Bronchial Asthma Causes Signs & Symptoms Investigations Medical Management Nursing Management Health Education
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Marathi aani english mix krun de
🫁 Bronchial Asthma (श्वासनलिका दमा)
1. CAUSES (कारणे)
Asthma हा एक chronic inflammatory airway disease आहे. त्याची कारणे दोन प्रकारची असतात:
A) Atopic Asthma (Allergic) - IgE-mediated
- Environmental allergens - धूळ (dust), परागकण (pollens), cockroach dander, animal fur, foods
- Positive family history असतो
- Skin test मध्ये wheal-and-flare reaction येते
- Serum IgE level elevated असतो
B) Non-Atopic Asthma
- Skin test negative असतो
- Viral infections trigger करतात - rhinovirus, parainfluenza, RSV
- Air pollutants - tobacco smoke, sulfur dioxide, ozone, nitrogen dioxide
C) Drug-Induced Asthma
- Aspirin आणि NSAIDs - cyclooxygenase pathway inhibit करतात → prostaglandin E2 कमी होतो → leukotrienes वाढतात → bronchospasm
- Nasal polyps + recurrent rhinitis सोबत येतो
D) Occupational Asthma
- Fumes (epoxy resins, plastics), organic dusts (wood, cotton), gases (toluene), chemicals (formaldehyde, penicillin products)
- Repeated exposure नंतर attack येतो
E) Other Triggers
- Cold air, exercise
- GERD (gastroesophageal reflux)
- Emotional stress, anxiety
- Strong odors, paint, perfumes
2. PATHOPHYSIOLOGY (रोगाची प्रक्रिया)
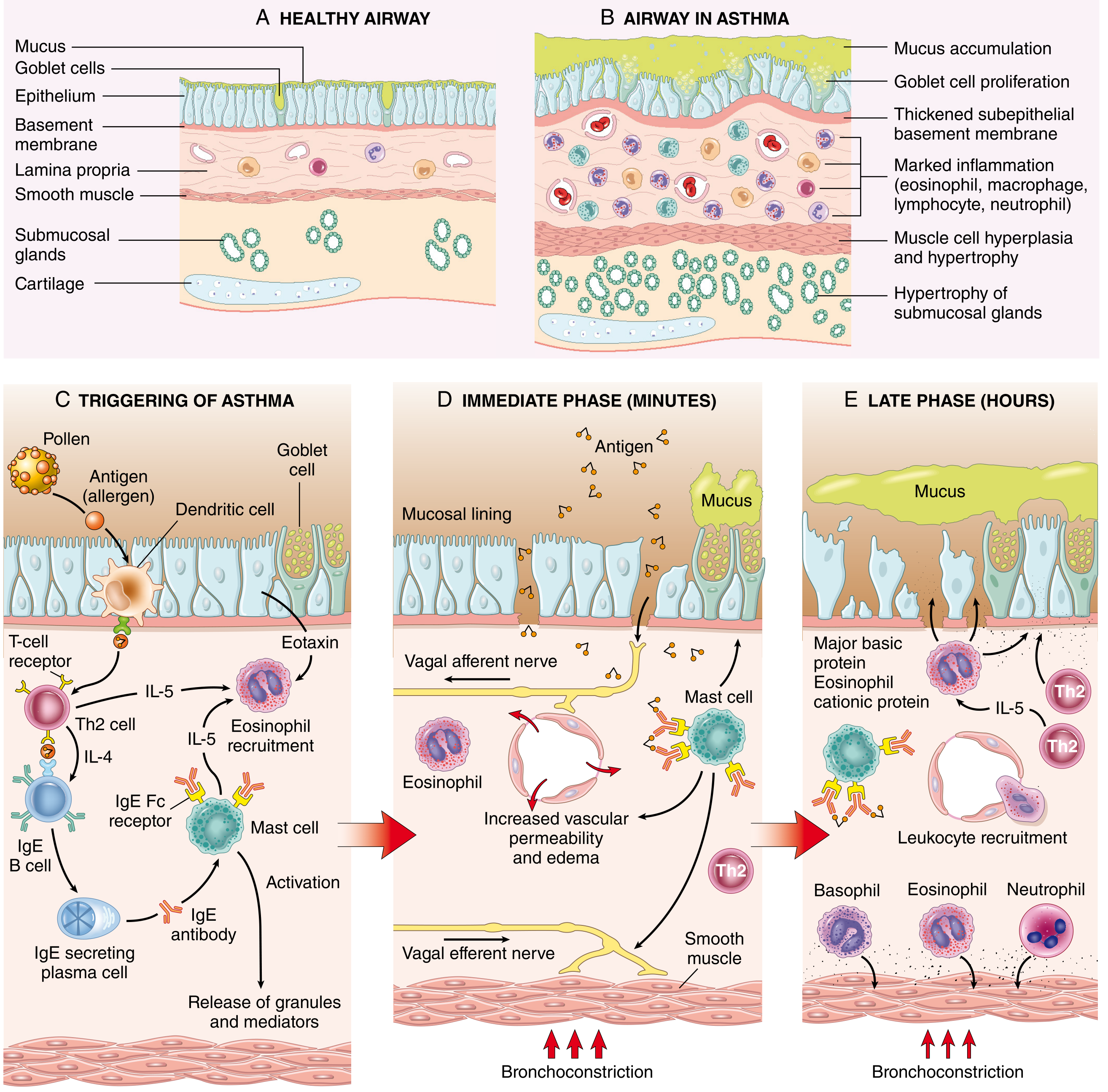
Healthy airway vs Asthmatic airway — Th2 response, IgE, mast cell activation, immediate आणि late phase reaction
Mechanism थोडक्यात:
