Structure and properties of cardiac muscle and mechanism of cardiac muscle contraction for 15marks refer mbbs textbooks
Structure and Properties of Cardiac Muscle, and Mechanism of Cardiac Muscle Contraction
I. STRUCTURE OF CARDIAC MUSCLE
A. General Organisation
- Guyton and Hall Textbook of Medical Physiology
- Junqueira's Basic Histology, 17e
B. Microscopic (Histological) Structure
- Each cardiac myocyte is approximately 15-30 μm in diameter and 80 μm in length
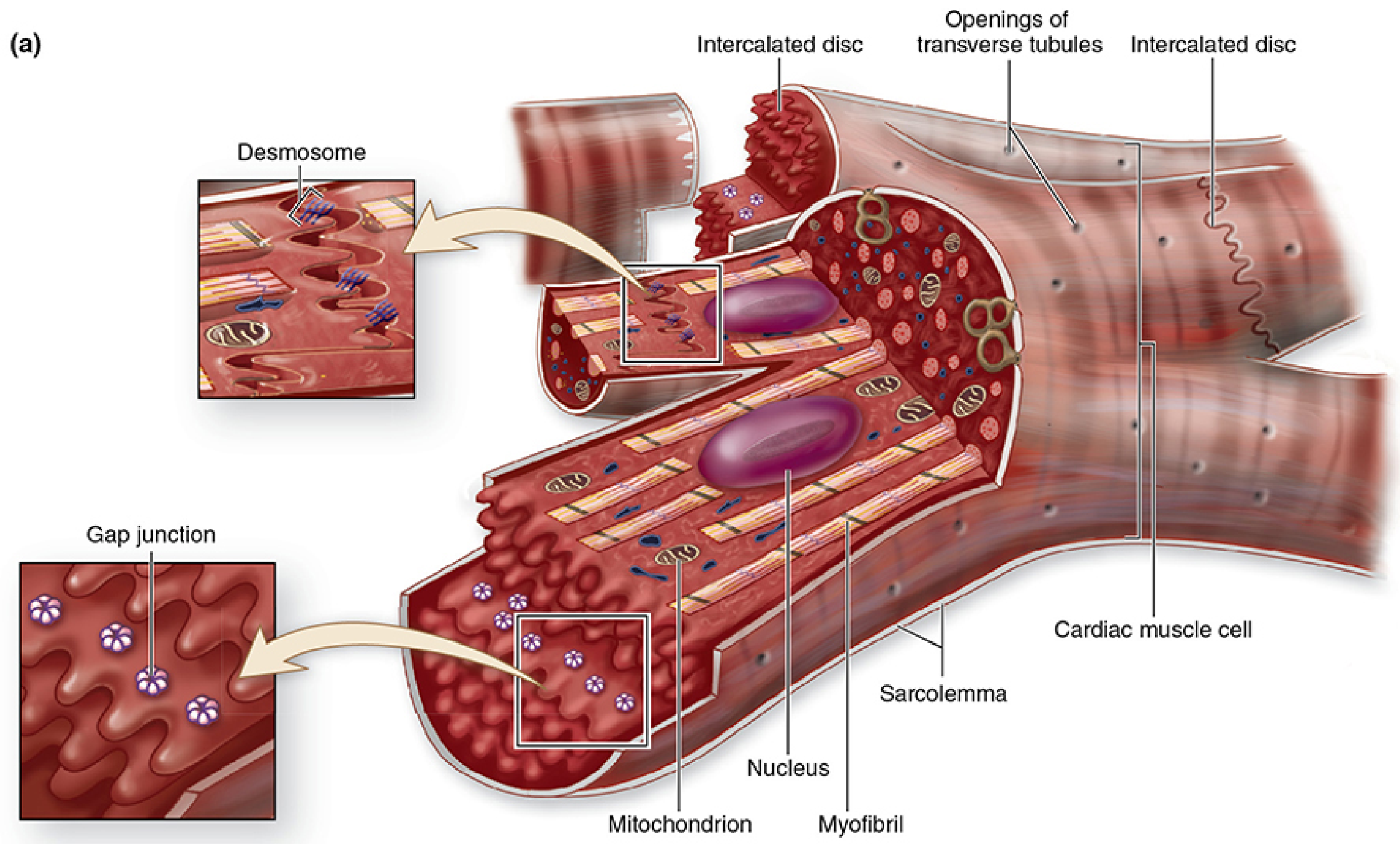
- Cardiac muscle fibres consist of numerous cylindrical cells arranged end-to-end, unlike skeletal muscle which is a single multinucleated cell
- Histology: A Text and Atlas (Ross & Pawlina)
- Each cardiac muscle cell has a single, centrally placed nucleus (occasionally two)
- This is a key distinguishing feature from skeletal muscle, where multiple nuclei lie peripherally just beneath the sarcolemma
- The myofibrils separate to pass around the nucleus, forming a biconical juxtanuclear region rich in mitochondria, Golgi apparatus, lipofuscin granules, and glycogen
- Histology: A Text and Atlas
- Cardiac muscle is striated in the same manner as skeletal muscle, with typical myofibrils containing actin and myosin filaments arranged in A bands, I bands, H zones, and Z lines
- Each sarcomere (Z line to Z line) contains thick filaments (myosin) and thin filaments (actin + tropomyosin + troponin)
- Troponin C binds Ca²⁺; tropomyosin blocks myosin-binding sites when Ca²⁺ is absent
- Costanzo Physiology, 7e
- The most distinctive histological feature of cardiac muscle
- They appear as densely staining transverse bands crossing fibres in a linear or staircase (step-like) pattern in light microscopy
- Represent specialised cell-to-cell junctions between adjacent cardiac myocytes
| Component | Location in Disc | Junctions Present | Function |
|---|---|---|---|
| Transverse (T) portion | Perpendicular to myofibrils | Fascia adherens + Desmosomes | Mechanical coupling - transmits contractile force |
| Lateral (L) portion | Parallel to myofibrils | Gap junctions (connexons) | Electrical coupling - ion diffusion |
