Cora in Orthopaedics in 10 marks pg answer with flow chart and images
CORA center of rotation of angulation orthopaedics deformity correction 10 marks
https://abs.orthofix.it/blog/cora-center-of-rotation-of-angu…
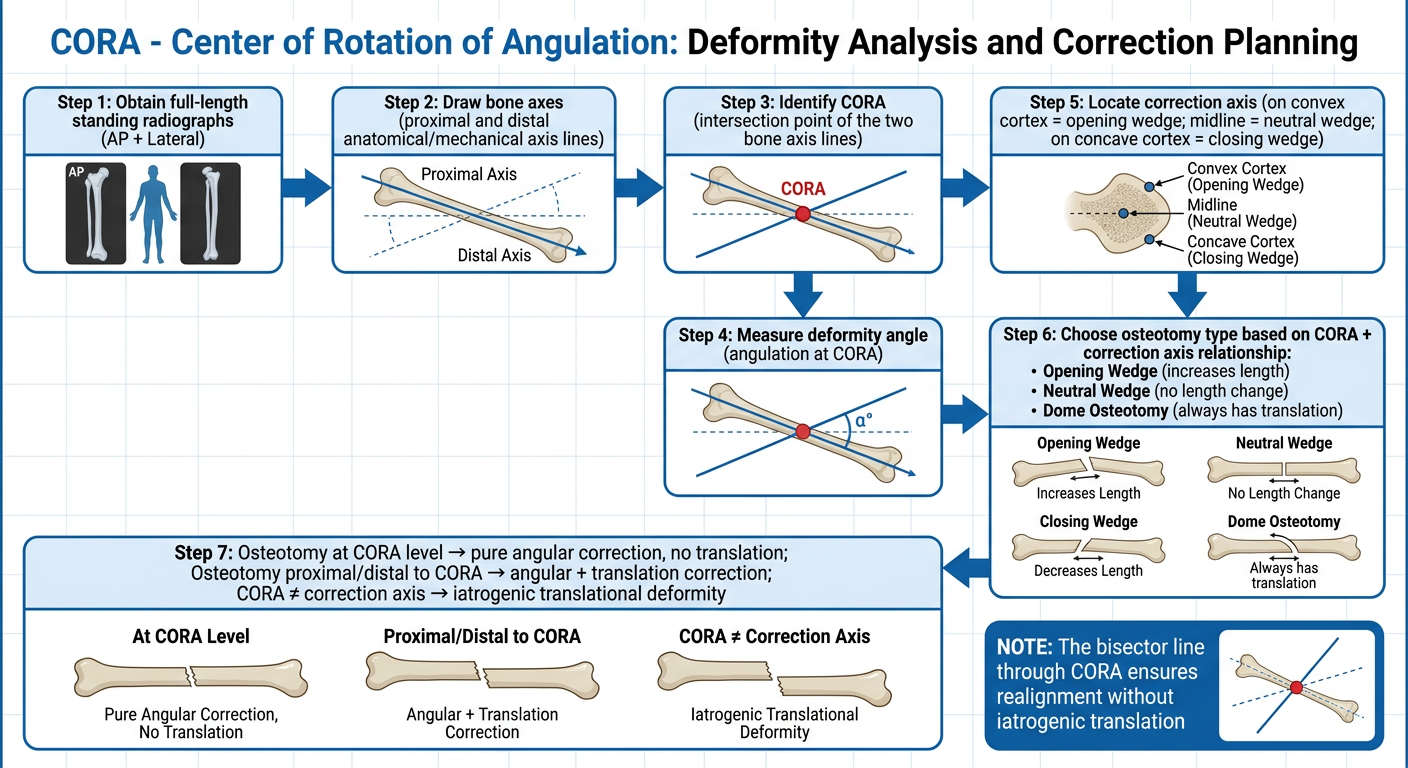
A clean medical flowchart titled "CORA - Center of Rotation of Angulation: Deformity Analysis and Correction Planning" showing the step-by-step process: Step 1: Obtain full-length standing radiographs (AP + Lateral) → Step 2: Draw bone axes (proximal and distal anatomical/mechanical axis lines) → Step 3: Identify CORA (intersection point of the two bone axis lines) → Step 4: Measure deformity angle (angulation at CORA) → Step 5: Locate correction axis (on convex cortex = opening wedge; midline = neutral wedge; on concave cortex = closing wedge) → Step 6: Choose osteotomy type based on CORA + correction axis relationship: Opening Wedge (increases length), Neutral Wedge (no length change), Closing Wedge (decreases length), Dome Osteotomy (always has translation) → Step 7: Osteotomy at CORA level → pure angular correction, no translation; Osteotomy proximal/distal to CORA → angular + translation correction; CORA ≠ correction axis → iatrogenic translational deformity. Include a note box: "The bisector line through CORA ensures realignment without iatrogenic translation". Use professional medical diagram style with blue and white colors.