- Allergen शरीरात शिरतो → Dendritic cells antigen present करतात → Th2 cells activate होतात
- Th2 cells cytokines सोडतात:
- IL-4 → IgE production stimulate करतो
- IL-5 → Eosinophils activate करतो
- IL-13 → Mucus secretion वाढवतो
- IgE → Mast cells वर बसतो → Re-exposure मध्ये mast cell degranulation होते
- Early phase (minutes): Bronchoconstriction + mucus + vascular permeability वाढते
- Late phase (hours): Eosinophils, neutrophils, basophils recruit होतात → epithelial damage → airway remodeling
Airway मध्ये बदल:
- Mucus accumulation (goblet cell proliferation)
- Thickened basement membrane
- Smooth muscle hyperplasia & hypertrophy
- Submucosal gland hypertrophy
- Marked inflammation (eosinophils, macrophages, lymphocytes)
3. SIGNS & SYMPTOMS (चिन्हे आणि लक्षणे)
Symptoms (रुग्णाला काय होतं):
| Symptom | वर्णन |
|---|---|
| Dyspnea | श्वास घेण्यास त्रास, विशेषतः exertion मध्ये |
| Wheezing | श्वास घेताना "seet-seet" असा आवाज |
| Cough | कोरडा खोकला, रात्री जास्त |
| Chest tightness | छातीत घट्टपणा |
| Sputum production | जाड, चिकट कफ |
Signs (तपासणीत दिसते):
- Tachypnea - श्वसनाचा वेग वाढलेला
- Tachycardia - हृदयाचा ठोका जलद
- Accessory muscle use - मानेचे, खांद्याचे स्नायू श्वासासाठी वापरणे
- Prolonged expiration - उच्छवास लांब होतो
- Hyperinflation - छाती barrel-shaped दिसते (chronic cases)
- Cyanosis - severe cases मध्ये ओठ/बोटे निळे पडतात
- Pulsus paradoxus - severe attack मध्ये
- Silent chest - अत्यंत severe obstruction मध्ये wheezing बंद होतो (धोक्याचे लक्षण!)
