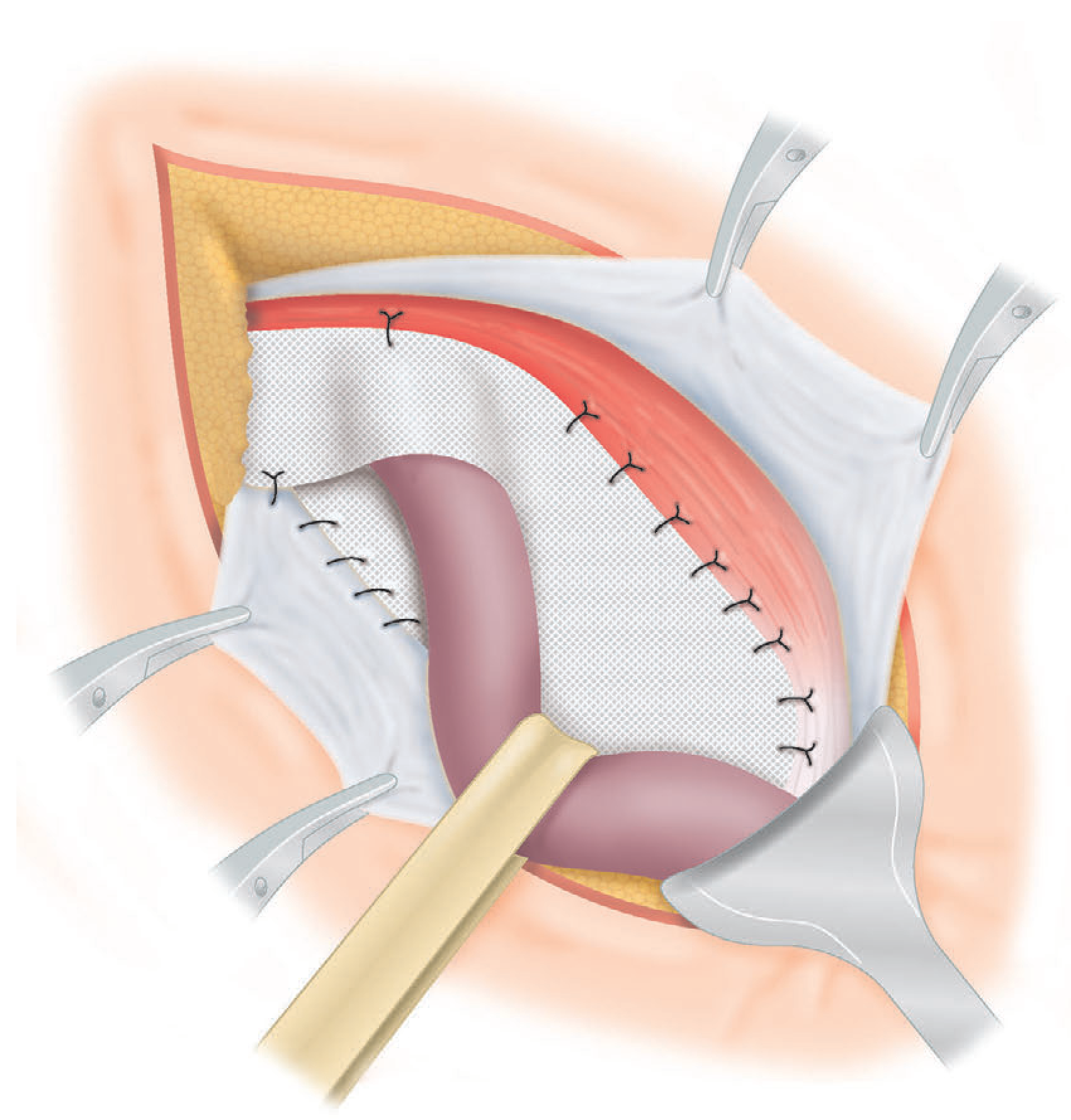
Figure: Lichtenstein's flat mesh repair (Bailey & Love)
3d. Open Plug/Complex Mesh Repair (Not Recommended)
Cone-shaped plugs are placed in the defect before a flat patch. Problems include: solidification of the plug (meshoma), migration, erosion into the bladder or cord. The 2018 European Hernia Society guidelines do not recommend mesh plugs or complex mesh systems over Lichtenstein.
3e. Open Preperitoneal Repair (Stoppa)
Midline incision, mesh placed in the preperitoneal space to cover the entire myopectineal orifice (bilateral). Indicated when multiple open repairs have failed. Now largely superseded by laparoscopic TEP.
3f. Laparoscopic Repair - TEP and TAPP
Both approaches place a 10 × 15 cm mesh in the extraperitoneal plane, covering:
- Hesselbach's triangle (direct hernia site)
- Deep inguinal ring (indirect hernia site)
- Femoral canal
TEP (Totally Extraperitoneal): Surgeon develops the preperitoneal space entirely without entering the peritoneal cavity. No need to close peritoneum. Technically more demanding.
TAPP (Transabdominal Preperitoneal): Surgeon enters the peritoneal cavity first through laparoscopic ports, then incises the peritoneum above the hernia to open the extraperitoneal space. Peritoneum is closed at the end to cover the mesh.
Advantages of laparoscopic over open:
- Reduced acute and chronic pain
- Faster return to full activity
- Fewer wound complications (infection, haematoma, seroma)
- Particularly beneficial for bilateral hernias (both sides repaired through the same ports) and recurrent hernias after previous open surgery (avoids re-entering scarred anterior tissue)
Disadvantages: Long learning curve; requires general anaesthesia; higher equipment costs; risk of rare but serious complications (bowel/vessel injury during trocar placement, mesh migration).
Robot-assisted laparoscopic repair is increasing in use. The enhanced 3D view and ergonomics benefit the surgeon, but no additional patient benefit has been demonstrated and cost remains difficult to justify for simple repairs.
3g. Special Situations
| Situation | Approach |
|---|---|
| Children | Herniotomy only (under GA) |
| Bilateral hernias | Laparoscopic preferred (single anaesthetic) |
| Recurrence after open | Laparoscopic TEP/TAPP preferred |
| Recurrence after laparoscopic | Open anterior approach |
| Strangulated/incarcerated | Emergency open repair; bowel resection if necrotic |
| Sliding hernia | Open repair with caution - bowel forms part of sac |
3h. Anaesthesia
Elective inguinal hernia repair can be performed under local, regional, or general anaesthesia with minimal risk even in high-risk patients. Local anaesthesia (field block with ilioinguinal/iliohypogastric nerve blocks) is appropriate for the Lichtenstein repair and reduces systemic risk.
Key Differentiating Points: Direct vs. Indirect
| Feature | Indirect | Direct |
|---|---|---|
| Position relative to epigastric vessels | Lateral | Medial |
| Hesselbach's triangle | No | Yes |
| Aetiology | Congenital or acquired | Always acquired |
| Can reach scrotum | Yes | No |
| Strangulation risk | Higher | Lower (broad neck) |
| Age | Any (peak in young and old) | Elderly |
Bailey and Love's Short Practice of Surgery, 28th Ed., Chapter 64, pp. 1087-1091 | Schwartz's Principles of Surgery, 11th Ed., Chapter 39 | Fischer's Mastery of Surgery, 8th Ed., Chapter on inguinofemoral hernias
Anal anatomy. dentate line anatomy
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have all the material needed. Let me compile a comprehensive, well-illustrated answer.