- Fascia adherens: anchors actin filaments of the terminal sarcomere; analogous to the Z line
- Desmosomes (maculae adherentes): provide firm mechanical attachment; prevent pulling apart of cells during contraction
- Gap junctions: allow rapid ionic diffusion between cells; electrical resistance is extremely low, making cardiac muscle a functional syncytium
- Located at the Z line level in cardiac muscle (unlike skeletal muscle where they are at the A-I junction)
- Diameter is approximately 5 times greater than in skeletal muscle (volume 25 times greater)
- Open directly into the extracellular space, allowing extracellular Ca²⁺ to enter and be stored inside tubules
- Lined with mucopolysaccharides that are electronegatively charged and bind Ca²⁺
- Form dyads with the sarcoplasmic reticulum (not triads as in skeletal muscle)
- Guyton and Hall; Histology: A Text and Atlas
- Less well developed than in skeletal muscle
- Forms a dyadic structure with T-tubules (one SR terminal cisterna + one T-tubule)
- Contains ryanodine receptors (RyR2/Ca²⁺ release channels) on its membrane
- Stores Ca²⁺ that is released upon excitation
- Costanzo Physiology, 7e
- Extraordinarily abundant - occupy 25-35% of the cell volume
- Large mitochondria are densely packed between myofibrils, often extending the full length of a sarcomere, with closely packed cristae
- This reflects the heart's absolute dependence on aerobic metabolism (cardiac muscle is almost exclusively aerobic)
- Histology: A Text and Atlas
- Atrial cells contain specific secretory granules (0.3-0.4 μm) in the juxtanuclear cytoplasm
- Contain Atrial Natriuretic Factor (ANF) and Brain Natriuretic Factor (BNF)
- Both are diuretic hormones; inhibit renin and aldosterone secretion, and relax vascular smooth muscle
- BNF levels rise markedly in congestive heart failure (clinical marker)
- Histology: A Text and Atlas
II. PROPERTIES OF CARDIAC MUSCLE
1. Syncytial Property (Functional Syncytium)
- Because gap junctions at intercalated discs allow free ionic flow, the cardiac muscle acts as a functional syncytium
