MRI SWI Explanation
Reading File
Finding Sources
Searching the Web
MRI SWI susceptibility weighted imaging physics clinical applications
Reading File
Finding Sources
Reading Web Page
https://www.binasss.sa.cr/abril/39.pdf
Loading Image
Reading File
Here is a thorough explanation of MRI Susceptibility Weighted Imaging (SWI):
MRI Susceptibility Weighted Imaging (SWI)
What Is SWI?
SWI is a specialized MRI sequence that exploits magnetic susceptibility differences between tissues to create contrast. "Magnetic susceptibility" refers to how much a substance distorts the local magnetic field around it. When tissues contain compounds that are paramagnetic (strongly attracted to a magnetic field) or diamagnetic (weakly repelled), they cause local field inhomogeneities that SWI is uniquely sensitive to.
Physical Basis
The core principle is simple: substances like deoxygenated hemoglobin, blood breakdown products (hemosiderin, intracellular methemoglobin), iron deposits, and calcium all have different magnetic susceptibility compared to normal brain tissue. When placed in a magnetic field, they distort the local field around them, causing protons nearby to precess at slightly different frequencies. This dephasing reduces the net magnetization vector, producing signal loss (dark areas on the image).
Why GRE? Standard spin-echo sequences use a refocusing pulse that largely cancels out susceptibility effects. Gradient echo (GRE) sequences do NOT have this refocusing pulse, so susceptibility effects are preserved and amplified - making SWI exquisitely sensitive.
Technical implementation:
- 3D gradient echo acquisition with high spatial resolution
- Fully flow-compensated to minimize vascular dephasing from blood flow
- Uses both magnitude and phase images reconstructed separately, then combined
- Typical parameters: TR 25-50 ms, TE 20-40 ms, flip angle 15-20°
- Phase post-processing: a phase mask is applied to the magnitude image multiple times, further accentuating susceptibility differences
- Higher field strengths (3T, 7T) give stronger effects, allowing shorter TE and better signal-to-noise
What SWI Detects (and Why)
| Substance | Magnetic Property | Appearance on SWI |
|---|---|---|
| Deoxyhemoglobin | Paramagnetic | Dark (hypointense) |
| Intracellular methemoglobin | Paramagnetic | Dark |
| Hemosiderin | Paramagnetic | Dark |
| Iron deposits | Paramagnetic | Dark |
| Calcium | Diamagnetic | Dark (but phase image can differentiate) |
| Oxygenated blood | Diamagnetic (similar to brain) | Isointense |
| Veins (deoxygenated blood) | Paramagnetic | Dark, well-visualized |
A key advantage: the phase image can differentiate paramagnetic (iron, blood) from diamagnetic (calcium) substances - which look the same on the magnitude image but have opposite phase shifts. This helps distinguish hemorrhage from calcification.
Clinical Applications
1. Cerebral Microbleeds
SWI is the most sensitive sequence for detecting microbleeds - tiny foci of hemosiderin that appear as small dark "blooming" dots. This is clinically important in:
- Cerebral amyloid angiopathy (CAA) - lobar/cortical microbleeds
- Hypertensive small vessel disease - deep/basal ganglia microbleeds
- Traumatic brain injury / Diffuse axonal injury (DAI) - SWI detects 30% more lesions than CT and structural MRI combined in the ED
2. Trauma and Traumatic Brain Injury
SWI detects punctate hemorrhages (microhemorrhages) in deep subcortical white matter that are invisible on CT and standard MRI. The number and volume of SWI microhemorrhages correlates with clinical outcome and prognosis. It images the entire brain in ~4 minutes.
3. Stroke
- Detects intraluminal thrombus as linear hypointensity ("blooming") in vessels
- Identifies hemorrhagic transformation of ischemic infarcts
- Shows the "susceptibility vessel sign" - dark clot within an artery
4. Vascular Malformations
- Cavernomas appear as "popcorn" lesions with a dark hemosiderin rim - SWI shows many more lesions than T2
- AVMs - detects associated hemorrhage
- Developmental venous anomalies - venous structures are highlighted
5. Venous Imaging
Originally called "BOLD venography" (Blood Oxygen Level-Dependent), SWI shows small cortical and deep veins with excellent detail due to the paramagnetic deoxyhemoglobin in venous blood.