Anal Canal Anatomy and the Dentate Line
Sources: Bailey and Love's Short Practice of Surgery, 28th Ed. | Current Surgical Therapy, 14th Ed. | Sleisenger & Fordtran's Gastrointestinal and Liver Disease | Maingot's Abdominal Operations
1. Overview and Extent
The anal canal is the terminal segment of the large intestine, approximately 3-4 cm long in adults (slightly longer in males than females). It:
- Begins where the rectal ampulla narrows abruptly as the rectum passes through the pelvic diaphragm (levator ani) - marked by the palpable anorectal ring
- Ends at the anal verge - the mucocutaneous junction with hair-bearing perianal skin
Note: There is a useful distinction between the surgical anal canal (from anorectal ring to anal verge, ~4 cm) and the anatomical anal canal (from dentate line to anal verge, ~2 cm). Surgeons use the surgical definition.
Orientation: Because the anal canal slopes posteroinferiorly, an examining finger or instrument should be directed toward the umbilicus on insertion.
Relations:
- Posterior: anococcygeal ligament (separates it from the coccyx)
- Anterior: perineal body (separates it from the membranous urethra/penile bulb in males, or the lower vagina in females)
- Lateral: ischiorectal fossae
2. Key Diagram: Full Anal Canal Anatomy
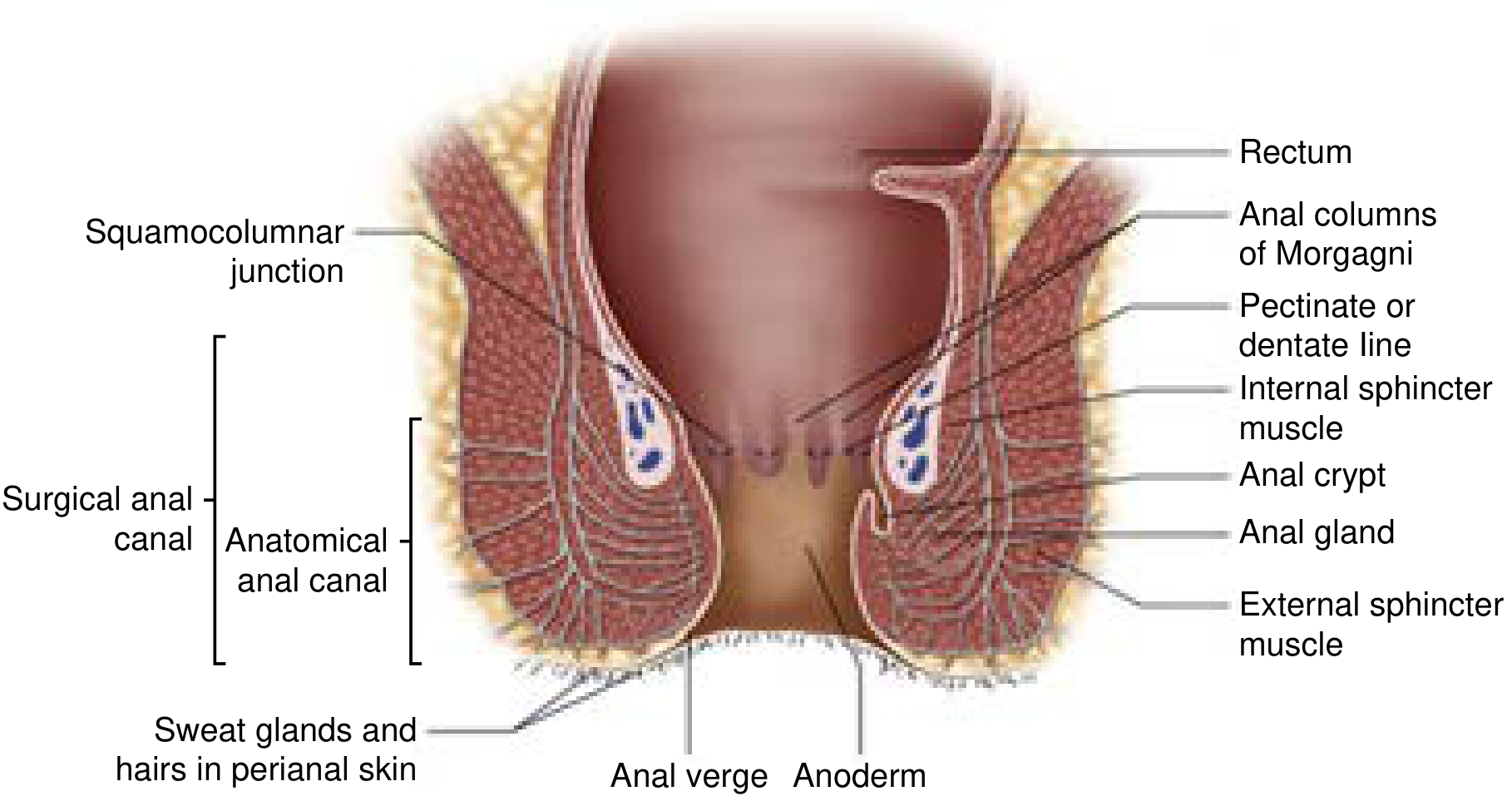
Anatomy of the anal canal showing the surgical and anatomical divisions, the dentate/pectinate line, columns of Morgagni, anal crypts, anal glands, and sphincter layers (Current Surgical Therapy, 14th Ed.)
3. The Sphincter Complex
3a. Internal Anal Sphincter (IAS)
- The thickened (2-5 mm) distal continuation of the circular smooth muscle of the rectum
- Involuntary muscle, controlled by the autonomic nervous system - predominantly responsible for resting anal tone (~85% of resting pressure)
- Surrounds the superior two-thirds of the anal canal
- Its lower border is palpable at the intersphincteric groove (white line of Hilton)
- Appears pearly-white when exposed at operation
- Relaxes in response to rectal distension (recto-anal inhibitory reflex) via intrinsic non-adrenergic, non-cholinergic fibres releasing nitric oxide
- Innervated by pelvic splanchnic (parasympathetic) nerves
3b. External Anal Sphincter (EAS)
- Forms the bulk of the sphincter complex
- Voluntary, striated (red) muscle - although traditionally divided into deep, superficial, and subcutaneous portions, it is functionally a single muscle (Goligher)
- Some fibres attach to the coccyx posteriorly; anteriorly they fuse with the perineal muscles
- Innervated by the pudendal nerve (S2, S3, S4)
3c. Puborectalis Muscle
- A U-shaped sling of levator ani arising from the pubic symphysis, looping around the posterior anorectal junction
- Maintains the anorectal angle (normally ~90°) - a critical component of continence
- Supplied by sacral somatic nerves
- Together with the deep external sphincter, forms the palpable anorectal ring at the top of the anal canal
3d. Longitudinal Muscle
- Continuation of the outer longitudinal smooth muscle of the rectum, augmented by striated muscle from the pelvic floor
- Passes between the external and internal sphincters, then splits into multiple terminal septa
- These septa insert into the skin of the anal canal and perianal skin, creating the intersphincteric plane
- During defecation: contracts to widen the lumen, flatten anal cushions, shorten the canal, and evert the anal margin
4. The Intersphincteric Plane
Between the external sphincter laterally and the longitudinal muscle medially lies the intersphincteric plane. This is:
- Where the anal intramuscular glands (6-10 in number) are located
- A key route for spread of anorectal infection (hence perianal and intersphincteric abscesses)
- A surgical access plane for sphincter-preserving procedures
5. The Epithelium: Three Zones
The lining of the anal canal changes from top to bottom across three distinct zones:
| Zone | Location | Epithelium | Sensation |
|---|---|---|---|
| Zone 1 | Proximal anal canal (above dentate) | Columnar (rectal-type mucosa) | Autonomic (pain-insensitive) |
| Zone 2 (ATZ) | Around the dentate line ± 1-2 cm | Transitional (cuboidal/squamous metaplasia) | Transitional |
| Zone 3 (Anoderm) | Below dentate to anal verge | Non-keratinised stratified squamous - no hair follicles or glands | Richly innervated somatic (highly sensitive) |
At the anal verge the epithelium becomes thicker and keratinised, with hair follicles, apocrine glands, and sweat glands - transitioning to true perianal skin.