Severity Classification:
| Severity | Symptoms | PEF/FEV1 |
|---|---|---|
| Mild | Activity मध्येच dyspnea | ≥70% predicted |
| Moderate | Daily activities limit होतात | 40–69% predicted |
| Severe | Rest मध्येही dyspnea, बोलता येत नाही | <40% predicted |
| Life-threatening | बोलणे अशक्य, घाम येतो | <25% predicted |
4. INVESTIGATIONS (तपासण्या)
A) Pulmonary Function Tests (PFTs)
-
Spirometry - सर्वात महत्त्वाची तपासणी
- FEV1 कमी असतो
- FVC कमी असतो
- FEV1/FVC ratio कमी (<70%) → obstructive pattern
- Bronchodilator दिल्यावर FEV1 ≥12% आणि ≥200 mL ने वाढल्यास → reversible obstruction → asthma confirmed
-
Peak Expiratory Flow Rate (PEFR)
- Peak flow meter वापरून घरी measure करता येते
- Morning आणि evening PEFR मध्ये >20% variation → asthma suggest करतो
B) Arterial Blood Gas (ABG)
- Mild/moderate: PaO2 कमी, PaCO2 कमी (hyperventilation)
- Severe/life-threatening: PaCO2 normal किंवा वाढलेला → ventilatory failure चा धोका
C) Chest X-Ray
- Acute attack मध्ये hyperinflation दिसते
- Pneumothorax, pneumonia rule out करण्यासाठी
D) Pulse Oximetry (SpO2)
- Continuous monitoring साठी
- SpO2 <92% → severe attack
E) Blood Tests
- CBC - Eosinophilia (>4%) दिसते
- Serum IgE - Atopic asthma मध्ये elevated
- Allergen-specific IgE (RAST test) - कोणत्या allergen ला sensitive आहे ते ओळखण्यासाठी
F) Sputum Examination
- Eosinophils, Curschmann spirals, Charcot-Leyden crystals दिसतात
G) FeNO (Fraction of Exhaled Nitric Oxide)
- Eosinophilic airway inflammation चा biomarker
- Elevated FeNO → ICS ला चांगला response मिळतो
H) Skin Prick Test
- Specific allergens ओळखण्यासाठी
- Atopic asthma diagnosis मध्ये उपयुक्त
5. MEDICAL MANAGEMENT (वैद्यकीय उपचार)
GINA Step Therapy (पायरी पायरी उपचार):
| Step | Treatment |
|---|---|
| Step 1 (Mild intermittent) | SABA as needed (Salbutamol/Albuterol inhaler) |
| Step 2 (Mild persistent) | Low-dose ICS + SABA as needed |
| Step 3 (Moderate) | Low-medium dose ICS + LABA |
| Step 4 (Severe) | Medium-high dose ICS + LABA ± LAMA |
| Step 5 (Very severe) | High-dose ICS + LABA + add-on biologics (e.g., Omalizumab) |
A) Bronchodilators (श्वासनलिका उघडणारी औषधे)
1. Short-Acting β2 Agonists (SABA) - Rescue inhaler
- Salbutamol (Albuterol) - सर्वात जास्त वापरली जाते
- MDI (metered-dose inhaler) किंवा nebulizer द्वारे
- 2–6 puffs दर 4 तासांनी (acute attack मध्ये दर 15-20 min)
- Side effects: tachycardia, tremors, hypokalemia
2. Long-Acting β2 Agonists (LABA) - Maintenance
- Salmeterol, Formoterol - 12 तास effect
- ICS सोबतच वापरतात, एकट्याने नाही
- Acute attack साठी नाही
3. Anticholinergics
- Ipratropium bromide (SAMA) - acute severe asthma मध्ये SABA सोबत
- Tiotropium (LAMA) - Step 4-5 मध्ये add-on therapy
B) Corticosteroids (दाह कमी करणारी औषधे)
1. Inhaled Corticosteroids (ICS) - First-line controller
- Budesonide, Fluticasone, Beclomethasone
- Airway inflammation कमी करतो
- Use नंतर तोंड धुणे आवश्यक (oral candidiasis टाळण्यासाठी)
2. Systemic Corticosteroids
- Acute severe attack मध्ये
- IV Methylprednisolone 1 mg/kg किंवा Oral Prednisone 40–60 mg
- 5–10 दिवसांचा course (tapering नाही)
- Peak effect 4–8 तासांनंतर
C) Leukotriene Receptor Antagonists
- Montelukast - mild persistent asthma मध्ये, aspirin-induced asthma मध्ये उपयुक्त
D) Oxygen Therapy
- SpO2 ≥94–95% ठेवण्यासाठी
- Nasal cannula किंवा mask द्वारे
E) Magnesium Sulfate (Status Asthmaticus मध्ये)
- IV MgSO4 1–2 grams over 30 minutes
- Smooth muscle relax करतो → bronchodilation
- FEV1/PEFR <25% असल्यास द्यावे
F) Biologics (Severe Asthma साठी)
- Omalizumab - Anti-IgE (allergic asthma)
- Mepolizumab, Benralizumab - Anti-IL-5 (eosinophilic asthma)
6. NURSING MANAGEMENT (परिचर्या व्यवस्थापन)
A) Assessment (मूल्यांकन)
- Respiratory rate, depth, rhythm नोंद करणे
- SpO2 monitor करणे
- Breath sounds auscultate करणे (wheeze, silent chest)
- Level of consciousness check करणे
- Pulsus paradoxus तपासणे