- Two syncytia exist: the atrial syncytium and the ventricular syncytium, separated by the fibrous skeleton of the heart (which electrically insulates them except at the AV bundle)
- When any part is stimulated, the action potential spreads through the entire syncytium → the heart contracts as one unit ("all-or-none" principle)
- Guyton and Hall
2. Rhythmicity (Automaticity)
- Cardiac muscle possesses inherent automaticity - it can generate action potentials spontaneously without external neural input
- Pacemaker cells (SA node) exhibit spontaneous phase 4 depolarisation due to the funny current (I_f) and generate rhythmic action potentials that drive the entire heart
3. Prolonged Action Potential and Refractory Period
- The cardiac action potential averages ~105 mV (resting: -85 mV → peak: +20 mV)
- It has a characteristic plateau lasting ~0.2-0.3 seconds, caused by:
- Opening of L-type Ca²⁺ channels (slow calcium channels) - remain open for several tenths of a second
- Reduced K⁺ permeability (K⁺ channels close during the plateau, unlike skeletal muscle)
- The long plateau makes ventricular contraction last 15 times longer than a skeletal muscle twitch
- The prolonged refractory period (lasting nearly the entire duration of contraction) prevents tetanic contraction - vital for the heart to relax and fill between beats
- Guyton and Hall
4. All-or-None Law
- A single cardiac muscle cell either contracts maximally or not at all; there is no partial contraction in response to sub-threshold stimuli
5. Frank-Starling Mechanism
- Within physiological limits, the force of contraction increases with the initial length of the muscle fibre (preload). Stretching of cardiac muscle increases sensitivity of troponin C to Ca²⁺ and increases cross-bridge formation.
6. Dependence on Extracellular Ca²⁺
- Unlike skeletal muscle (which relies almost entirely on intracellular SR calcium), cardiac muscle is critically dependent on extracellular Ca²⁺
- A heart placed in a calcium-free solution stops beating within ~1 minute