6. The Dentate (Pectinate) Line - Central Landmark
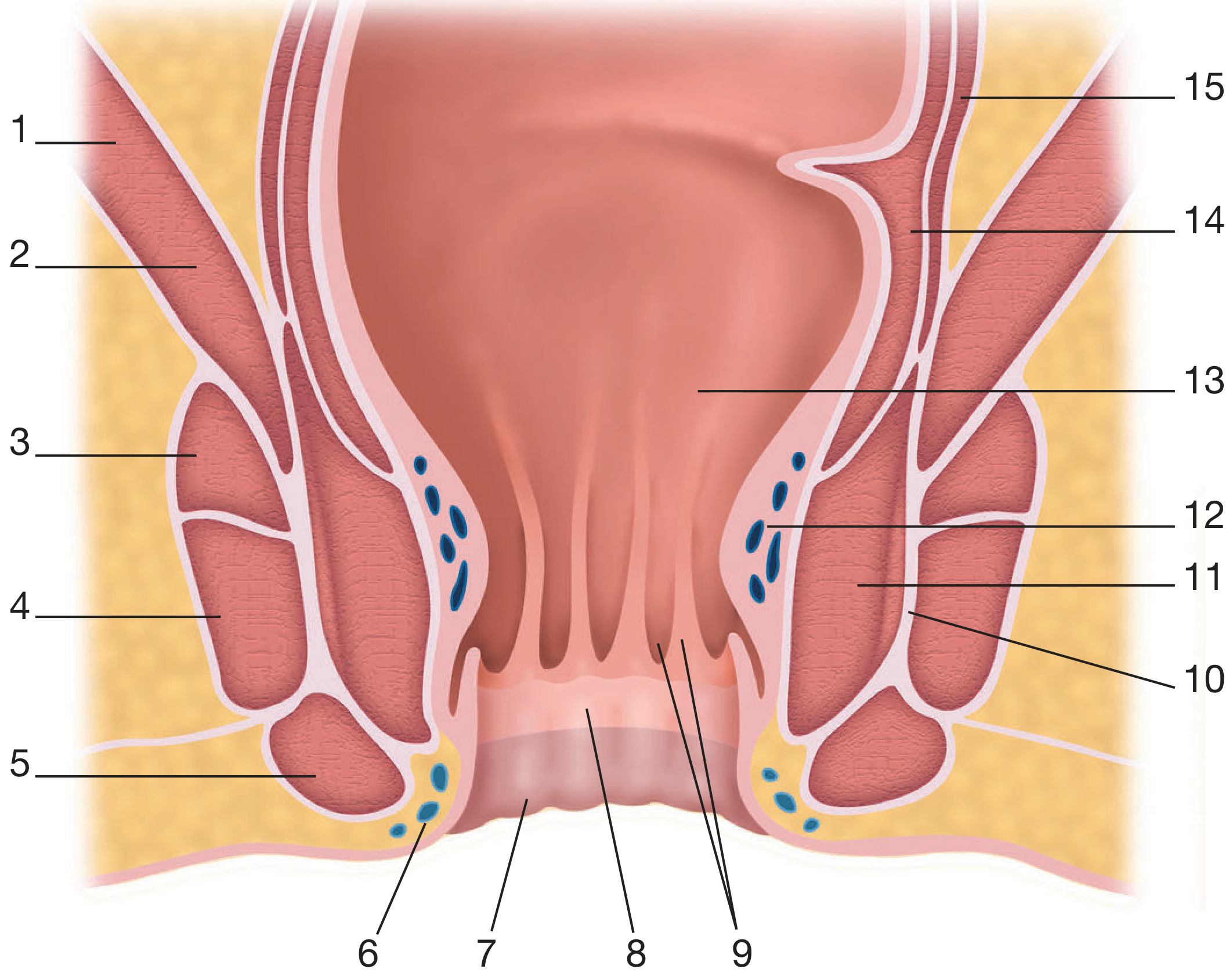
Coronal anatomy of the anal canal (Bailey & Love, adapted from Herold et al., Coloproctology)
The dentate line (also called the pectinate line) is one of the most important anatomical landmarks in colorectal surgery. It sits approximately 2 cm above the anal verge.
Formation
- As the rectum funnels into the narrower anal canal, the mucosa forms 8-12 vertical pleats - the Columns of Morgagni
- At their bases, the columns are connected by small mucosal folds called anal valves (or crypts of Morgagni)
- The row of alternating columns and crypts creates a serrated ("dentate") or comb-like ("pectinate") appearance - the dentate line
Embryological Significance
The dentate line marks the junction between endoderm (cloacal/hindgut origin, proximal) and ectoderm (proctodaeal invagination, distal). This single embryological fact explains the following major differences between tissue above and below:
Anal Glands
At the base of each anal crypt are small anal intramuscular glands (6-10 total). These:
- Extend into the internal sphincter and the intersphincteric space
- Secrete mucus to aid defecation
- If blocked - become the source of anal abscesses and fistula-in-ano
7. Comparison: Above vs. Below the Dentate Line
This is one of the most commonly examined topics in surgery and gastroenterology:
| Feature | Above Dentate Line | Below Dentate Line |
|---|---|---|
| Embryology | Endoderm (cloacal/hindgut) | Ectoderm (proctodaeum) |
| Epithelium | Columnar / transitional | Non-keratinised squamous (anoderm) |
| Pain sensation | Absent (visceral/autonomic) | Present (somatic, very sensitive) |
| Arterial supply | Superior rectal artery (from IMA) | Inferior rectal artery (from pudendal/internal iliac) |
| Venous drainage | Superior rectal vein → portal system | Inferior rectal/pudendal veins → systemic (internal iliac) |
| Lymphatic drainage | Internal iliac nodes / inferior mesenteric nodes | Inguinal lymph nodes |
| Nerve supply | Autonomic (sympathetic + parasympathetic) | Somatic (pudendal nerve) |
| Pathology above | Internal haemorrhoids; adenocarcinoma; non-keratinising SCC | - |
| Pathology below | - | External haemorrhoids; anal tags; keratinising SCC; perianal warts |
Clinical Pearls from the Dentate Line
- Biopsy above the dentate line: no anaesthesia needed - the area is pain-insensitive
- Rubber band ligation of haemorrhoids: bands must be placed above the dentate line, or the patient will experience severe pain (somatic innervation below)
- Inguinal lymphadenopathy in the absence of obvious leg pathology: always examine the anal canal - a tumour below the dentate line drains to inguinal nodes
- Posterior midline ischaemia: the posterior anal canal is the least well-perfused zone (85% of people), which is why chronic anal fissures occur most commonly at the posterior commissure and why vasodilators (glyceryl trinitrate, diltiazem) aid healing
8. Vasculature of the Anal Canal
Arterial Supply
| Artery | Territory | Origin |
|---|---|---|
| Superior rectal artery | Proximal anal canal, columns | Inferior mesenteric artery |
| Middle rectal artery | Mid anal canal | Internal iliac artery |
| Inferior rectal artery | Distal canal, external sphincter | Internal pudendal artery |
The three sources anastomose freely, giving the anal canal a rich blood supply.