- Peak flow measurement करणे
B) Positioning (स्थिती)
- रुग्णाला high Fowler's position (90°) किंवा orthopneic position मध्ये ठेवणे
- Breathing सोपे व्हावे म्हणून पुढे वाकून बसण्यास मदत करणे
C) Airway Management
- Airway patent ठेवणे
- Oxygen prescribed प्रमाणे देणे (target SpO2 ≥94%)
- Nebulizer treatments वेळेवर देणे
- Secretions loose करण्यासाठी adequate hydration
- Suction available ठेवणे
D) Medication Administration
- Inhaled medications योग्य technique ने देणे
- MDI वापरताना spacer वापरणे
- ICS नंतर तोंड धुवायला सांगणे
- IV medications prescribed rate ने देणे
- Side effects monitor करणे (tremors, tachycardia, hyperglycemia)
E) Fluid Management
- Adequate oral/IV hydration देणे (secretions thin करण्यासाठी)
- I/O chart maintain करणे
F) Monitoring
- Vital signs दर 15-30 min (acute attack मध्ये)
- SpO2 continuous
- ABG values interpret करणे
- Peak flow नोंद ठेवणे
- Signs of respiratory failure: agitation, cyanosis, silent chest, altered consciousness
G) Psychological Support
- रुग्णाला शांत ठेवणे, anxiety कमी करणे
- Calm, reassuring presence ठेवणे (anxiety → attack worse करतो)
- Simple language मध्ये procedures समजावणे
H) Emergency Preparedness
- Emergency cart nearby ठेवणे
- Intubation equipment तयार ठेवणे
- Doctor ला वेळेत call करणे - deterioration, silent chest, altered sensorium
7. HEALTH EDUCATION (आरोग्य शिक्षण)
A) Trigger Avoidance (कारणे टाळणे)
- धूळ (dust mites) पासून बचाव - mattress covers वापरणे, नियमित bedding wash करणे
- पाळीव प्राण्यांपासून दूर राहणे
- धूम्रपान (smoking) पूर्णपणे बंद करणे - active आणि passive दोन्ही
- थंड हवा टाळणे, बाहेर जाताना तोंडावर मास्क वापरणे
- Strong perfumes, chemical fumes, paint टाळणे
- NSAID/Aspirin - doctor च्या सल्ल्याशिवाय घेऊ नका
B) Inhaler Technique (योग्य inhaler वापरणे)
- MDI वापरण्याची step-by-step technique शिकवणे:
- Inhaler shake करा
- Deep breath बाहेर सोडा
- Mouthpiece तोंडात घ्या, spacer वापरा
- हळू दीर्घ श्वास घेताना puff दाबा
- 10 seconds breath hold करा
- ICS नंतर तोंड धुवा
- Demonstration करून दाखवणे आणि रुग्णाकडून return demonstration घेणे
C) Peak Flow Monitoring
- घरी peak flow meter वापरण्यास शिकवणे
- Green zone (≥80% personal best) - normal, continue medications
- Yellow zone (50–79%) - caution, reliever घ्या, doctor ला call करा
- Red zone (<50%) - Emergency! तातडीने hospital मध्ये जा
D) Asthma Action Plan
- Written action plan देणे
- कोणती symptoms आल्यास काय करायचे हे लिहून देणे
- Emergency contact numbers देणे
E) Medication Compliance
- Prescribed medications नियमित घेणे, symptoms नसले तरी
- ICS "symptoms नाहीत म्हणून बंद करू नका" हे समजावणे
- Rescue inhaler नेहमी जवळ ठेवणे
F) Lifestyle Modifications
- Regular mild exercise - swimming (warm water) चांगले असते, पण warm-up आवश्यक
- Exercise आधी SABA घेण्याची सवय (exercise-induced bronchospasm टाळण्यासाठी)
- Balanced diet - fruits, vegetables, omega-3 fatty acids
- Obesity असल्यास weight loss - asthma control सुधारतो
- Stress management - yoga, breathing exercises (Pranayama)
- Adequate sleep घेणे
G) Regular Follow-up
- Doctor कडे नियमित follow-up - दर 3-6 months
- Spirometry वर्षातून एकदा
- Vaccination - Influenza vaccine वर्षातून एकदा, Pneumococcal vaccine घेणे
- Symptoms diary maintain करणे
H) Warning Signs (धोक्याची चिन्हे)
खालील लक्षणे आल्यास तातडीने hospital मध्ये जा:
- Reliever inhaler ने relief नाही
- बोलता येत नाही
- ओठ/बोटे निळे पडले
- Chest मध्ये wheeze बंद झाला (silent chest)
- Confusion, drowsiness
- SpO2 <90%
Sources: Robbins Cotran & Kumar - Pathologic Basis of Disease | Tintinalli's Emergency Medicine | Murray & Nadel's Textbook of Respiratory Medicine | Goldman-Cecil Medicine
Child health nursing gnm 2nd years ch aahe question aahe ha
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the content needed. Let me compile the comprehensive pediatric asthma notes in Marathi-English mix format.