6. Brain Tumors
- Detects intratumoral microhemorrhages
- Venous architecture within tumors
- Helps grade gliomas (higher grade = more vessels/hemorrhage)
7. Neurodegenerative Diseases
Iron accumulates in specific brain regions in many neurodegenerative disorders, and SWI patterns are now part of diagnostic criteria for several conditions:
- Parkinson's disease - iron in substantia nigra
- Neurodegeneration with Brain Iron Accumulation (NBIA)
- Multiple sclerosis - iron rim around chronic active plaques
- Huntington's disease
- Chronic traumatic encephalopathy (CTE)
SWI vs. Other Sequences
| Feature | T2* GRE | SWI |
|---|---|---|
| Technique | 2D gradient echo | 3D gradient echo + phase processing |
| Sensitivity for microbleeds | Moderate | High (superior) |
| Phase information used | No | Yes (phase mask applied) |
| Spatial resolution | Lower | Higher |
| Vein visualization | Moderate | Excellent |
Quantitative Susceptibility Mapping (QSM) - The Next Step
QSM is an advanced post-processing technique applied to SWI raw data that generates quantitative maps of tissue susceptibility. It allows:
- Actual measurement of brain iron concentration
- Better differentiation of calcium vs. iron
- Longitudinal tracking of iron changes in neurodegenerative disease
- Research into disease biomarkers
Example: Multiple Cavernomas on SWI
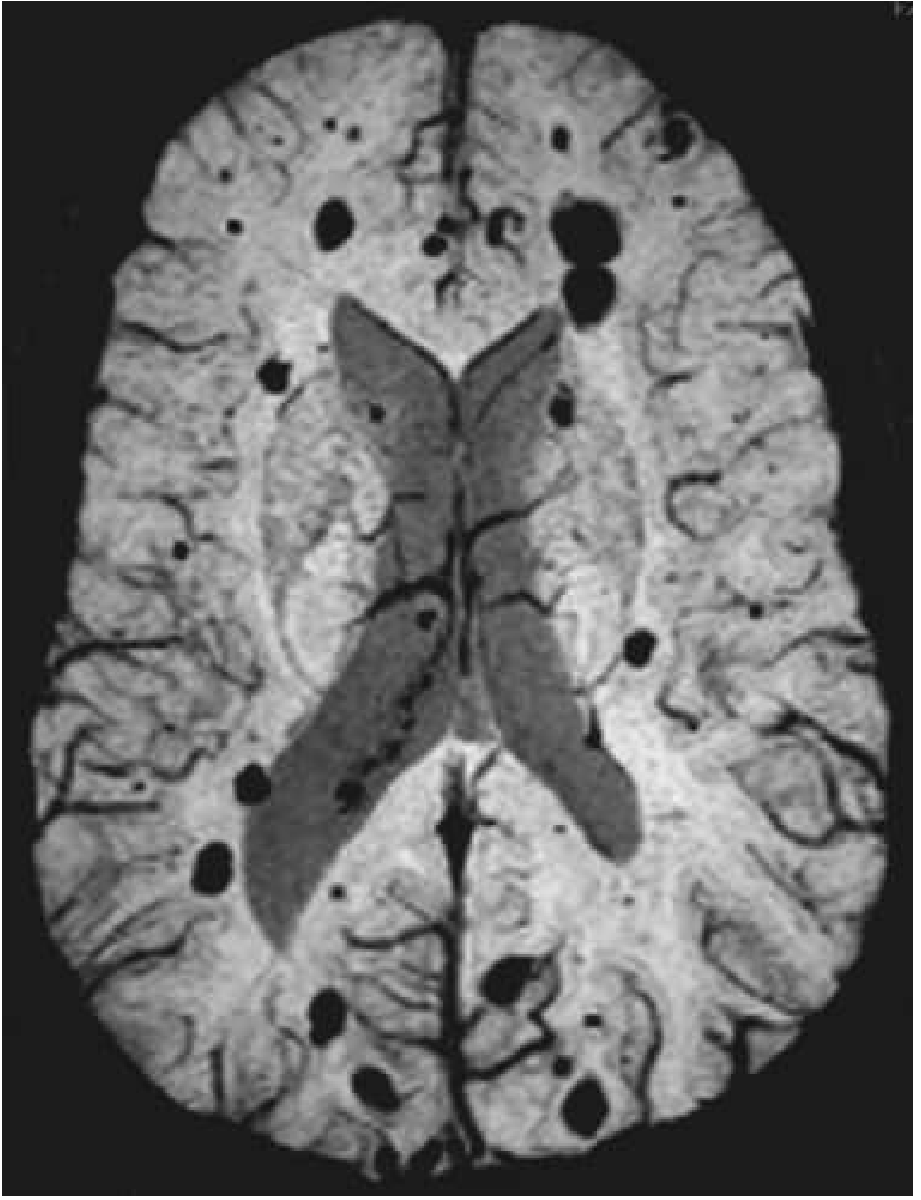
SWI at 3T in a patient with multiple cavernomas. Note the numerous dark (hypointense) circular lesions scattered throughout both hemispheres - each representing a cavernoma with its hemosiderin rim. These would be far less conspicuous on standard T1 or T2 sequences.
Limitations of SWI
- Susceptibility artifacts near air-tissue interfaces (skull base, sinuses, petrous bone) can mimic or obscure lesions
- "Blooming artifact" - lesions appear larger than they really are (can be a feature or a limitation)
- Challenging at the cervical spine due to pulsation and respiratory motion
- Cannot reliably distinguish old from acute blood in all situations
- Calcium and iron can be confused on magnitude images alone (requires phase image)
- Quality varies between MRI vendors and scanner implementations