Venous Drainage
- Superior (internal) haemorrhoidal plexus: drains above the dentate line → superior rectal vein → portal system (inferior mesenteric vein)
- Inferior (external) haemorrhoidal plexus: drains below the dentate line → inferior rectal and pudendal veins → internal iliac vein → systemic circulation
The submucosa contains a mucosal suspensory ligament (fibromuscular mesh from the longitudinal muscle) that separates the two plexuses and tethers the mucosa below the dentate line more firmly than above. With ageing this mesh is progressively replaced by fibroelastic tissue, which becomes fragmented - contributing to the downward displacement of anal cushions and haemorrhoid formation.
Anal Cushions
Three discrete submucosal vascular cushions (at 3, 7, and 11 o'clock in the lithotomy position) contribute to the airtight seal of the anal canal at rest. During defecation, the longitudinal muscle flattens them; on relaxation they distend again to restore the seal.
9. Lymphatic Drainage
- Above the dentate line: drains via superior rectal lymphatics to inferior mesenteric nodes, and laterally via middle/inferior rectal vessels to internal iliac nodes
- Below the dentate line: drains to superficial inguinal then deep inguinal lymph nodes
- Tumours in the Anal Transition Zone (ATZ) may follow either route
10. Nerve Supply
| Region | Nerves | Type |
|---|---|---|
| Above dentate | Pelvic splanchnic (S2-4, parasympathetic); sympathetic via hypogastric plexus | Autonomic; pain-insensitive |
| Below dentate (anoderm) | Pudendal nerve (S2-4) | Somatic; highly sensitive (pain, touch, temperature) |
| Internal sphincter | Autonomic (sympathetic = contraction; parasympathetic/NO = relaxation) | Involuntary |
| External sphincter | Pudendal nerve (inferior rectal branch) | Voluntary |
| Puborectalis | Sacral somatic nerves (S3-4) | Voluntary |
Bailey and Love's Short Practice of Surgery, 28th Ed., Chapter 80 | Sleisenger & Fordtran's GI and Liver Disease, Chapter 129 | Current Surgical Therapy, 14th Ed. | Maingot's Abdominal Operations, Chapter 42
Thyroid anatomy and physiology. Thyroiditis. Thyroid nodules, solitary nodule. Benign and malignant conditions of the thyroid gland.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material. Let me compile the full answer.
Thyroid Gland: Anatomy, Physiology, Thyroiditis, Nodules, and Tumours
Sources: Guyton & Hall Medical Physiology | Bailey & Love's Surgery, 28th Ed. | Robbins & Cotran Pathologic Basis of Disease | Schwartz's Principles of Surgery, 11th Ed. | Fischer's Mastery of Surgery, 8th Ed.
1. Anatomy
Gross Anatomy
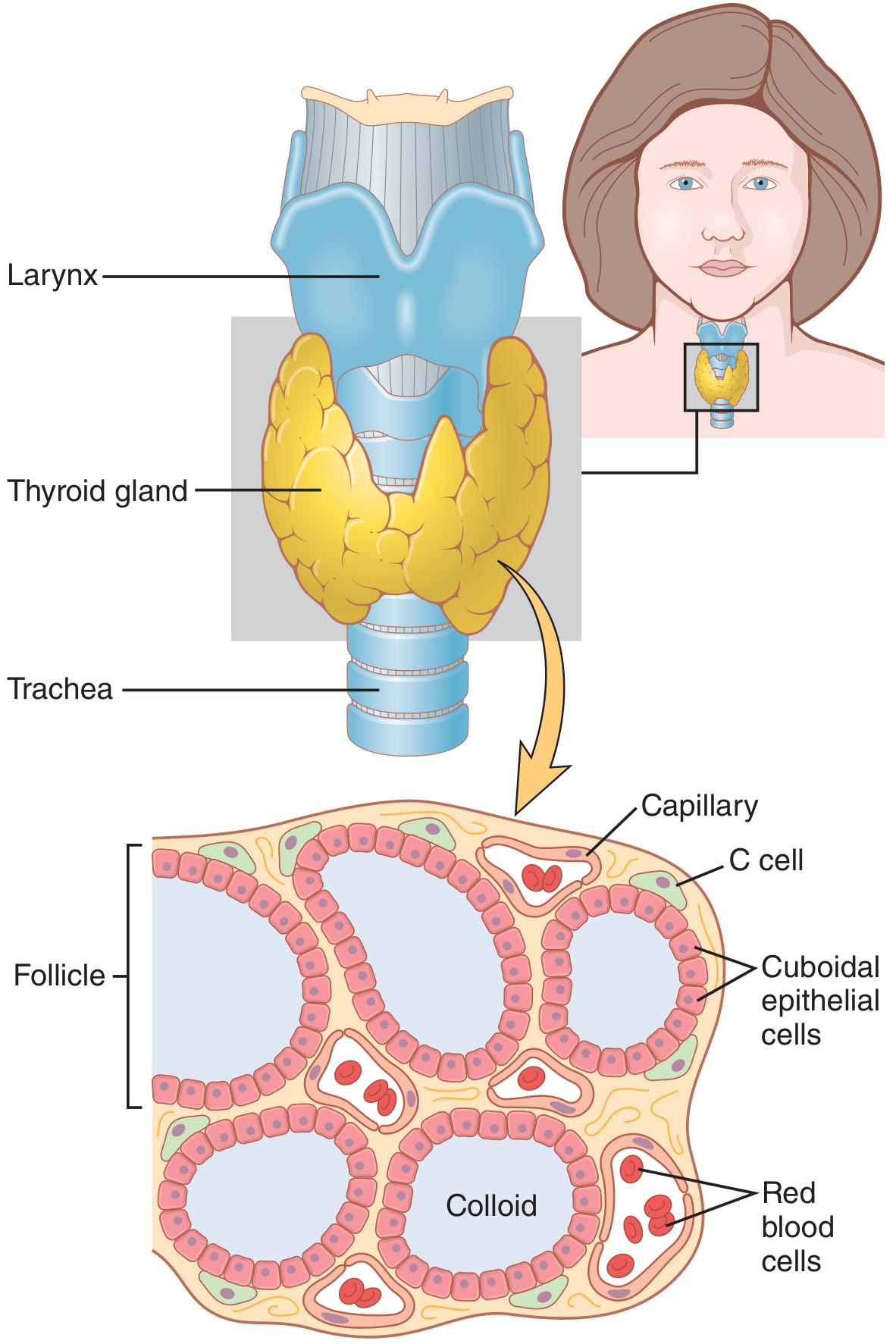
Figure: Gross and microscopic anatomy of the thyroid gland (Guyton & Hall)
The thyroid gland lies in the anterior neck, straddling the trachea below the larynx. It consists of two lateral lobes connected by a narrow isthmus at the level of the 2nd-3rd tracheal rings. A pyramidal lobe may ascend from the isthmus (a remnant of the thyroglossal duct) in about 50% of people.
Relations:
- Anterolateral: strap muscles (sternohyoid, sternothyroid, omohyoid)
- Posterior: trachea and oesophagus
- Posterolateral: carotid sheath (common carotid artery, internal jugular vein, vagus nerve)
- The space between the thyroid and carotid sheath contains the recurrent laryngeal nerve (RLN), the inferior thyroid artery, and the parathyroid glands
Vasculature:
- Superior thyroid artery (from external carotid) - enters the apex of each lobe
- Inferior thyroid artery (from thyrocervical trunk of subclavian) - the most important, as it runs alongside the RLN
- The inferior thyroid artery and the RLN cross each other in a variable and surgically important relationship
- Thyroid ima artery - inconstant, runs directly from the aorta
- Venous drainage: superior and middle thyroid veins → internal jugular; inferior thyroid veins → brachiocephalic
Lymphatics: drain to prelaryngeal (Delphian node), pretracheal, and deep cervical nodes.