🫁 Bronchial Asthma in Children
(GNM 2nd Year - Child Health Nursing | Long Answer Notes)
DEFINITION (व्याख्या)
Bronchial Asthma म्हणजे lower airway चा chronic inflammatory disease आहे, ज्यामध्ये bronchoconstriction, mucosal edema, आणि pulmonary secretions यांमुळे reversible airway obstruction होते.
- मुलांमध्ये 1 in 12 children ला asthma असतो
- Non-Hispanic black children मध्ये prevalence 16% पर्यंत असतो
- 17% मुलांना ED/Urgent care लागते, 5% ला hospitalization लागते
CAUSES / ETIOLOGY (कारणे)
1. Atopic (Allergic) Causes - सर्वात सामान्य
- Inhalant allergens - धूळ (house dust mites), animal dander (मांजर, कुत्रा), cockroach, pollens
- Food allergens - milk, egg, peanuts, wheat (लहान मुलांमध्ये जास्त)
- Positive family history - एक parent असल्यास मुलाला 25% risk, दोन्ही parents असल्यास आणखी जास्त
2. Infections (संक्रमण) - मुलांमध्ये सर्वात सामान्य trigger
- Upper Respiratory Infections (URI) - rhinovirus, RSV, parainfluenza virus
- Viral bronchiolitis नंतर asthma develop होण्याचा धोका वाढतो
3. Environmental Triggers (पर्यावरणीय कारणे)
- Passive smoking - घरात कोणी धूम्रपान करत असल्यास
- Air pollutants - dust, smoke, chemical fumes
- Strong odors - paint, perfume, cleaning agents
- Cold air, exercise - विशेषतः थंड हवामानात खेळणे
4. Non-Allergic Causes
- Exercise-induced bronchospasm (खेळताना attack)
- Aspirin / NSAIDs - drug-induced
- Emotional stress, crying, laughing (लहान मुलांमध्ये)
- GERD (gastroesophageal reflux) - acid regurgitation triggers bronchospasm
5. Predisposing Factors (पूर्वस्थिती)
- Atopy (eczema + allergic rhinitis असलेल्या मुलांमध्ये जास्त)
- Prematurity / low birth weight
- Maternal smoking during pregnancy
- Early exposure to allergens
PATHOPHYSIOLOGY (रोगाची प्रक्रिया)
मुलांमध्ये विशेष:
मुलांची chest wall compliant (लवचिक) असते आणि ribs horizontal असतात, त्यामुळे thorax वापरून breathing करण्याची क्षमता कमी असते. त्यामुळे diaphragm वर जास्त अवलंबन असते.
- Allergen / Trigger → Th2 immune response activate होतो
- IgE production → Mast cells वर बसतो
- Re-exposure → Mast cell degranulation → Histamine, Leukotrienes सुटतात
- Early phase (minutes):
- Bronchoconstriction
- Mucosal edema
- Increased mucus secretion
- Late phase (hours):
- Eosinophils, Neutrophils, Lymphocytes येतात
- Airway wall remodeling
- Epithelial damage
Airway मध्ये होणारे बदल:
| बदल | परिणाम |
|---|---|
| Goblet cell proliferation | जास्त mucus |
| Thickened basement membrane | Airway narrow होते |
| Smooth muscle hyperplasia | Bronchoconstriction जास्त |
| Submucosal gland hypertrophy | Thick secretions |
| Eosinophil infiltration | Epithelial damage |
लहान मुलांमध्ये धोका का जास्त?
