Secondary suturing for burst abdomen
"burst abdomen" AND "secondary suture"
"abdominal wound dehiscence" AND repair
secondary suturing burst abdomen technique tension sutures surgical steps
https://www.vumc.org/global-surgical-atlas/sites/default/fil…
Secondary Suturing for Burst Abdomen (Wound Dehiscence)
Definition and Overview
- Bailey & Love's Short Practice of Surgery, 28th ed., p. 5799
When Does It Occur?
- Most commonly on day 5-8 post-operatively, when wound tensile strength is at its lowest
- Often heralded by a serosanguinous ("pink fluid") discharge from the wound - a classic warning sign
- The patient may report a "popping" sensation after straining or coughing
Risk Factors
- Malnutrition, obesity, diabetes mellitus
- Renal failure, jaundice
- Sepsis, malignancy
- Steroid therapy
- Emergency surgery
- Inadequate or poorly tensioned wound closure
- Infection, haematoma, or seroma at the wound
- Raised intra-abdominal pressure (bowel obstruction, COPD with excessive coughing)
Pre-operative Management (Before Return to Theatre)
- Cover eviscerated bowel immediately with warm, moist saline-soaked packs
- Keep the patient NBM; establish IV access
- Correct fluid and electrolyte imbalances
- Administer systemic antibiotics
- If evisceration is NOT present: an abdominal binder may be used as a temporising measure; however, if the full extent of dehiscence is uncertain, operative exploration is mandatory
- Plan for general anaesthesia - this operation cannot be adequately performed under local or spinal anaesthesia
Surgical Technique: Secondary Suturing
1. Anaesthesia and Preparation
- Performed in the operating theatre under general anaesthesia
- Full muscle relaxation is needed to allow re-approximation of the fascia without undue tension
2. Wound Exploration
- Open the entire skin incision
- Carefully inspect and trace the fascial closure suture back to intact, non-dehisced fascia
- Debride all non-viable and infected tissue at fascial edges - anatomy must be clear before closure
3. Abdominal Exploration and Lavage
- Gently explore the peritoneal cavity, especially if there is purulent, feculent, or bilious discharge - the source must be identified and managed
- If the wound is clean (no purulent discharge), limit exploration to avoid iatrogenic bowel injury
- Lavage the peritoneal cavity with warm normal saline
4. Placement of Retention Sutures (before tying)
- Using heavy non-absorbable monofilament or braided suture (e.g., No. 2 nylon, Prolene, or stainless steel)
- Placed 3-4 cm from the fascial edge, passing through: skin → subcutaneous fat → anterior rectus sheath → rectus muscle → posterior rectus sheath → peritoneum (full thickness)
- These are placed without tying at this stage
- Sutures should ideally lie in the extraperitoneal/preperitoneal space to minimise visceral contact and avoid the "cheese wire" effect on bowel loops
- Protect bowel with a malleable retractor during each needle pass; needle must be visualised at all times
5. Fascial Closure
- Close the fascia using large bites of non-absorbable suture (e.g., Prolene or PDS), using the mass-closure technique
- Begin with sutures at each end of the wound and meet in the middle
- Final sutures are placed without excessive tension to allow adequate visualisation and needle passage
- Important note: the peritoneum does not need to be closed separately - it does not contribute significantly to wound strength
6. Skin Closure and Tying of Retention Sutures
- Close the skin very loosely (this is a contaminated/potentially infected field)
- Thread each retention suture through a short segment of sterile IV tubing (or red rubber catheter bolster) to distribute pressure across the skin and prevent suture cut-through
- Tie down the retention sutures - no excessive tension required
7. Post-operative wound management
- In patients with suspected infection, poor tissue quality, or excessive tension - it may be preferable to leave the wound open and manage with regular dressings or vacuum-assisted closure (VAC) pumps
Retention Sutures: Key Points
| Feature | Detail |
|---|---|
| Material | Heavy No. 1 or 2 non-absorbable nylon, Prolene, or braided nylon |
| Placement | Through all layers, 3-4 cm lateral to fascial edge |
| Purpose | Reduce evisceration risk if fascial closure fails; do NOT prevent dehiscence itself |
| Bolster | IV tubing or red rubber catheter prevents skin cut-through |
| Tying | Loose - over bolster only; overtightening causes pressure necrosis |
| Removal | After 6-8 weeks (retain until skin wound well healed for 3-4 weeks minimum) |
| Drawbacks | Substantially uncomfortable, cause skin breakdown and wound complications |
- Current Surgical Therapy, 14th ed., p. 1422; Pye's Surgical Handicraft, 22nd ed., p. 7262
- VUMC Global Surgical Atlas - Closure of Laparotomy Wound Dehiscence (Davis R.)