Nerve supply:
- Sympathetic: superior and inferior cervical ganglia (vasoconstriction)
- The recurrent laryngeal nerve is not a thyroid nerve but is intimately related to the gland during surgery - it innervates all intrinsic laryngeal muscles except cricothyroid. Damage causes hoarseness (unilateral) or airway obstruction (bilateral)
- The superior laryngeal nerve (external branch) supplies the cricothyroid muscle and may be damaged during ligation of the superior thyroid artery
Parathyroid glands: typically four, located on the posterior surface of the thyroid. The superior pair lies consistently posterior to the RLN above the inferior thyroid artery crossing. The inferior pair is more variable.
Microscopic Anatomy
The gland is composed of:
- Follicles (100-300 µm diameter): spherical units lined by cuboidal follicular epithelial cells, enclosing a lumen filled with colloid (principally thyroglobulin). These cells are responsible for T3/T4 synthesis.
- Parafollicular C cells: scattered between follicles, produce calcitonin, which lowers plasma calcium. These are the origin of medullary thyroid carcinoma.
- Rich capillary network: thyroid blood flow is ~5× its weight per minute
2. Thyroid Hormone Physiology
Synthesis Pathway
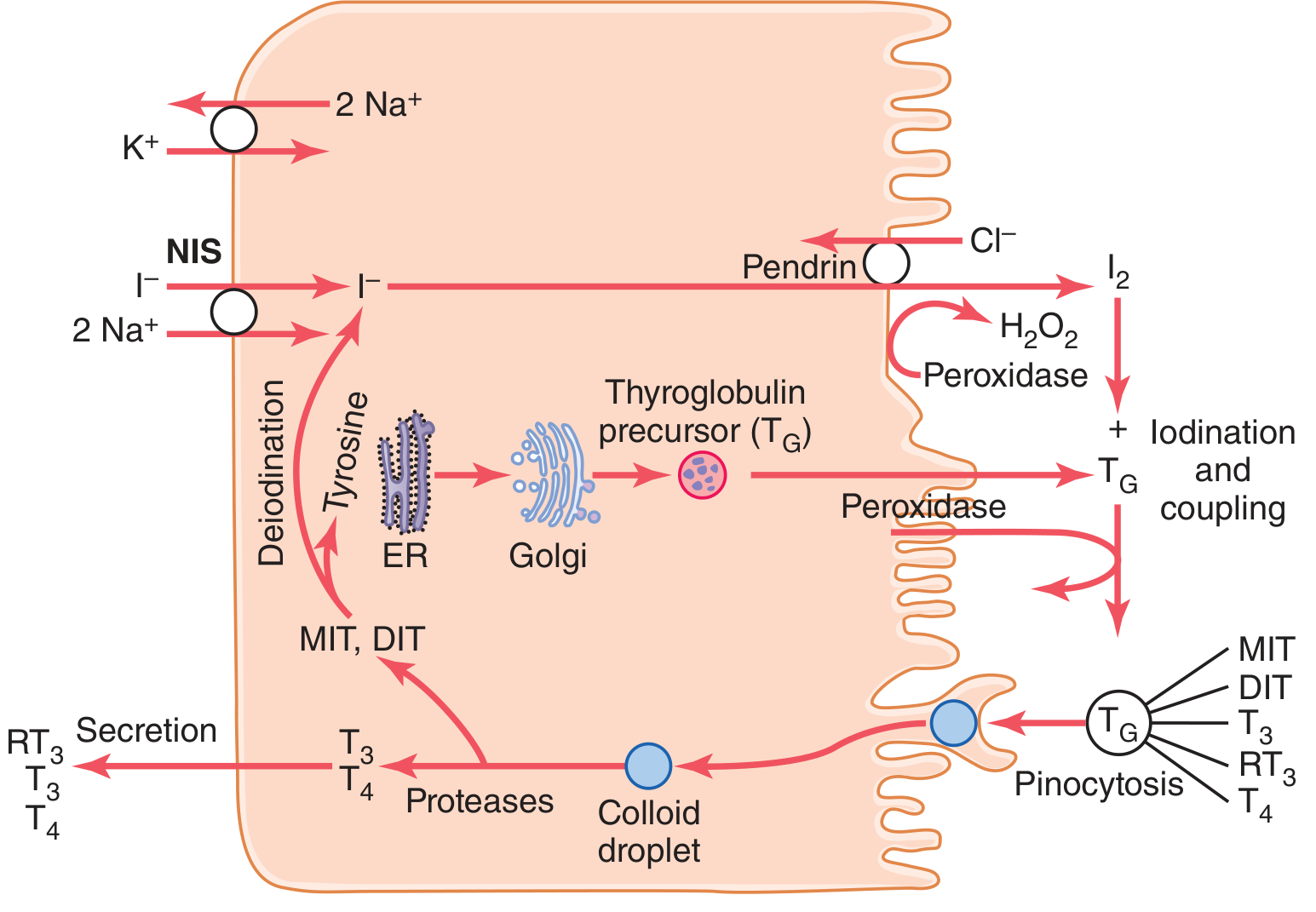
Figure: Thyroid hormone synthesis steps (Guyton & Hall, Fig. 77.2)
Step 1 - Iodide trapping: Iodide (I⁻) is actively transported from blood into the follicular cell via the sodium-iodide symporter (NIS) on the basolateral membrane, co-transporting 2 Na⁺. Energy is derived from the Na⁺/K⁺ ATPase. Normal concentration ratio = 30×; maximally stimulated = 250×.
Step 2 - Iodide transport to colloid: Iodide crosses the apical membrane via pendrin (chloride-iodide counter-transporter) into the follicle lumen.
Step 3 - Thyroglobulin synthesis: Follicular cells synthesize thyroglobulin (MW ~335,000; contains ~70 tyrosine residues) in the ER/Golgi and secrete it into the colloid.
Step 4 - Oxidation and organification: Iodide is oxidised to iodine by thyroid peroxidase (TPO) using H₂O₂. Iodine then attaches to tyrosine residues on thyroglobulin, forming monoiodotyrosine (MIT) and diiodotyrosine (DIT).
Step 5 - Coupling: TPO catalyses coupling: MIT + DIT = T3 (triiodothyronine); DIT + DIT = T4 (thyroxine). T4 is the predominant product.
Step 6 - Secretion: TSH stimulates pinocytosis of colloid, fusion with lysosomes, and proteolytic cleavage of thyroglobulin. Free T3 and T4 are released into the bloodstream. MIT and DIT are deiodinated and the iodide is recycled.
About 50 mg of iodine per year is required for normal hormone production (~1 mg/week). Common table salt is iodised at 1:100,000 to prevent deficiency.
Regulation
- TSH (thyrotropin) from the anterior pituitary is the primary driver of thyroid function - stimulates all steps of synthesis, iodide trapping, and follicular cell growth
- TRH (thyrotropin-releasing hormone) from the hypothalamus stimulates TSH release
- Negative feedback: rising T3/T4 inhibit both TRH and TSH release
T3 vs. T4
| Feature | T4 (Thyroxine) | T3 (Triiodothyronine) |
|---|---|---|
| Amount secreted | ~90% | ~10% |
| Peripheral conversion | Deiodination → T3 | Active form |
| Potency | Less active (prohormone) | 3-5× more potent |
| Half-life | ~7 days | ~1 day |
Actions: regulate basal metabolic rate, protein synthesis, cardiac output, thermogenesis, CNS development (critical in foetal/neonatal life), and bone metabolism.
3. Thyroiditis
Thyroiditis encompasses several forms of thyroid inflammation.
3a. Hashimoto's Thyroiditis (Chronic Autoimmune Thyroiditis)
The most common cause of hypothyroidism in iodine-sufficient regions.