- Infant (<12 months) चा oxygen consumption adult च्या दुप्पट असतो
- Increased airway resistance + compliant chest → tachypnea, fatigue लवकर
- लवकर hypoxemia → bradycardia → cardiopulmonary arrest होण्याचा धोका
SIGNS & SYMPTOMS (चिन्हे आणि लक्षणे)
Symptoms (रुग्णाला होणारे त्रास):
- Wheezing - श्वास सोडताना "seet-seet" आवाज (सर्वात characteristic)
- Dyspnea - श्वास घेण्यास त्रास
- Cough - रात्री जास्त, कधी कधी dry, कधी productive
- Chest tightness - छातीत घट्टपणा (मोठ्या मुलांमध्ये सांगता येतो)
- Difficulty sleeping, eating, speaking - moderate/severe मध्ये
Signs (तपासणीत दिसतात):
सामान्य (Mild-Moderate):
- Tachypnea - श्वास जलद
- Tachycardia - हृदयाचा ठोका वाढलेला
- Expiratory wheezing (stethoscope वर ऐकू येते)
- Prolonged expiratory phase
गंभीर (Severe):
- Accessory muscle use - neck, intercostal, subcostal retractions
- Nasal flaring - नाकपुड्या फुगणे
- Subcostal/Intercostal retractions - श्वासाच्या वेळी छाती आत जाणे
- Cyanosis - ओठ/बोटे निळे पडणे
- Unable to speak full sentences
- Anxious, restless - hypoxia चे लक्षण
अत्यंत धोकादायक:
- Silent chest (wheezing बंद होणे - extreme obstruction)
- Altered mental status, lethargy
- SpO2 ≤92%
SEVERITY CLASSIFICATION (तीव्रतेचे प्रकार)
| Severity | Symptoms | SpO2 | Treatment |
|---|---|---|---|
| Mild | Wheezing, थोडा dyspnea, बोलता येते | >95% | SABA inhaler |
| Moderate | Retractions, बोलणे कठीण, tachypnea | 92-95% | SABA + Corticosteroids |
| Severe | Severe retractions, बोलता येत नाही, cyanosis | <92% | SABA + CS + O2 + Ipratropium |
| Life-threatening | Silent chest, drowsy, apnea | <90% | PICU, intubation |
INVESTIGATIONS (तपासण्या)
1. Pulse Oximetry (SpO2) - First & Most Important
- सर्व wheezing मुलांना लगेच लावावे
- SpO2 ≤92% → supplemental oxygen द्यावे
- "Fifth vital sign" म्हणून ओळखले जाते
2. Peak Expiratory Flow Rate (PEFR)
- 5 वर्षांपेक्षा कमी वयाच्या मुलांना करता येत नाही
-
5 वर्षांमध्ये: best of 3 attempts, child standing
- 2/3 मुलांना acute attack मध्ये PEFR करणे जड जाते
3. Chest X-Ray (CXR)
- Routine नाही - सर्व wheezing मुलांना CXR नको
- CXR कधी करावे:
- Choking history असल्यास (foreign body)
- Focal chest findings
- Extreme distress
- First time wheeze + asymmetric findings
- Cardiac cause suspected
4. Arterial Blood Gas (ABG)
- Routine नाही - severe cases मध्येच
- PaCO2 ≥40 mmHg + hypoxia = impending respiratory failure (धोकादायक!)
- अचानक "शांत" वाटणारे मूल → hypercarbia असू शकतो
5. Blood Tests
- CBC - Eosinophilia
- Serum IgE - Atopic asthma मध्ये elevated
- Allergen-specific IgE (RAST)
6. Spirometry (FEV1/FVC)
-
5-6 वर्षांच्या मुलांमध्ये करता येते
- Obstructive pattern: FEV1/FVC < 70%
- Post-bronchodilator FEV1 ≥12% वाढल्यास → reversible = asthma
7. Skin Prick Test
- Allergen identification साठी
- Stable state मध्ये करतात
MEDICAL MANAGEMENT (वैद्यकीय उपचार)
GINA Step Therapy (मुलांसाठी, 6-11 years):
| Step | Severity | Treatment |
|---|---|---|
| Step 1 | Intermittent | SABA as needed (Salbutamol) |
| Step 2 | Mild persistent | Low-dose ICS daily + SABA |
| Step 3 | Moderate | Low-medium ICS + LABA किंवा Montelukast |
| Step 4 | Severe | Medium-high ICS + LABA |
| Step 5 | Very severe | Specialist referral, biologics |
A) Short-Acting Beta-2 Agonists (SABA) - Rescue / First-line
Salbutamol (Albuterol) - मुलांसाठी drug of choice
- Nebulizer किंवा MDI + Spacer (MDI-S) द्वारे
- Acute attack मध्ये दर 20 minutes, पहिल्या 1 तासात 3 treatments
- MDI-S हे nebulizer इतकेच effective - सर्व वयांमध्ये
- Face mask spacer → लहान मुलांसाठी (mouthpiece वापरता येत नाही)
- Side effects: tachycardia, tremors, hypokalemia