CORA (Center of Rotation of Angulation) in Orthopaedics
Definition
The CORA concept was systematized by Paley and colleagues and has become the universal standard for preoperative planning of osteotomies in limb deformity correction.
Flowchart: Step-by-Step CORA Method
Step-by-Step Methodology
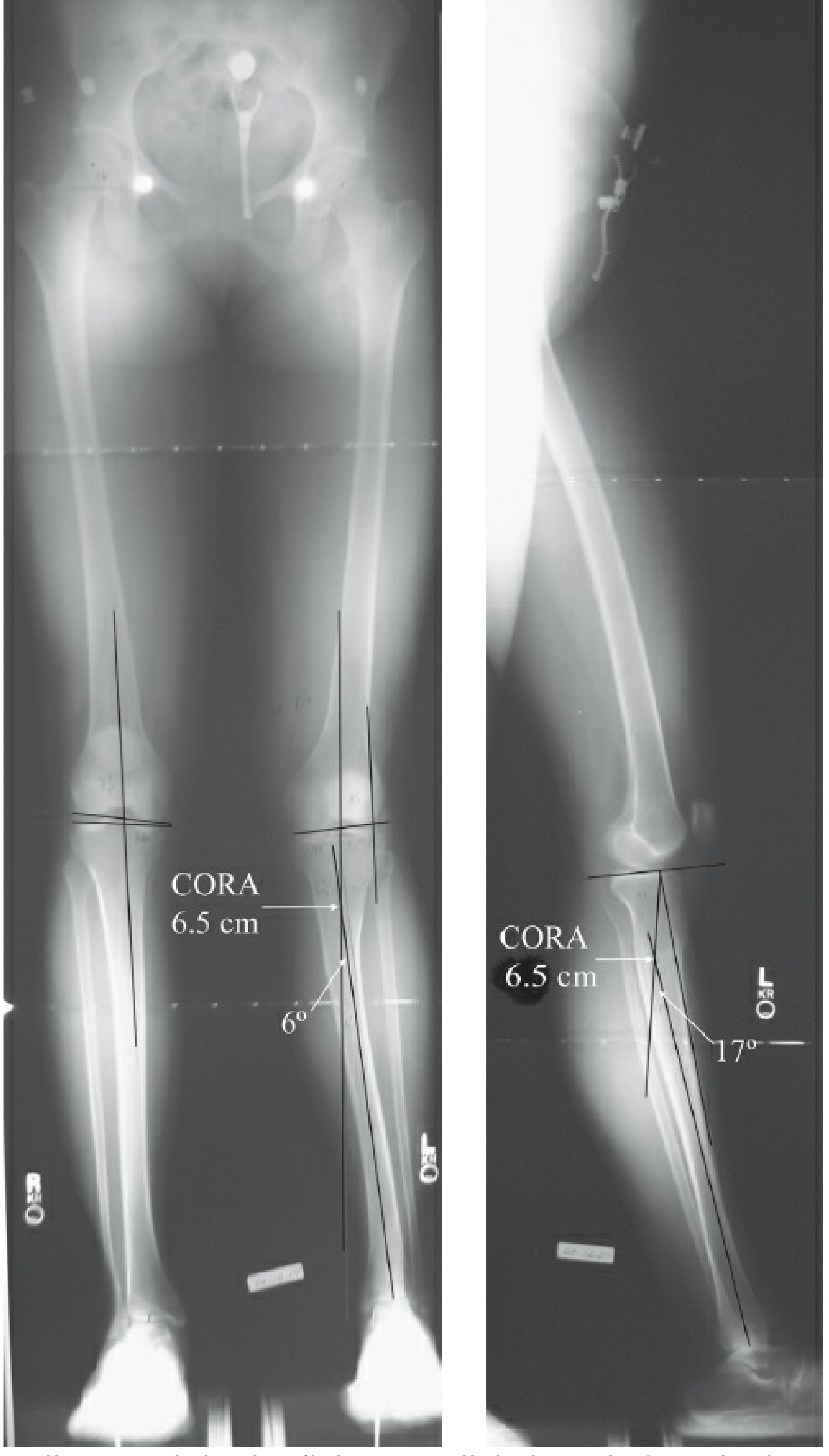
Step 1: Radiographic Assessment
- Obtain long-leg standing radiographs (51-inch AP and lateral views)
- Assess: limb alignment, mechanical axis deviation (MAD), joint orientation angles
- Normal MAD = 1-15 mm medial to knee joint center
Step 2: Draw Bone Axes
- Draw the proximal bone axis (anatomic or mechanical) above the deformity
- Draw the distal bone axis below the deformity
- These two lines will diverge/intersect at the site of deformity
Step 3: Locate the CORA
- The intersection point of the proximal and distal axes = CORA
- The CORA lies at the apex of angulation
- A bisector line runs through the CORA at equal angles to both axes - correction along this line ensures pure angular correction without translation
Deformity Types Analyzed by CORA
| Deformity Type | Description |
|---|---|
| Length | Shortening or overlengthening - measured joint center to joint center |