Epidemiology: Peak age 45-65 years; female:male = 10:1 to 20:1. Leading cause of non-endemic goitre in children.
Pathogenesis: Autoimmune breakdown of self-tolerance to thyroid antigens. Key mechanisms:
- CD8+ cytotoxic T cells directly destroy follicular cells
- CD4+ Th1 cells release IFN-γ → macrophage activation → follicle damage
- Autoantibodies to thyroglobulin and thyroid peroxidase (TPO) present in the vast majority of patients
- Genetic predisposition: CTLA4, PTPN22, IL2RA gene polymorphisms (shared with other autoimmune diseases)
Pathology: Diffuse gland enlargement (well-demarcated from surrounding structures); pale, yellow-tan cut surface. Histologically:
- Dense mononuclear infiltrate with lymphoid follicles and germinal centres
- Oncocytic (Hürthle cell) change of follicular epithelium - pink, granular cytoplasm
- Follicular atrophy and variable fibrosis
- Classic FNA appearance: oncocytes + heterogeneous lymphocytes
Clinical Features: Usually presents as painless diffuse goitre with hypothyroidism developing gradually. Occasional early transient thyrotoxicosis ("hashitoxicosis") from follicle rupture. As disease progresses: T4/T3 fall, TSH rises compensatorily.
Associations: Type 1 diabetes, Addison's disease, SLE, myasthenia gravis, Sjögren's syndrome. Increased risk of extranodal marginal zone B-cell lymphoma of the thyroid. Possible predisposition to papillary carcinoma (debated).
3b. Subacute Granulomatous Thyroiditis (de Quervain's Thyroiditis)
Aetiology: Follows a viral infection (mumps, Coxsackie, adenovirus).
Clinical: Pain in the neck, fever, malaise, firm irregular goitre. In 10% the onset is acute and very painful with transient hyperthyroidism. In one-third: asymptomatic except for a goitre.
Investigations: Raised inflammatory markers (ESR, CRP), absent thyroid antibodies, serum T4 high-normal or mildly elevated, ¹²³I uptake low (distinguishes from Graves' disease).
Natural course: Self-limiting over several months. Typically: thyrotoxic phase → hypothyroid phase → euthyroid recovery.
Treatment: Prednisone 10-20 mg/day for 7 days, then taper over a month. Thyroxine replacement if hypothyroidism is prominent. Aspirin/NSAIDs for milder cases.
3c. Chronic Lymphocytic (Silent/Painless) Thyroiditis
Similar to Hashimoto's histologically but typically painless and transient. Occurs especially in the postpartum setting (postpartum thyroiditis). Usually self-limiting.
3d. Riedel's Thyroiditis
Very rare (<0.5% of goitres). Thyroid tissue replaced by dense fibrous tissue that infiltrates beyond the capsule into adjacent muscles, parathyroids, RLNs, and carotid sheath. Associated with systemic fibrosclerosis (retroperitoneal fibrosis, mediastinal fibrosis). The gland feels rock hard and fixed - must be distinguished from anaplastic carcinoma by biopsy (wedge of isthmus). Treatment: high-dose steroids, tamoxifen, thyroxine replacement.
4. Thyroid Nodules and the Solitary Nodule
Epidemiology
Palpable thyroid nodules occur in approximately 4% of the US population. Thyroid cancer incidence is ~40 new cases per 1 million. The critical clinical task is identifying which nodules harbour malignancy.
Risk Factors for Malignancy in a Nodule
- History of ionizing radiation exposure (especially childhood radiation for tinea capitis, thymic enlargement, Hodgkin's disease). Risk is maximal 20-30 years post-exposure; 40% of post-radiation nodules are malignant
- Family history of thyroid cancer or associated syndromes (MEN2, Cowden syndrome, FAP)
- Male sex (a nodule in a male carries higher risk)
- Age extremes (very young or elderly)
- Rapid growth, fixation, vocal cord paralysis (hoarseness), dysphagia, cervical lymphadenopathy
Evaluation of the Solitary Thyroid Nodule
History: Duration, growth rate, pain (unusual - raises suspicion for intranodal haemorrhage, thyroiditis, or malignancy), dysphagia, dyspnoea, hoarseness, dull aching pain (suggests MTC), family history, radiation exposure.
Examination: Nodule characteristics, cervical lymph nodes, voice quality, signs of hypo/hyperthyroidism.
Investigations:
-
TSH - first test in all patients. Low TSH → radionuclide scan (functioning/"hot" nodule rarely malignant). Normal/high TSH → proceed to ultrasound.
-
Ultrasound - primary imaging tool. Suspicious features:
- Hypoechoic
- Irregular or ill-defined margins
- Microcalcifications
- Taller-than-wide orientation (in transverse plane)
- Loss of fatty hilum in lymph nodes, peripheral vascularity
-
TI-RADS (Thyroid Imaging Reporting and Data System) by the American College of Radiology - stratifies nodules by risk and guides FNA threshold.
-
Fine-Needle Aspiration Biopsy (FNAB) - the key diagnostic test. Results classified by the Bethesda System:
| Bethesda Category | Diagnosis | Malignancy Risk | Management |
|---|---|---|---|
| I | Non-diagnostic | 1-4% | Repeat FNA |
| II | Benign | 0-3% | Observation |
| III | AUS/FLUS | 10-30% | Repeat FNA or molecular testing |
| IV | Follicular neoplasm | 25-40% | Diagnostic lobectomy or molecular testing |
| V | Suspicious for malignancy | 50-75% | Surgery |
| VI | Malignant | 97-99% | Surgery |
Up to 5% of FNA results are overtly malignant; ~20% are indeterminate (Bethesda III-V).
-
Molecular testing (e.g., ThyroSeq, Afirma) - used for indeterminate Bethesda III/IV nodules to stratify malignancy risk and guide surgical decision-making.
-
Cross-sectional imaging (CT/MRI) - for suspected invasive tumour, retrosternal extension, bulky lymphadenopathy, or compressive symptoms. Pemberton's sign (facial congestion/JVD when arms raised) suggests SVC obstruction from retrosternal goitre.
-
Laryngoscopy - all patients with subjective voice change, prior neck surgery, or suspected posterior extrathyroidal extension.
5. Benign Conditions of the Thyroid Gland
5a. Follicular Adenoma
The most common benign thyroid neoplasm. A solitary, encapsulated lesion of follicular epithelium with a complete fibrous capsule - no capsular or vascular invasion (this distinguishes it from follicular carcinoma on histology). FNA cannot reliably distinguish adenoma from follicular carcinoma - a surgical specimen is needed to assess the capsule.
5b. Toxic Adenoma (Plummer's Disease)
A hyperfunctioning follicular adenoma - produces T3/T4 autonomously. Appears as a "hot nodule" on radionuclide scan. Risk of malignancy is very low. Treatment: radioiodine or surgery.
5c. Multinodular Goitre
Diffuse or nodular enlargement due to follicular hyperplasia, often related to iodine deficiency. May cause compressive symptoms (tracheal deviation, SVC obstruction). Treatment: medical (thyroxine) or surgical (thyroidectomy) for compressive symptoms.
5d. Graves' Disease
The most common cause of endogenous hyperthyroidism. Autoimmune - thyroid-stimulating immunoglobulin (TSI) binds and activates the TSH receptor in ~90% of patients. Classic triad:
- Hyperthyroidism with diffuse goitre
- Infiltrative ophthalmopathy (exophthalmos) - mediated by TSH-receptor antibodies activating retro-orbital fibroblasts → glycosaminoglycan accumulation
- Pretibial myxoedema (infiltrative dermopathy) - minority of patients
Genetic overlap with Hashimoto's (CTLA4, PTPN22, IL2RA polymorphisms; TSHR gene variants specifically). Female:male = 5-10:1; peak 20-50 years. Treatment: antithyroid drugs (carbimazole/propylthiouracil), radioiodine, or thyroidectomy.