- Ca²⁺ enters through T-tubule L-type channels during the action potential plateau to trigger SR Ca²⁺ release
- Guyton and Hall; Harper's Illustrated Biochemistry, 32e
III. MECHANISM OF CARDIAC MUSCLE CONTRACTION
A. The Contractile Proteins
- Thick filaments: composed of myosin; globular heads have actin-binding sites and ATPase activity
- Thin filaments: three proteins - actin (two twisted strands with myosin-binding site), tropomyosin (runs along the actin groove and blocks myosin-binding site at rest), and troponin complex (troponin T - binds tropomyosin; troponin I - inhibits actin-myosin interaction; troponin C - binds Ca²⁺)
- Costanzo Physiology, 7e
B. Excitation-Contraction Coupling
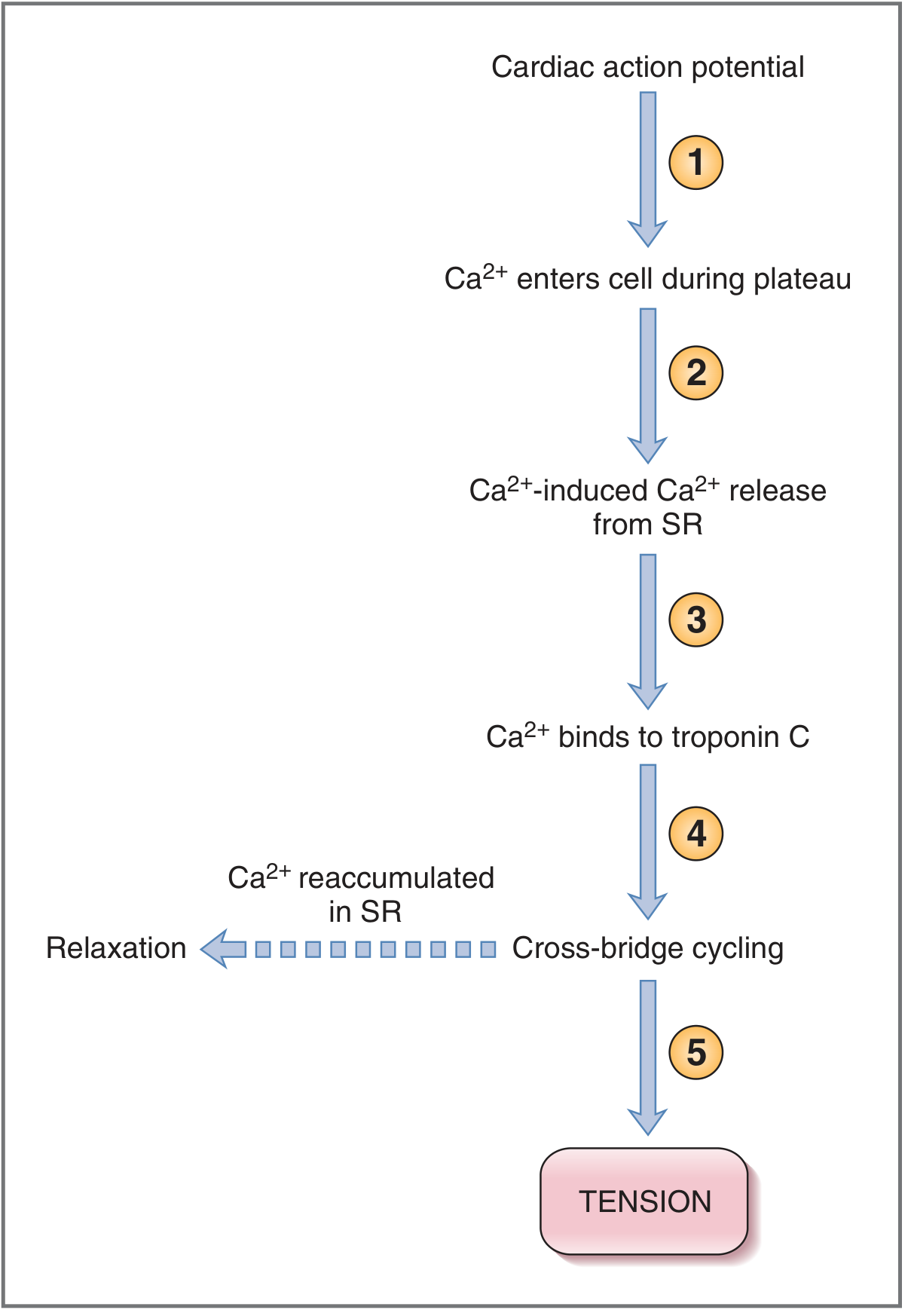
- A cardiac action potential is initiated at the SA node and spreads across the sarcolemma
- Depolarisation travels into the cell interior via the T-tubules
- During phase 2 (plateau) of the action potential, L-type Ca²⁺ channels (dihydropyridine receptors, DHPRs) open, allowing Ca²⁺ to flow from extracellular fluid (ECF) into the cytoplasm (ICF)
- The Ca²⁺ entering through L-type channels acts as a "trigger Ca²⁺" - this small amount of Ca²⁺ alone is insufficient to initiate contraction
- It binds to ryanodine receptors (RyR2) on the SR membrane, triggering the release of a much larger amount of Ca²⁺ from SR stores
- This amplification mechanism is called Ca²⁺-induced Ca²⁺ release (CICR)
- The magnitude of Ca²⁺ release depends on: (a) amount of Ca²⁺ stored in SR and (b) the size of the inward Ca²⁺ current during the plateau
- Costanzo Physiology, 7e
- Intracellular Ca²⁺ concentration rises from ~0.1 μmol/L (resting) to ~1-10 μmol/L
- Ca²⁺ binds to troponin C (TnC), causing a conformational change in the troponin-tropomyosin complex
- Tropomyosin moves out of the myosin-binding groove on actin, exposing the active sites on actin
- Myosin heads bind to the exposed actin active sites, forming cross-bridges
- ATP hydrolysis drives a power stroke - the myosin head pivots, pulling the thin filament toward the centre of the sarcomere