Role of Retention Sutures in Prevention (Prophylactic Use)
-
Indication: Elderly patients, malignancy, bowel obstruction, contaminated wounds, malnutrition
-
Evidence is mixed: Khorgami et al. (2013, RCT of 300 patients) showed a significantly lower wound dehiscence rate with retention sutures (4% vs. 13.3%); however, evisceration rates did not differ
-
Rink et al. (2000) found no difference in wound failure but increased patient morbidity (discomfort) with retention sutures
-
Modern trend favours mass closure (a single-layer, continuous technique taking large bites of fascia), which has made prophylactic tension sutures largely obsolete - associated with <1% wound dehiscence rate and 5-10% incisional hernia rate
-
Campbell Walsh Wein Urology, p. 1457; Pye's Surgical Handicraft, p. 7262
Post-operative Care After Secondary Suturing
- Aggressive nutritional support: high-protein diet, multivitamins; treat any underlying malnutrition
- Treat sepsis and any causative condition aggressively
- Manage factors that raise intra-abdominal pressure (ileus, COPD, ascites)
- Remove retention sutures only after the skin wound has been well healed for at least 3-4 weeks (typically 6-8 weeks total)
Alternatives When Primary Re-closure is Not Feasible
- Vacuum-assisted closure (VAC/NPWT): Open abdomen management with negative pressure wound therapy, sometimes combined with mesh-mediated fascial traction
- Planned ventral hernia: Skin closure only, with later elective repair
- Biological or synthetic mesh bridging: For patients with true loss of abdominal domain
Give in detail of retention suturing for burst abdomen for my seminar with relavent images and video link that I can show
retention sutures burst abdomen technique surgical video YouTube
"retention sutures" AND "abdominal dehiscence"
retention sutures burst abdomen bolster technique images diagram anatomy layers
site:youtube.com "retention sutures" OR "burst abdomen" secondary closure surgical technique
https://pmc.ncbi.nlm.nih.gov/articles/PMC6114125
Retention Suturing for Burst Abdomen
A Detailed Seminar Guide
1. What is Burst Abdomen (Wound Dehiscence)?
Classic Presentation
- Pink/serosanguinous wound discharge (often precedes burst)
- Patient reports a "popping" or "giving way" sensation during coughing or straining
- Visible wound opening, with or without evisceration of bowel/omentum
2. Clinical Photo: Complete Fascial Dehiscence

3. Risk Factors (for Seminar Summary Box)
| Systemic | Local / Technical |
|---|---|
| Malnutrition / hypoalbuminaemia | Poor closure technique |
| Obesity | Wound infection / haematoma |
| Diabetes mellitus | Suture cut-through |
| Malignancy | Raised intra-abdominal pressure |
| Steroid / immunosuppressive therapy | Bowel obstruction / ileus |
| Renal failure / jaundice | Post-op coughing (COPD) |
| Sepsis | Emergency surgery (contamination) |
| Elderly age | Fascial ischaemia |
Key mechanism: Increased collagenolytic activity (collagenase) within 0.5-0.75 cm of the wound edge is the main biochemical driver of suture cut-through.
4. What Are Retention Sutures?
Their Purpose (Critical Point for Seminar)
Retention sutures do NOT prevent fascial dehiscence - they prevent evisceration if the fascial closure fails. This is a frequently tested distinction.