6. Malignant Conditions of the Thyroid Gland
Thyroid cancers are predominantly (>95%) well-differentiated and carry an excellent prognosis. They are more common in women (3:1).
Overview of Thyroid Carcinomas
| Type | % of Thyroid Ca | Origin | Prognosis |
|---|---|---|---|
| Papillary | ~80% | Follicular epithelium | Excellent (>95% 10-yr survival) |
| Follicular | ~10-15% | Follicular epithelium | Good (depends on invasion) |
| Hürthle cell | ~3-5% | Follicular epithelium | Intermediate |
| Medullary | ~1-2% | Parafollicular C cells | Intermediate |
| Anaplastic | ~1-2% | Follicular epithelium | Very poor (~100% mortality) |
6a. Papillary Thyroid Carcinoma (PTC)
The most common thyroid malignancy - 80% of all thyroid cancers in iodine-sufficient areas. Predominant cancer in children and radiation-exposed individuals. F:M = 2:1; mean age 30-40 years.
Molecular pathogenesis: Activation of the MAP kinase pathway by mutually exclusive mechanisms:
- BRAF mutation (most common, 40-65%) - V600E variant associated with extrathyroidal extension, lymph node metastasis, and worse prognosis
- RET/PTC rearrangements (10-20%) - especially in children post-radiation
- NTRK1 rearrangements (10-20%)
- RAS mutations (10-30%)
Gross: Hard, whitish; remains flat on sectioning (unlike benign nodules that bulge). Macroscopic calcification, cystic change possible.
Histology: Papillary projections (fronds of fibrovascular stroma covered by neoplastic epithelium), or follicular variant. Diagnosis is based on characteristic nuclear features:
- Pale, glassy nuclei ("ground-glass" or "Orphan Annie eye" nuclei)
- Nuclear grooves
- Intranuclear cytoplasmic inclusions (pseudoinclusions)
- Psammoma bodies - concentric calcified deposits (~40% of cases), representing calcified sloughed cells; virtually pathognomonic when found in a thyroid FNA
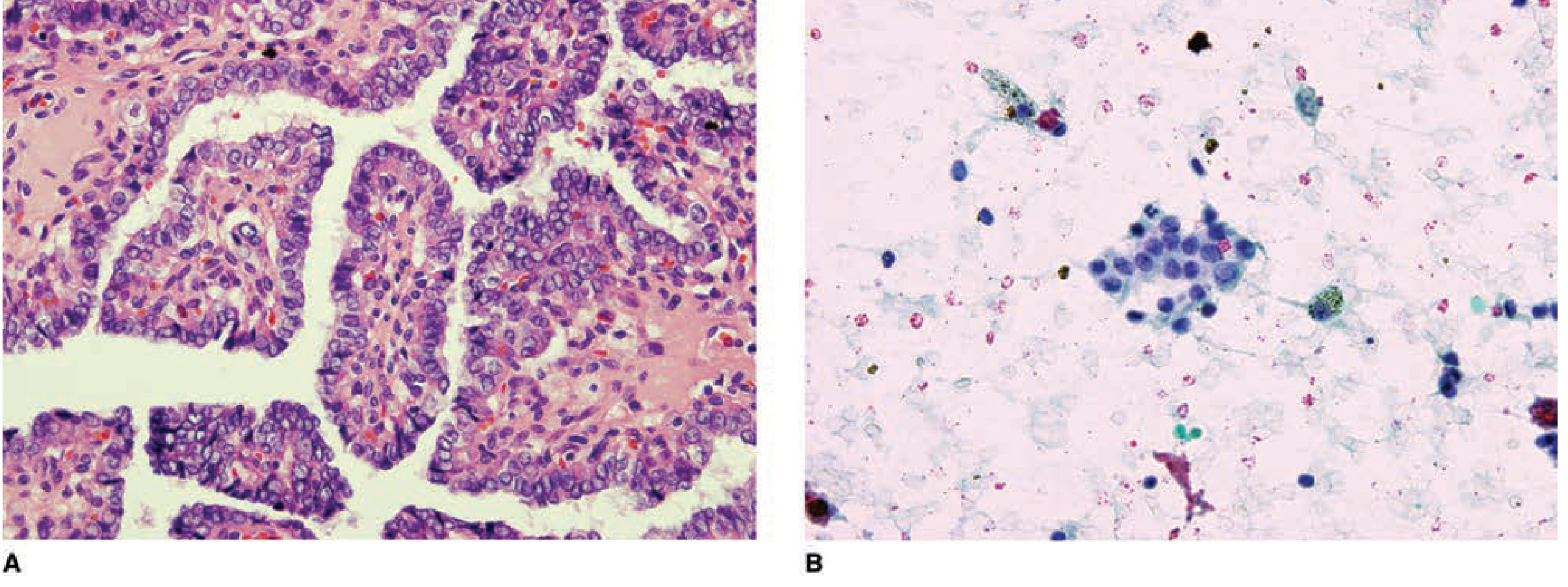
Figure: A. Papillary carcinoma histology (H&E). B. FNAB showing Orphan Annie nuclear inclusions (Schwartz's Principles of Surgery)
Multifocality: Present in up to 85% on microscopic examination.
Spread: Characteristically by lymphatics → cervical nodes. "Lateral aberrant thyroid" in a lymph node almost always represents metastatic PTC. Haematogenous spread (to lung, bone) occurs in up to 20% over the course of disease.
Key variant: NIFTP (Non-Invasive Follicular Thyroid Neoplasm with Papillary-like nuclear features) - formerly encapsulated follicular variant of PTC. No capsular invasion; behaves indolently; no longer classified as carcinoma.
Prognosis: >95% 10-year survival. Prognostic systems include AGES, MACIS, AMES, and TNM. High-risk features: age >55, tumour >4 cm, extrathyroidal extension, distant metastases, BRAF V600E mutation, TERT promoter mutation.
Treatment: Total/near-total thyroidectomy for high-risk or bilateral disease; hemithyroidectomy for low-risk, small, unilateral tumours. Central neck dissection for node-positive disease. Post-operative radioactive iodine (RAI) ablation for high-risk patients. Long-term TSH suppression with levothyroxine. Thyroglobulin monitoring for recurrence.
6b. Follicular Thyroid Carcinoma (FTC)
~10-15% of thyroid cancers. More common in iodine-deficient areas. Peak age 40-60 years.
Key distinction from adenoma: Capsular and/or vascular invasion - this can only be assessed on the entire surgical specimen, not by FNA. Hence FNA cannot diagnose FTC.
Molecular: RAS mutations, PIK3CA gain-of-function, PTEN loss-of-function, and the characteristic PAX8-PPAR-γ translocation (found in up to 50%).
Gross: Solitary, well-encapsulated (minimally invasive) or widely invasive tumour replacing the lobe (see image above).
Spread: Characteristically haematogenous to lungs, bone, liver (in contrast to PTC's lymphatic spread). Regional lymph node metastases uncommon.
Prognosis: Variable - minimally invasive (<10% die within 10 years); widely invasive (~50% die within 10 years).
Treatment: Total thyroidectomy. RAI useful as well-differentiated metastases may concentrate radioiodine.