⚠️ Levalbuterol racemic albuterol पेक्षा जास्त effective नाही आणि 5-25 पट महाग आहे - racemic albuterol च वापरावे
B) Corticosteroids (दाह कमी करण्यासाठी)
1. Inhaled Corticosteroids (ICS) - Controller therapy
- Budesonide, Fluticasone, Beclomethasone
- Persistent asthma मध्ये first-line maintenance
- ICS घेतल्यावर तोंड धुवावे (oral candidiasis टाळण्यासाठी)
- मुलांच्या growth वर mild effect - पण long-term benefit जास्त
2. Systemic Corticosteroids
- Moderate-severe attack मध्ये
- Oral Dexamethasone - मुलांमध्ये जास्त preferred
- Prednisone सारखेच effective, पण कमी doses, कमी vomiting, जास्त compliance
- Oral Prednisone - 1-2 mg/kg/day, max 40 mg, 3-5 days
- IV Methylprednisolone - severe/hospitalized मुलांसाठी
C) Anticholinergics
- Ipratropium Bromide (Atrovent) - moderate-severe attack मध्ये SABA सोबत
- Bronchodilation + mucus secretion कमी करतो
D) Oxygen Therapy
- SpO2 ≤92% असल्यास लगेच द्यावे
- Nasal cannula किंवा face mask
- Target: SpO2 ≥94%
E) IV Magnesium Sulfate
- Severe/life-threatening asthma मध्ये
- 25-75 mg/kg IV over 20-30 minutes
- Smooth muscle relax करतो
F) Leukotriene Receptor Antagonists
- Montelukast - mild persistent asthma मध्ये
- Aspirin-induced आणि exercise-induced asthma मध्ये विशेष उपयुक्त
- Oral tablet - compliance चांगली
NURSING MANAGEMENT (परिचर्या व्यवस्थापन)
A) Assessment (मूल्यांकन)
- Respiratory rate, depth, rhythm नोंद
- SpO2 monitor - सर्वप्रथम
- Breath sounds auscultate - wheeze, silent chest
- Mental status, alertness check
- Retractions, nasal flaring, cyanosis
- Asthma score (respiratory rate + wheezing + retractions + SpO2)
- Vital signs - dर 15-30 min (acute attack मध्ये)
B) Positioning (स्थिती)
- मोठ्या मुलांना High Fowler's position (90°) - breathing सोपे होते
- लहान मुलांना आईच्या मांडीवर upright ठेवणे
- Anxiety-provoking procedures (otoscopy, IV line) → SABA treatment सुरू झाल्यावरच करा
C) Airway & Breathing
- O2 prescribed प्रमाणे द्या (SpO2 ≤92% → तत्काळ O2)
- Nebulizer / MDI-S treatments वेळेवर द्या
- Secretions loose करण्यासाठी adequate fluids
- Suction available ठेवा
D) Medication Administration
- MDI + Spacer योग्य technique ने द्या
- लहान मुलांसाठी face mask spacer वापरा
- प्रत्येक puff नंतर मुलाने 5-8 श्वास घ्यावे
- ICS नंतर तोंड + face धुवा
- Dexamethasone/Prednisone - vomiting monitor करा
- IV medications prescribed rate ने द्या
- Side effects monitor - tachycardia, tremors, hyperglycemia
E) Monitoring - Deterioration साठी
खालील signs monitor करा - Doctor ला तत्काळ call करा:
- SpO2 कमी होणे (<92%)
- Silent chest
- Altered mental status / lethargy
- Cyanosis
- Respiratory fatigue signs
F) Fluid Management
- Oral hydration (mild cases) - secretions thin होतात
- IV fluids (severe/vomiting cases)
- I/O chart maintain करा
G) Psychological Support (मुलांसाठी विशेष महत्त्वाचे)
- मुलाला शांत करणे - रडणे / anxiety → attack worse करते
- पालकांनाही शांत ठेवणे (मुलांना पालकांची anxiety जाणवते)
- आई/बाबांना जवळ ठेवणे - separation anxiety कमी होते
- Simple words मध्ये मुलाला procedures explain करणे
- Distraction techniques - खेळणी, TV
H) Emergency Preparedness
- Emergency cart तयार ठेवणे
- Intubation equipment (child-size ET tube)
- Bag-valve mask (age-appropriate size)
- PICU team ला वेळेत alert करणे
HEALTH EDUCATION (आरोग्य शिक्षण) - पालकांना
A) Trigger Avoidance
- Passive smoking पूर्णपणे बंद - घरात, गाडीत कुठेही नाही
- Dust mites कमी करा - mattress covers, नियमित bedding wash (hot water)
- पाळीव प्राण्यांपासून मुलाला दूर ठेवा
- थंड हवेत खेळताना warm-up + SABA inhaler आधी
- Strong chemical odors, paint, spray टाळा
- Cockroach infestation control करा
B) Inhaler Technique (सर्वात महत्त्वाचे!)