- Current Surgical Therapy, 14th ed., p. 1422; Sabiston Textbook of Surgery, p. 2059
5. Types of Retention Sutures
A. External (Full-Thickness / Through-and-Through)
- Pass through: skin → subcutaneous fat → anterior fascia → muscle → posterior fascia → peritoneum
- Tied over a bolster (IV tubing / red rubber catheter) on the skin surface
- Visible on the surface as a "ladder" or "railroad track" pattern
- More secure but creates an unsightly scar and more skin complications
B. Internal (Extraperitoneal / Subfascial)
- Pass through all layers except the skin - lie in the preperitoneal/extraperitoneal space
- Avoids the cheese-wire effect on bowel loops
- Does not produce a surface ladder-pattern scar
- Cannot be released without reopening the wound
6. Layers of the Abdominal Wall (Anatomy Refresher for Seminar)
7. Layered Closure Overview (Context)
8. Step-by-Step Surgical Technique
Step 1 - Anaesthesia and Theatre Setup
- General anaesthesia with full muscle relaxation is mandatory
- Cannot be done under local/spinal - adequate relaxation is needed to approximate retracted fascia
- Broad-spectrum antibiotics pre-operatively
- Position: supine; full sterile prep and draping
Step 2 - Wound Exploration and Debridement
- Open the entire skin incision
- Trace the fascial suture back to intact fascia at both ends
- Debride all non-viable tissue at fascial edges - fresh, bleeding fascia must be exposed for a good bite
- Identify and remove any infected or necrotic material
Step 3 - Abdominal Exploration and Lavage
- If purulent, feculent, or bilious discharge is present: find and manage the source (anastomotic leak, perforation)
- Gentle downward pressure on bowel for limited visualisation if no discharge
- Lavage with warm normal saline (2-3 litres minimum)
- Limit unnecessary exploration to avoid iatrogenic bowel injury
Step 4 - Place Retention Sutures FIRST (Before Tying)
- 3-4 cm lateral to the fascial edge (some texts say 4-6 cm)
- 3-5 cm apart from each other along the wound length
- Full thickness: skin → subcutaneous fat → anterior sheath → rectus → posterior sheath → peritoneum
- Pass extraperitoneally wherever possible to avoid bowel contact
- Always keep the needle in direct visual field
- Use a malleable retractor to depress and protect underlying bowel during each pass
- Never pass the needle blindly
Step 5 - Fascial Closure (Mass Closure Technique)
- Close the fascia using a non-absorbable suture (e.g., No. 1 Prolene or PDS)
- Large, consistent bites of fascia (1-2 cm from edge, 1 cm apart - Jenkins' rule: suture length = 4× wound length)
- Mass closure (single layer, all fascial layers together) is preferred over layered closure
- Interrupted sutures are preferred over continuous in high-risk/contaminated cases - single stitch failure then cannot open the whole wound
- Peritoneum closure is NOT required and does NOT contribute to wound strength
- Begin at each end and meet in the middle
Step 6 - Tie the Retention Sutures Over a Bolster
- Cut sterile IV tubing (or red rubber catheter, or commercial bolster) into 4-5 cm strips
- Thread each retention suture through a strip of IV tubing
- Tie down firmly but without excessive tension - overtightening causes pressure necrosis and skin cut-through
- The bolster distributes force over a wide area of skin, preventing the "cheese wire" effect
Step 7 - Skin Closure
- Close skin loosely (loosely approximated - not tight)
- In frankly infected wounds: leave skin open and pack with antiseptic/saline-soaked gauze
- In contaminated-but-not-infected wounds: loose interrupted skin sutures or clips
- Consider a superficial wound drain in the subcutaneous space
9. Retention Suture Configurations (Cross-Sectional Diagrams)

10. Post-operative Management
| Issue | Action |
|---|---|
| Nutrition | High-protein diet + multivitamins immediately post-op; treat malnutrition aggressively |
| Infection | Continue targeted antibiotics; wound surveillance |
| IAP monitoring | Monitor intra-abdominal pressure (bladder pressure) - retention sutures can raise IAP (normal = 5-7 mmHg) |
| Respiratory | Incentive spirometry; physio for COPD patients |
| Skin care | Daily inspection under bolsters for pressure necrosis |
| DVT prophylaxis | LMWH + compression stockings |
| Suture removal | Remove retention sutures after 6-8 weeks - only after skin wound has been well healed for at least 3-4 weeks |
11. Complications of Retention Sutures
| Complication | Mechanism | Prevention |
|---|---|---|
| Pressure necrosis / skin breakdown | Suture cuts into skin | Use bolster/IV tubing; avoid overtightening |
| Pain / discomfort | Constant tension on skin | Warn patient; analgesia |
| Raised intra-abdominal pressure (IAP/IAH) | Reduced abdominal wall compliance | Monitor bladder pressure; remove early if IAH develops |
| Bowel entrapment / cut-through | Suture loop around bowel | Keep sutures extraperitoneal; use malleable retractor |
| Ugly scar ("ladder" / "railroad" pattern) | Full-thickness suture marks | Use internal retention sutures if possible |
| Wound infection | Foreign body reaction | Strict aseptic technique; avoid excessive tension |
| Incisional hernia | Despite retention sutures, 43% develop hernia | Correct nutrition, treat infection |
Key evidence (PMC6114125): Retention sutures reduce abdominal wall compliance, which can paradoxically raise intra-abdominal pressure (IAH occurs in ~12% of post-operative patients). They should be used cautiously in patients already at risk of raised IAP.