| Angulation | Magnitude + direction of apex; CORA identifies the level |
| Rotation | About longitudinal axis; measured by clinical exam or axial CT |
| Translation | Parallel shift of bone axes; identified when CORA from two methods differs |
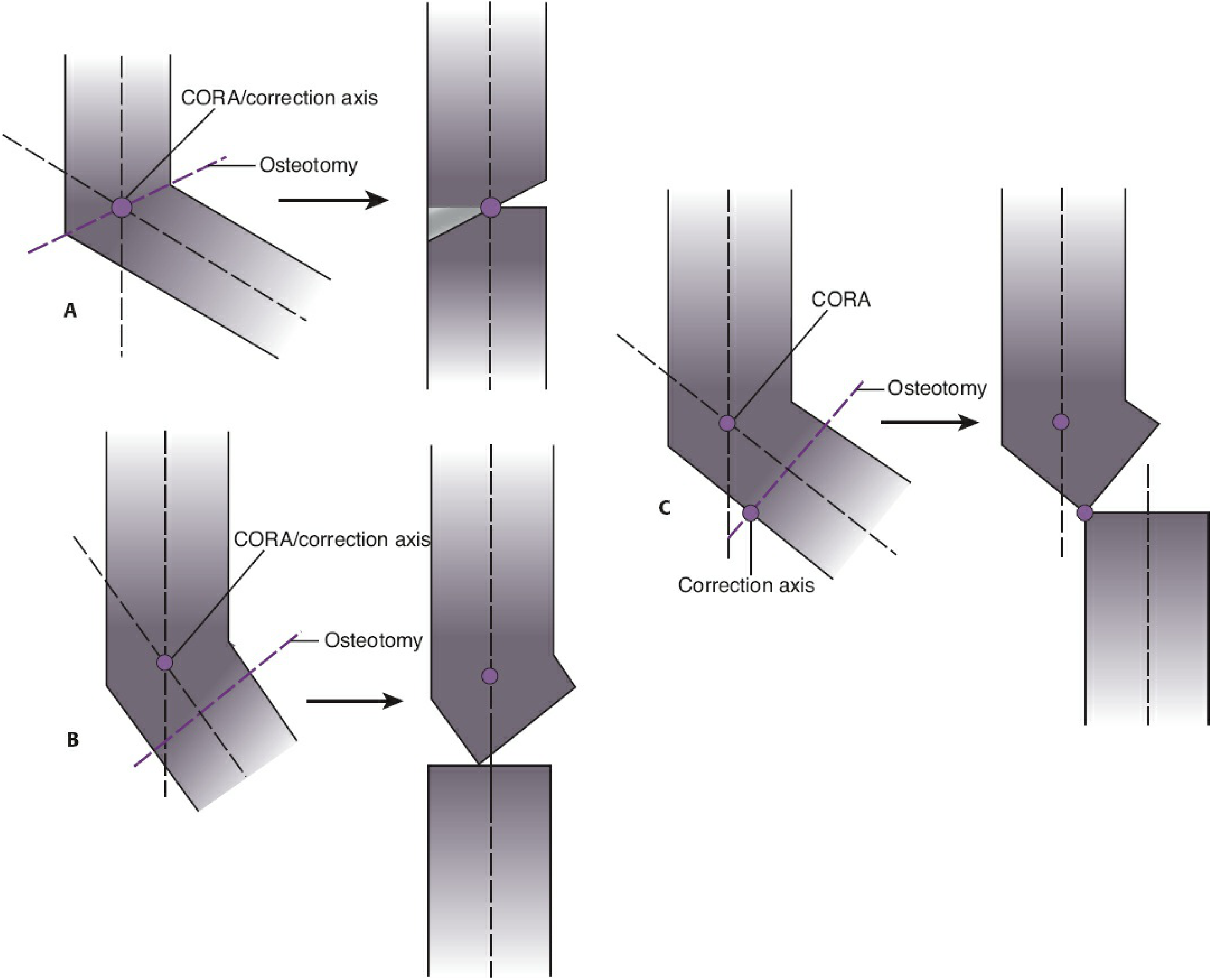
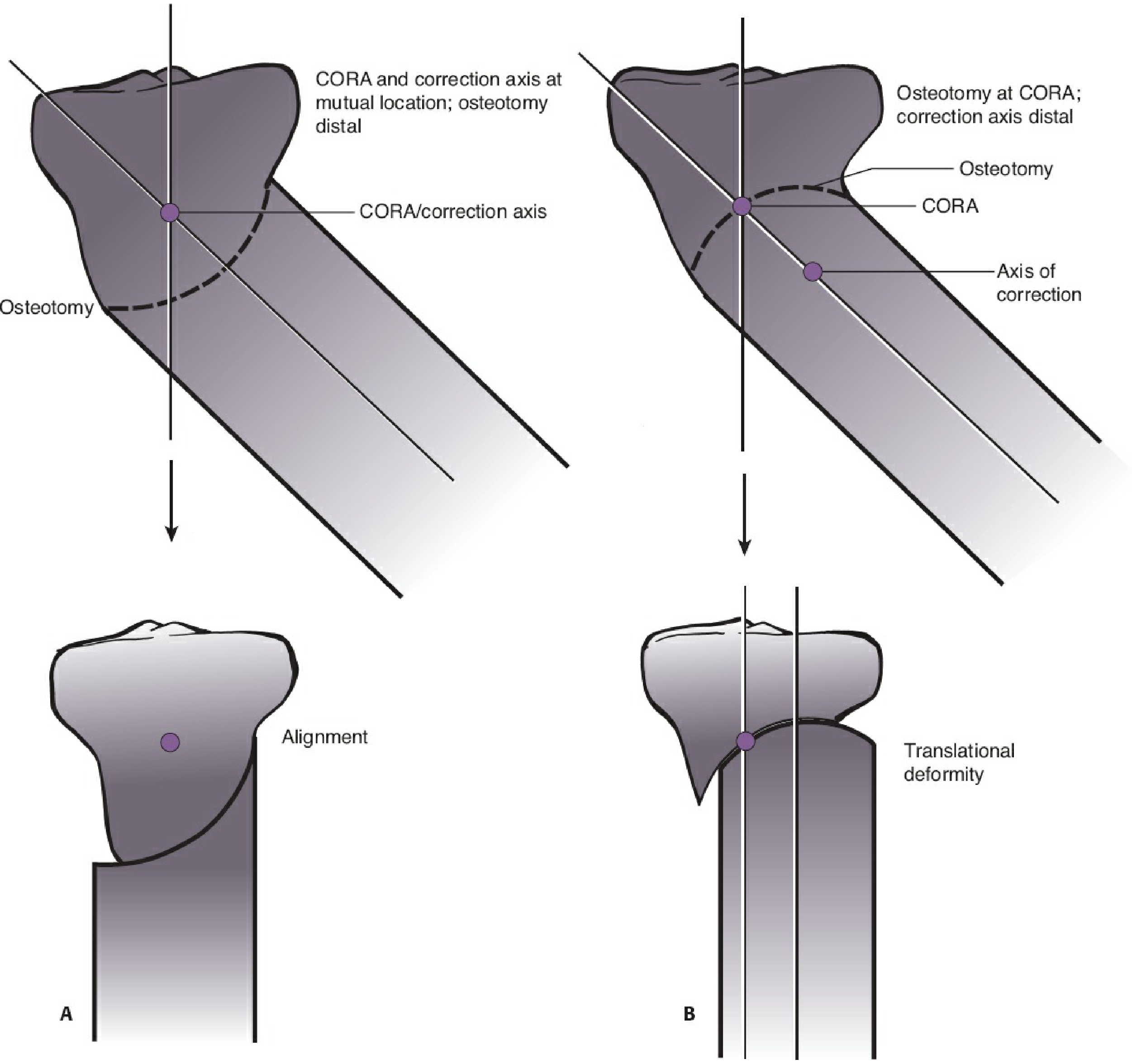
Osteotomy Rules (The Core of CORA)
| Scenario | CORA | Correction Axis | Osteotomy | Result |
|---|---|---|---|---|
| A (Ideal) | Same point | Same point | At CORA | Pure angular correction, NO translation |
| B | Same point | Same point | Proximal or distal to CORA | Angular + obligatory translation (acceptable) |
| C (Avoid) | Different point | Different point | - | Iatrogenic translational deformity |
Types of Wedge Osteotomies Based on CORA Position
1. Opening Wedge Osteotomy
- CORA and correction axis lie on the convex cortex
- Concave side cortex is distracted to restore alignment
- Increases bone length
- Empty wedge-shaped gap traverses the bone diameter
2. Neutral Wedge Osteotomy
- CORA and correction axis lie in the center of the bone
- Concave side distracted, convex side compressed
- A bone wedge is removed from convex side