MDI + Spacer technique - पालकांना शिकवा:
- Inhaler shake करा
- Spacer (face mask) मुलाच्या तोंड + नाकावर घट्ट लावा
- 1 puff spray करा
- मुल 5-8 श्वास घेऊ दे
- ICS असल्यास - face + तोंड पाण्याने धुवा
- Return demonstration घ्या!
C) Peak Flow Monitoring (5+ years)
- Green zone (≥80%) - Normal, regular medicines continue
- Yellow zone (50-79%) - Caution! Rescue inhaler द्या, doctor ला call करा
- Red zone (<50%) - Emergency! तातडीने hospital
D) Written Asthma Action Plan द्या
- लिखित plan - "हे symptoms आल्यास हे करा"
- Emergency contact numbers
- "कधी hospital ला जायचे" हे स्पष्टपणे सांगा
E) Medication Compliance
- "Symptoms नाहीत म्हणून ICS बंद करू नका" हे नीट समजावा
- Rescue inhaler मुलाच्या school bag मध्ये आणि घरी दोन्ही ठेवा
- Teacher ला/school ला सांगा - मुलाला asthma आहे
- Medicines वेळेवर refill करा
F) School & Activity
- Physical activity बंद करू नका - asthma control आल्यावर मुले खेळू शकतात
- Swimming (warm water) - asthmatic मुलांसाठी चांगले
- Exercise आधी SABA द्या (exercise-induced bronchospasm टाळण्यासाठी)
- School nurse / teacher ला written instructions द्या
G) Vaccination (लसीकरण)
- Influenza vaccine - वर्षातून एकदा (URI common trigger आहे)
- Pneumococcal vaccine - pneumonia prevent करण्यासाठी
H) Warning Signs - "तातडीने Hospital ला जा"
पालकांना हे लक्षात ठेवायला सांगा:
- Rescue inhaler देऊनही आराम नाही
- श्वास घेताना खूप जड वाटतेय, मूल बोलू शकत नाही
- ओठ / बोटे निळे पडले
- मूल खूप अस्वस्थ आहे किंवा झोपाळू झाले
- Chest मध्ये आवाज बंद झाला
- SpO2 <90%
DIFFERENTIAL DIAGNOSIS (वेगळे आजार)
| Condition | Asthma पेक्षा वेगळे कसे? |
|---|---|
| Bronchiolitis | Infant <2 years, first episode, viral URI, family history नाही |
| Croup | Inspiratory stridor, barky cough, fever |
| Foreign body | Choking history, toddler, unilateral wheeze |
| Pneumonia | Focal wheeze, rales, high fever, grunting |
| Cardiac failure | Murmur, hepatomegaly, rales, cardiomegaly on CXR |
| GERD | Wheezing after feeds, vomiting |
| Cystic fibrosis | Diarrhea, weight loss, salty sweat, chronic cough |
COMPLICATIONS (गुंतागुंत)
- Status Asthmaticus - Bronchodilator ने improve न होणारा severe attack
- Respiratory failure - Hypoxemia + Hypercapnia
- Pneumothorax - Air trapping मुळे
- Pneumomediastinum
- Growth retardation - Uncontrolled asthma मुळे
- School absenteeism - मुलांच्या शिक्षणावर परिणाम
NURSING DIAGNOSES (परिचर्या निदान)
- Ineffective airway clearance r/t bronchoconstriction, excess mucus
- Impaired gas exchange r/t airway obstruction
- Ineffective breathing pattern r/t bronchospasm
- Activity intolerance r/t dyspnea
- Anxiety (child + parents) r/t breathing difficulty
- Deficient knowledge (parents) r/t disease management, inhaler technique
Sources: Rosen's Emergency Medicine (Pediatric Asthma) | Robbins Cotran & Kumar - Pathologic Basis of Disease | Swanson's Family Medicine Review | Murray & Nadel's Textbook of Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.