12. Prophylactic vs Therapeutic Use
| Prophylactic | Therapeutic (Secondary Suturing) | |
|---|---|---|
| Timing | At primary closure | At secondary re-operation for burst abdomen |
| Indication | High-risk patients (malnourished, malignancy, contaminated field) | Established full-thickness dehiscence ± evisceration |
| Evidence | Mixed; Khorgami RCT (2013): 4% vs 13.3% dehiscence (p=0.007) | Standard of care for full-thickness dehiscence |
| Trend | Moving away from routine use; mass closure preferred | Still the recommended primary repair technique |
13. Alternatives When Primary Re-closure is Not Possible
- VAC/NPWT (Vacuum-Assisted Closure) - negative pressure wound therapy; promotes granulation; used for open abdomen management
- Dynamic retention sutures (ABRA system) - sequential tightening devices that gradually approximate fascial edges over days
- Planned ventral hernia - skin closure only, elective mesh repair later
- Mesh bridging - biological or synthetic mesh when primary fascial approximation is impossible
14. Video Resources for Your Seminar
-
Retention sutures (mass closure) - Burst abdomen - covers retention sutures specifically for burst abdomen with rectus anatomy
-
Secondary Suturing for Burst Abdomen - Dr Jay Mehta - a trained cancer surgeon demonstrating the actual operative technique (most directly relevant for your seminar)
-
How to Apply Retention Sutures - Dr Tayyab Riaz - focused tutorial on retention suture placement technique
-
Abdominal Wall Closure - Prof. Chintamani - describes mass closure / Jenkins rule in detail
-
Mass / Tension Closure for Midline Laparotomy - demonstrates tension suture technique for midline laparotomy closure
15. Summary Box for Seminar Slide
Secondary Retention Suturing - Key Points
- Burst abdomen = surgical emergency; return to theatre under GA
- Retention sutures = full-thickness, heavy nylon (No. 1-2), 3-4 cm from edge, 3-5 cm apart
- Placed BEFORE tying; fascia closed FIRST with mass closure
- Tied over bolster (IV tubing) - never overtight
- They prevent evisceration, NOT dehiscence
- Leave in situ 6-8 weeks; remove after skin fully healed
- Monitor for IAP rise, pressure necrosis, and pain post-op
- Aggressive nutrition is as important as the suture technique
Create a PowerPoint presentation on burst abdomen management with these images and diagrams
mkdir -p /home/daytona/workspace/burst-abdomen-ppt && node /home/daytona/skills/shared/scripts/fetch_images.js \ "https://cdn.orris.care/cdss_images/49fc1f3c6f0d85667052744536224df2f9cd16ebec6f0068079c586f40e36fca.png" \ "https://basicmedicalkey.com/wp-content/uploads/2017/04/B9780323073585000371_f28-09af-9780323073585.jpg" \ "https://resources.ama.uk.com/glowm_www/graphics/figures/v1/0560/008f.gif" \ "https://media.springernature.com/lw1200/springer-static/image/art%3A10.1007%2Fs00423-023-02954-w/MediaObjects/423_2023_2954_Fig2_HTML.png" \ "https://oncohemakey.com/wp-content/uploads/2016/12/image01770.jpeg" \ 2>/dev/null | node -e " const data = require('fs').readFileSync('/dev/stdin','utf8'); const imgs = JSON.parse(data); imgs.forEach((img,i) => { const status = img.error ? 'FAILED: '+img.error : 'OK ('+img.base64.substring(0,30)+'...)'; console.log(i, status.substring(0,80)); }); "
~/burst-abdomen-ppt/build.js
const pptxgen = require("pptxgenjs");
const { execSync } = require("child_process");
// ── Color palette (deep surgical blue / crimson / off-white) ─────────────────
const C = {
darkBlue: "0D2B4E", // dominant dark bg
midBlue: "1A4A7A", // section headers
accent: "C0392B", // crimson accent (surgical / urgent)
accentGold:"E8A020", // gold highlight
white: "FFFFFF",
offWhite: "F0F4F8",
lightBlue: "D6E8F5",
textDark: "1A1A2E",
textMid: "2C3E6B",
subtleGray:"8899AA",
};
// ── Fetch all images ──────────────────────────────────────────────────────────
console.log("Fetching images...");
const imageUrls = [
"https://cdn.orris.care/cdss_images/49fc1f3c6f0d85667052744536224df2f9cd16ebec6f0068079c586f40e36fca.png",
"https://basicmedicalkey.com/wp-content/uploads/2017/04/B9780323073585000371_f28-09af-9780323073585.jpg",
"https://resources.ama.uk.com/glowm_www/graphics/figures/v1/0560/008f.gif",