- No change in bone length
3. Closing Wedge Osteotomy
- CORA and correction axis lie on the concave cortex
- Convex side cortex is compressed to restore alignment
- Bone wedge removed across entire diameter
- Decreases bone length (shortening)
4. Dome Osteotomy
- The osteotomy arc cannot pass through both CORA and correction axis simultaneously - translation always occurs
- If CORA and correction axis are at mutual location with osteotomy proximal/distal: angulation + translation results in realignment
- Can be opening, neutral, or closing depending on CORA position
- Unlike wedge osteotomies, bone removal is rarely needed
Multiple CORAs (Complex/Multi-Apical Deformities)
- When a bone has deformity at more than one level, multiple CORAs are identified
- Each CORA requires a separate osteotomy at its level
- Translational deformity (parallel shift of bone axes without angulation) has two different CORAs (one from each method of axis drawing); correction requires two wedge osteotomies of equal magnitude in opposite directions
Key Take-Home Points
- The CORA is identified at the intersection of proximal and distal bone axes
- Correction of angulation by rotating the bone around a point on the bisector line through the CORA ensures realignment without iatrogenic translation
- If the osteotomy site = CORA = correction axis: pure angular correction
- If the correction axis ≠ CORA: iatrogenic translation is introduced
- Wedge osteotomy type (opening/neutral/closing) depends on where the correction axis lies relative to the bone cross-section
- Dome osteotomies always involve some translation - plan the CORA-correction axis relationship accordingly
- The CORA method is applicable to any fixation technique (internal or external fixator, Ilizarov, etc.)
Summary Table
| Feature | Details |
|---|---|
| Full form | Center of Rotation of Angulation |
| Definition | Intersection of proximal and distal bone axes on radiograph |
| Purpose | Localizes apex of deformity for osteotomy planning |
| Bisector line | Line through CORA = safe correction axis for pure angular correction |
| Opening wedge | CORA on convex cortex; lengthens bone |
| Neutral wedge | CORA at bone center; no length change |
| Closing wedge | CORA on concave cortex; shortens bone |
| Dome osteotomy | Always has translation; plan accordingly |
| Multi-CORA | Multi-apical or translational deformity; needs multiple osteotomies |