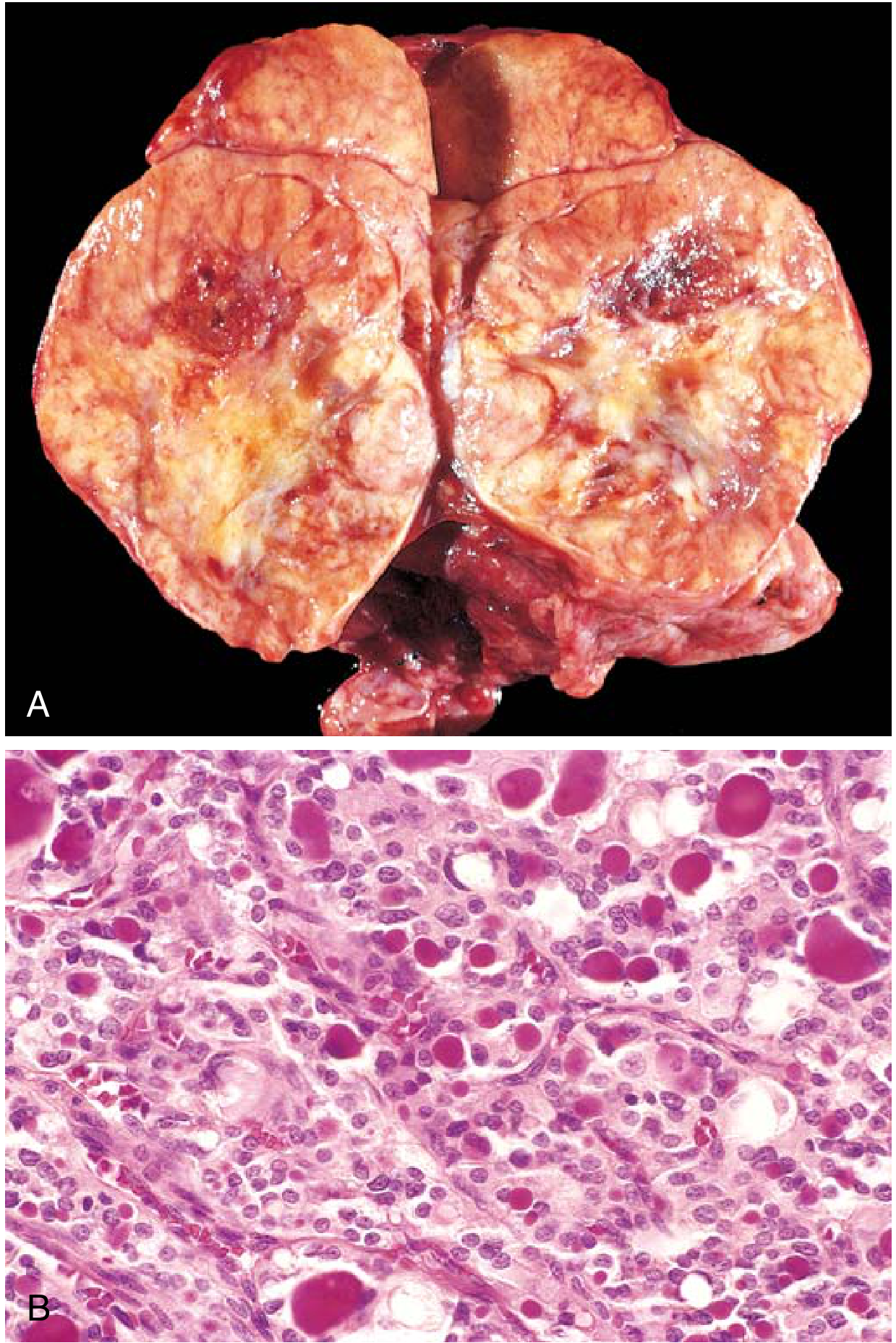
Figure: Follicular thyroid carcinoma (Robbins & Cotran)
6c. Hürthle Cell (Oncocytic) Thyroid Carcinoma
Variant of follicular carcinoma composed of oncocytic (Hürthle/Askenazy) cells. Distinguished by being less likely to take up RAI, making RAI ablation less effective.
6d. Medullary Thyroid Carcinoma (MTC)
Derived from parafollicular C cells; located at the junction of the upper one-third and lower two-thirds of the thyroid parenchyma. Now accounts for ~1-2% of thyroid cancers.
Key features:
- Secretes calcitonin (tumour marker) and often CEA
- 75% sporadic (typically 4th-6th decade); 25% hereditary
- All patients require genetic testing for RET mutations regardless of family history (7% of apparently sporadic cases carry germline mutations)
Hereditary syndromes (RET germline mutations):
- MEN2A (95% of MEN2): MTC + pheochromocytoma + primary hyperparathyroidism - autosomal dominant
- MEN2B: MTC + pheochromocytoma + mucosal neuromas + intestinal ganglioneuromatosis + marfanoid habitus - MTC is often aggressive, presents early
- Familial MTC (FMTC): MTC only, no PHEO or PHPT
Somatic RET mutation in ~50% of sporadic cases.
Workup: Basal calcitonin, CEA, screen for pheochromocytoma (24-hr urine/plasma metanephrines - must be excluded before surgery), serum calcium. Neck ultrasound + FNA. Genetic testing for germline RET.
Histology: Sheets or nests of polygonal to spindle-shaped cells with granular cytoplasm; amyloid deposits in the stroma (from procalcitonin).
Treatment: Total thyroidectomy + central neck dissection. Patients with RET mutations may undergo prophylactic thyroidectomy.
6e. Anaplastic (Undifferentiated) Thyroid Carcinoma (ATC)
The most aggressive thyroid malignancy. Mortality ~100%; mean survival ~6 months. Mean age 65-71 years; 60-70% women.
Pathogenesis: Most arise by dedifferentiation of pre-existing well-differentiated carcinoma (over half have concurrent or prior well-differentiated cancer; >80% have a history of thyroid nodules). Key molecular event: TP53 loss-of-function mutation (not seen in well-differentiated cancers). Also harbours RAS, PIK3CA mutations. Risk factors: prior neck irradiation, iodine deficiency.
Presentation: Rapidly enlarging, bulky, fixed neck mass causing airway obstruction, dysphagia, hoarseness.
Histology: Highly anaplastic cells - large pleomorphic, spindle-shaped cells, or a mixed pattern. Extensive necrosis.
Treatment: Combination of surgery (if resectable), radiotherapy, and chemotherapy. Tyrosine kinase inhibitors (lenvatinib, sorafenib, dabrafenib + trametinib for BRAF-mutated cases). 2021 ATA guidelines guide current management. Death usually results from local invasion and airway compromise rather than distant metastases.
Summary Table: Thyroid Carcinoma Features
| Feature | Papillary | Follicular | Medullary | Anaplastic |
|---|---|---|---|---|
| Origin | Follicular cells | Follicular cells | C cells | Follicular cells |
| Frequency | 80% | 10-15% | 1-2% | 1-2% |
| Spread | Lymphatic | Haematogenous | Both | Local invasion |
| Key histology | Orphan Annie nuclei, psammoma bodies | Capsular/vascular invasion | Amyloid, calcitonin | Pleomorphic, anaplastic |
| Key mutation | BRAF V600E | PAX8-PPARγ, RAS | RET (germline + somatic) | TP53 loss |
| Tumour marker | Thyroglobulin | Thyroglobulin | Calcitonin, CEA | - |
| RAI uptake | Yes | Yes (well-diff metastases) | No | No |
| Prognosis | Excellent (>95% 10-yr) | Good to fair | Intermediate | Lethal |
Guyton & Hall Textbook of Medical Physiology, Chapter 77 | Bailey & Love's Surgery, 28th Ed., Chapter 55 | Robbins & Cotran Pathologic Basis of Disease, Chapter 24 | Schwartz's Principles of Surgery, 11th Ed., Chapter 38 | Fischer's Mastery of Surgery, 8th Ed., Chapter 34
This is a shared conversation. Sign in to Orris to start your own chat.