Sources: Bradley and Daroff's Neurology in Clinical Practice (p. 681); Rosen's Emergency Medicine - Concepts and Clinical Practice; Grainger & Allison's Diagnostic Radiology; Radiology 2021;299:3-26 (Haller et al.)
MR Spectroscopy explanation
Finding Sources
Searching the Web
MR spectroscopy MRS brain metabolites clinical applications NAA choline creatine
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC3539838
Finding Sources
Reading Web Page
https://cdn0.scrvt.com/39b415fb07de4d9656c7b516d8e2d907/1800…
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
I now have comprehensive material from the textbooks and authoritative sources. Here is the full explanation:
MR Spectroscopy (MRS)
What Is MRS?
MR Spectroscopy is a non-invasive MRI technique that measures the chemical composition of tissue rather than its anatomy. Instead of producing an image, it generates a spectrum - a graph of signal peaks, each corresponding to a specific metabolite at a characteristic resonance frequency. It is often called a "virtual biopsy" because it reveals the metabolic fingerprint of a region of interest without tissue sampling.
Physical Basis
All standard MRI uses the resonance of hydrogen (¹H/proton) nuclei to generate images. MRS exploits the same principle but measures the tiny differences in resonance frequency caused by the chemical environment of the proton - called the chemical shift (measured in parts per million, ppm).
- In standard MRI, chemical shift differences are suppressed to create clean anatomical images
- In MRS, these differences are preserved and displayed as a spectrum - each metabolite resonates at a unique ppm value
Key technical point: Water protons overwhelmingly dominate the MR signal. Since metabolites are present at concentrations ~10,000x lower than water, water suppression is essential. Special pulses (e.g., CHESS) selectively null the water peak before acquiring the spectrum.
Acquisition Techniques
Single Voxel Spectroscopy (SVS)
A single rectangular volume of interest (voxel, typically 1-8 cm³) is selected from a region such as a tumor or lesion. Three slice-selective pulses intersect to define the voxel.