- ADP + Pi are released; a new ATP binds to myosin, causing detachment of the cross-bridge
- The cycle repeats as long as Ca²⁺ occupies TnC binding sites → the Z lines move closer together → the sarcomere shortens → the entire cell shortens
- The magnitude of tension produced is directly proportional to the intracellular Ca²⁺ concentration
- This is why positive inotropes (e.g., digoxin, catecholamines) and negative inotropes (e.g., beta-blockers, Ca²⁺ channel blockers) act by altering intracellular Ca²⁺
C. Relaxation
| Mechanism | Location | Energy Source |
|---|---|---|
| SERCA2 pump (SR Ca²⁺-ATPase) | SR membrane | ATP (direct) |
| Sarcolemmal Ca²⁺-ATPase | Cell membrane | ATP (direct) |
| Na⁺-Ca²⁺ exchanger (NCX) | Cell membrane | Na⁺ gradient (indirect - ultimately Na⁺/K⁺-ATPase) |
- Ca²⁺ is reaccumulated into the SR via SERCA2 and extruded from the cell via sarcolemmal Ca²⁺-ATPase and NCX
- As Ca²⁺ falls, it dissociates from troponin C, tropomyosin returns to block actin, cross-bridge cycling stops, and the muscle relaxes
- Guyton and Hall; Costanzo Physiology, 7e
Summary Table: Cardiac Muscle vs. Skeletal Muscle
| Feature | Cardiac Muscle | Skeletal Muscle |
|---|---|---|
| Cell type | Uninucleate, branched cells in series | Multinucleate syncytium |
| Nucleus position | Central | Peripheral (subsarcolemmal) |
| T-tubule position | Z line | A-I junction |
| T-tubule diameter | 5× larger | Standard |
| SR development | Less developed | Well developed |
| Cell junctions | Intercalated discs | Absent |
| Ca²⁺ source for contraction | Extracellular + SR (CICR) | Almost entirely SR |
| Action potential plateau | Present (~0.2-0.3 s) | Absent |
| Contraction type | Cannot tetanise | Can tetanise |
| Mitochondria | 25-35% cell volume | Less abundant |
| Control | Autonomous (autorhythmic) | Voluntary (neural) |
- Guyton and Hall Textbook of Medical Physiology (Guyton & Hall, 14e)
- Costanzo Physiology, 7th Edition
- Junqueira's Basic Histology: Text and Atlas, 17e
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Ross & Pawlina)
- Harper's Illustrated Biochemistry, 32e