- Two common pulse sequences:
- PRESS (Point Resolved Spectroscopy): 90°-180°-180° pulses; most widely used clinically; good signal-to-noise ratio
- STEAM (Stimulated Echo Acquisition Mode): 90°-90°-90° pulses; lower SNR but allows shorter TE; good for short-TE metabolites
Multi-Voxel / Chemical Shift Imaging (CSI / MRSI)
Acquires spectra from multiple voxels simultaneously across a 2D or 3D grid, providing spatial mapping of metabolite distribution across a lesion and surrounding tissue. Useful for heterogeneous tumors and for detecting infiltration beyond the enhancing margin.
Echo Time (TE) Choice
| TE | Metabolites Visible | Use |
|---|---|---|
| Short TE (20-35 ms) | NAA, Cho, Cr, myo-inositol, glutamate/glutamine, lipids | More metabolites, busier spectrum |
| Long TE (135-288 ms) | NAA, Cho, Cr, lactate (inverts at TE=144 ms) | Cleaner spectrum, lactate identification |
The Major Metabolites
N-Acetylaspartate (NAA) - 2.0 ppm
- Marker of neuronal viability and density
- Found almost exclusively in mature neurons
- Decreased in: neuronal death, injury, tumor infiltration (replaced by non-neuronal cells), stroke, MS, dementia, epilepsy
- The single most important metabolite in clinical MRS
Choline (Cho) - 3.2 ppm
- Reflects cell membrane turnover and cellular proliferation
- Includes free choline, glycerophosphocholine, and phosphocholine
- Increased in: actively proliferating tumors, demyelination (MS), inflammation
- Elevated Cho is the hallmark of aggressive neoplasia
Creatine (Cr) - 3.0 ppm
- Marker of cellular energy metabolism (reflects creatine + phosphocreatine)
- Relatively stable across most brain regions and pathologies
- Used as the internal reference standard for calculating metabolite ratios
- Significantly reduced only in inborn errors of creatine metabolism
Lactate (Lac) - 1.3 ppm (doublet)
- Marker of anaerobic glycolysis
- Absent in normal brain
- Present in: ischemia/stroke, high-grade tumors (necrosis), abscesses, mitochondrial disorders
- Distinguishing feature: at TE=144 ms, lactate doublet inverts below baseline (helpful to confirm it's truly lactate and not lipid)
Lipids - 0.9 and 1.3 ppm
- Released with cell membrane destruction
- Found in: necrotic tumors, radiation necrosis, infarction
- Overlaps with lactate at short TE; differentiated at long TE (lipid stays positive, lactate inverts)
Myo-inositol (mI) - 3.56 ppm (short TE only)
- A sugar present almost exclusively in glial cells (astrocytes)
- Elevated in: low-grade gliomas, Alzheimer's disease (glial proliferation)
- Decreased in: hepatic encephalopathy
- Only detectable at short TE
Glutamate + Glutamine (Glx) - 2.1-2.4 ppm (short TE only)
- Excitatory neurotransmitters
- Elevated in: stroke, lymphoma, hypoxic-ischemic injury, hepatic encephalopathy
- Requires short TE; overlapping peaks make separation difficult without high-field scanners
Alanine - 1.47 ppm
- A doublet that also inverts at TE=144 ms (like lactate)
- Specifically elevated in meningiomas - helps distinguish from other extra-axial masses
Key Metabolite Ratios
| Ratio | Normal value | Significance |
|---|---|---|
| Cho/NAA | <1 | >1 suggests neoplasm |
| Cho/Cr | <2.5 | Elevated in tumors and active demyelination |
| NAA/Cr | ~2 | Reduced in neuronal loss |
| Lac/Cr | ~0 | Elevated in ischemia, high-grade tumors |
Clinical Applications
1. Brain Tumors (Most Common Use)
The hallmark tumor spectrum: ↑ Cho, ↓ NAA, ± lactate/lipids