Can u make a flow chat of mechanism of contraction of cardiac muscle
A detailed medical flowchart titled "Mechanism of Cardiac Muscle Contraction" showing the following sequential steps with arrows connecting each box: 1. "Action Potential initiated at SA Node" → spreads along sarcolemma 2. "Depolarisation travels down T-Tubules (L-type Ca²⁺ channels / DHPRs open)" 3. "Small amount of Ca²⁺ enters from ECF (Trigger Ca²⁺)" 4. "Trigger Ca²⁺ activates Ryanodine Receptors (RyR2) on Sarcoplasmic Reticulum (SR)" 5. "Ca²⁺-Induced Ca²⁺ Release (CICR) — Large Ca²⁺ release from SR" 6. "Intracellular [Ca²⁺] rises (0.1 → 10 µmol/L)" 7. "Ca²⁺ binds Troponin C (TnC)" → "Conformational change in Troponin-Tropomyosin complex" 8. "Tropomyosin shifts — Active sites on Actin EXPOSED" 9. "Myosin heads bind Actin → Cross-bridges form" 10. "ATP hydrolysis → Power Stroke (myosin head pivots)" 11. "Thin filaments slide toward M-line → Sarcomere shortens" 12. "TENSION / CONTRACTION" Then a separate RELAXATION branch showing: - "Ca²⁺ removed by: SERCA2 pump (SR) + Sarcolemmal Ca²⁺-ATPase + Na⁺-Ca²⁺ Exchanger (NCX)" - "Intracellular [Ca²⁺] falls" - "Ca²⁺ dissociates from Troponin C" - "Tropomyosin blocks actin active sites" - "Cross-bridges detach → RELAXATION" Clean professional medical diagram style with blue and white color scheme, clear bold text labels, rounded boxes, and directional arrows. Include a small note box: "Tension ∝ Intracellular [Ca²⁺]"
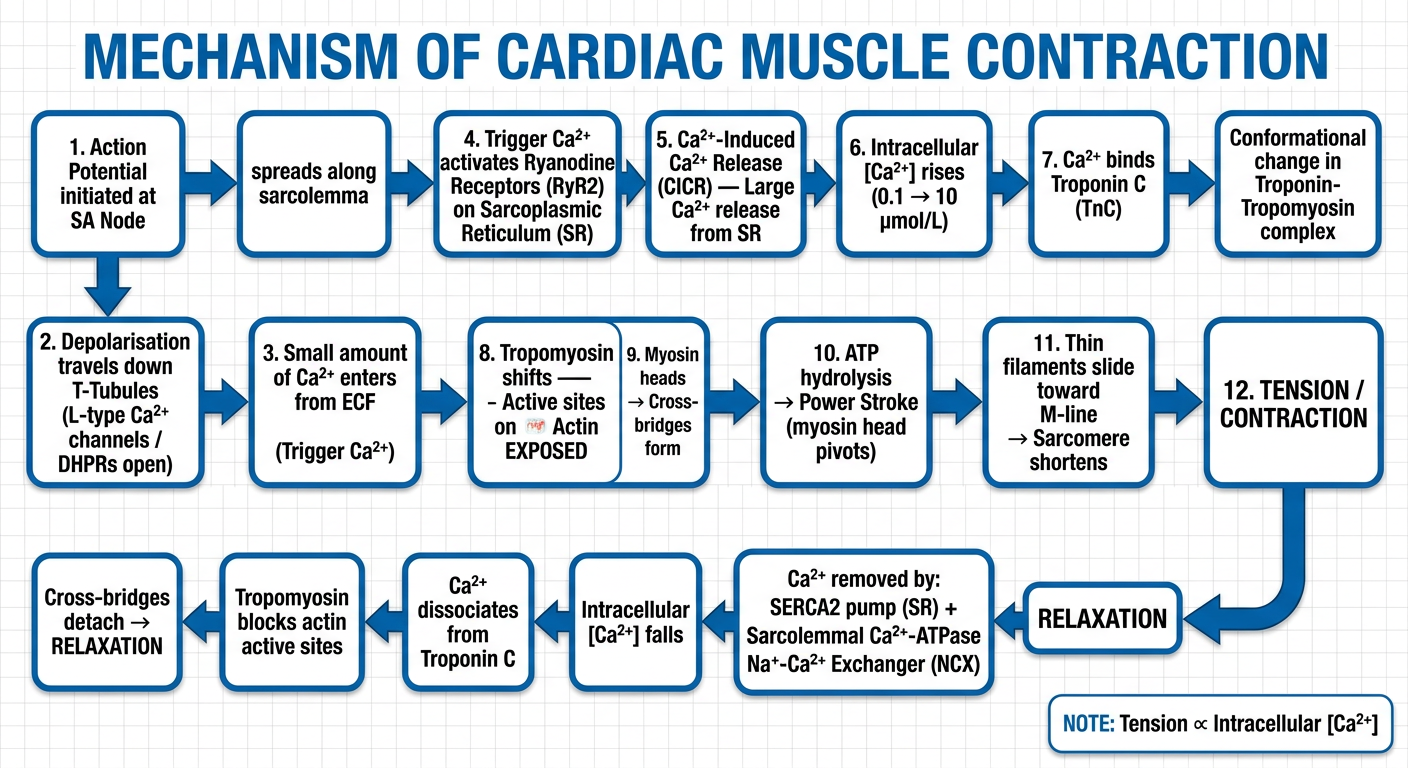
- Action potential at SA node → spreads along sarcolemma
- Depolarisation travels down T-tubules → L-type Ca²⁺ channels (DHPRs) open
- Trigger Ca²⁺ enters from ECF
- Trigger Ca²⁺ activates ryanodine receptors (RyR2) on the SR
- Ca²⁺-induced Ca²⁺ release (CICR) - large Ca²⁺ floods cytoplasm
- Ca²⁺ binds Troponin C → tropomyosin shifts → actin active sites exposed
- Myosin cross-bridges form → power stroke (ATP) → sarcomere shortens → TENSION
- Ca²⁺ pumped back by SERCA2 (into SR), sarcolemmal Ca²⁺-ATPase, and Na⁺-Ca²⁺ exchanger (NCX)
- Ca²⁺ dissociates from TnC → tropomyosin re-blocks actin → cross-bridges detach → RELAXATION