- Tumor vs. radiation necrosis: Radiation necrosis shows ↓↓ all metabolites (dead tissue) + lipids; tumor recurrence shows ↑ Cho. This distinction - often impossible on conventional MRI - is one of MRS's most valuable clinical roles
- Tumor grading: Higher Cho/Cr and Cho/NAA ratios correlate with higher grade; lactate/lipid peaks suggest necrosis (high-grade)
- Tumor vs. abscess: Pyogenic abscesses show free amino acids (valine, leucine, isoleucine) at 0.9 ppm - a near-pathognomonic finding
- Glioma vs. metastasis: Metastases show elevated Cho only within the lesion; gliomas show Cho elevation extending beyond the enhancing margin (infiltration)
- Meningioma: Alanine peak (inverted doublet at TE=144 ms) + absent NAA (no neurons) + elevated Cho
- Low-grade glioma: Elevated myo-inositol is characteristic
2. Stroke and Ischemia
- Acute/subacute: ↑ Lactate (anaerobic metabolism), ↓ NAA (neuronal death)
- Lactate appears within minutes of ischemia - MRS can detect metabolic failure before structural T2 changes appear
- Monitors tissue viability in the ischemic penumbra
3. Multiple Sclerosis
- Active plaques: ↑ Cho (demyelination/membrane breakdown), ↓ NAA
- Normal-appearing white matter: ↓ NAA indicates diffuse axonal injury not seen on conventional MRI
- NAA recovery after relapse correlates with clinical improvement
4. Epilepsy
- Temporal lobe epilepsy: ↓ NAA in the ipsilateral hippocampus helps lateralize the seizure focus for surgical planning
- Can identify the epileptogenic zone when MRI is normal
5. Dementia
- Alzheimer's disease: ↓ NAA (neuronal loss), ↑ myo-inositol (astrogliosis)
- Hepatic encephalopathy: ↓ myo-inositol, ↑ Glx (glutamine from ammonia metabolism)
- Creutzfeldt-Jakob disease: ↓ NAA + ↑ myo-inositol
6. Metabolic and Mitochondrial Disorders
- Creatine deficiency syndromes: absent/markedly reduced Cr peak
- Mitochondrial disorders (e.g., MELAS): elevated lactate in brain
- Canavan disease: massive ↑ NAA (deficiency of aspartoacylase)
Limitations of MRS
- Low sensitivity: Metabolites are at millimolar concentrations - only the most abundant are detectable
- Spatial resolution is poor compared to structural MRI; voxels are large (cm³ scale), averaging over heterogeneous tissue
- Susceptibility artifacts near bone, air cavities, or hemorrhage degrade spectra
- Water/lipid contamination from adjacent CSF or scalp fat can overwhelm metabolite peaks if voxel placement is imprecise
- Long acquisition time (3-15 minutes for SVS; longer for CSI)
- Operator dependence: Voxel placement, shimming, and water suppression quality critically affect results
- Limited to mobile molecules: Macromolecular-bound metabolites are invisible
- Not yet fully standardized across vendors and institutions - limiting broad clinical adoption
Summary: MRS in a Nutshell
| Metabolite | Location (ppm) | What it measures | Up in | Down in |
|---|---|---|---|---|
| NAA | 2.0 | Neuronal integrity | Canavan disease | Tumors, stroke, MS, dementia |
| Cho | 3.2 | Cell membrane turnover | Tumors, MS | -- |
| Cr | 3.0 | Energy metabolism | -- | Creatine deficiency |
| Lactate | 1.3 | Anaerobic glycolysis | Ischemia, high-grade tumors | (absent normally) |
| mI | 3.56 | Glial cells | Low-grade glioma, Alzheimer's | Hepatic encephalopathy |
| Lipids | 0.9/1.3 | Membrane destruction | Necrosis | -- |
| Alanine | 1.47 | (specific) | Meningioma | -- |
Sources: Bradley and Daroff's Neurology in Clinical Practice; Grainger & Allison's Diagnostic Radiology (p. 1365); Springer European Biophysics Journal MRS review; Siemens MRS Neuroimaging Guide (Radiology 2021)
This is a shared conversation. Sign in to Orris to start your own chat.