"https://media.springernature.com/lw1200/springer-static/image/art%3A10.1007%2Fs00423-023-02954-w/MediaObjects/423_2023_2954_Fig2_HTML.png",
"https://oncohemakey.com/wp-content/uploads/2016/12/image01770.jpeg",
];
const fetched = JSON.parse(
execSync(`node /home/daytona/skills/shared/scripts/fetch_images.js ${imageUrls.map(u => `"${u}"`).join(" ")}`).toString()
);
const [imgDehiscence, imgLayers, imgConfigs, imgTechniques, imgAnatomy] = fetched.map(f => f.base64);
// ── Helpers ───────────────────────────────────────────────────────────────────
function darkSlide(pres) {
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.darkBlue } });
return s;
}
function lightSlide(pres) {
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite } });
return s;
}
function sectionHeader(s, pres, title, subtitle) {
// Left accent bar
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.35, h: 5.625, fill: { color: C.accent } });
// Title
s.addText(title, {
x: 0.6, y: 1.5, w: 8.8, h: 1.2,
fontSize: 40, bold: true, color: C.white, fontFace: "Calibri",
});
if (subtitle) {
s.addText(subtitle, {
x: 0.6, y: 2.9, w: 8.8, h: 0.7,
fontSize: 20, color: C.lightBlue, fontFace: "Calibri", italic: true,
});
}
}
function slideHeader(s, pres, title) {
// Top bar
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: C.midBlue } });
// Left accent strip
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.2, h: 5.625, fill: { color: C.accent } });
s.addText(title, {
x: 0.35, y: 0.08, w: 9.3, h: 0.55,
fontSize: 22, bold: true, color: C.white, fontFace: "Calibri",
valign: "middle", margin: 0,
});
}
function footer(s, text) {
s.addText(text, {
x: 0, y: 5.35, w: 10, h: 0.28,
fontSize: 9, color: C.subtleGray, align: "center", fontFace: "Calibri",
});
}
function bulletBox(s, items, opts) {
const textArr = items.map((item, i) => ({
text: item,
options: { bullet: true, breakLine: i < items.length - 1, fontSize: opts.fontSize || 14, color: opts.color || C.textDark, fontFace: "Calibri" }
}));
s.addShape(s._pptx ? s._pptx.shapes.RECTANGLE : "rect", {
x: opts.x, y: opts.y, w: opts.w, h: opts.h, fill: { color: opts.bg || C.white },
shadow: { type: "outer", color: "000000", blur: 5, offset: 2, angle: 135, opacity: 0.1 },
});
s.addText(textArr, { x: opts.x + 0.15, y: opts.y + 0.1, w: opts.w - 0.3, h: opts.h - 0.2 });
}
function pill(s, pres, label, x, y, w, bg, fg) {
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x, y, w, h: 0.42, fill: { color: bg }, rectRadius: 0.05 });
s.addText(label, { x, y, w, h: 0.42, fontSize: 12, bold: true, color: fg, align: "center", valign: "middle", fontFace: "Calibri" });
}
// ═════════════════════════════════════════════════════════════════════════════
// BUILD PRESENTATION
// ═════════════════════════════════════════════════════════════════════════════
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Burst Abdomen: Management & Retention Suturing";
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 1 — Title
// ─────────────────────────────────────────────────────────────────────────────
{
const s = darkSlide(pres);
// Red diagonal accent
s.addShape(pres.shapes.RECTANGLE, { x: 6.8, y: 0, w: 3.2, h: 5.625, fill: { color: C.accent, transparency: 80 } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 4.5, w: 10, h: 1.125, fill: { color: C.accent, transparency: 60 } });
s.addText("BURST ABDOMEN", {
x: 0.5, y: 0.6, w: 9, h: 1.1,
fontSize: 52, bold: true, color: C.white, fontFace: "Calibri",
charSpacing: 6,
});
s.addText("Management & Retention Suturing Technique", {
x: 0.5, y: 1.75, w: 9, h: 0.6,
fontSize: 22, color: C.lightBlue, fontFace: "Calibri", italic: true,
});
// Horizontal rule
s.addShape(pres.shapes.RECTANGLE, { x: 0.5, y: 2.45, w: 5, h: 0.04, fill: { color: C.accentGold } });
s.addText([
{ text: "Surgical Management Seminar", options: { breakLine: true } },
{ text: "Retention Sutures • Secondary Closure • Wound Dehiscence", options: {} },
], {
x: 0.5, y: 2.6, w: 8.5, h: 0.8,
fontSize: 14, color: C.lightBlue, fontFace: "Calibri",
});
s.addText("Sources: Bailey & Love 28e • Current Surgical Therapy 14e • Sabiston 21e • Pye's Surgical Handicraft", {
x: 0, y: 5.3, w: 10, h: 0.28,
fontSize: 8, color: C.subtleGray, align: "center", fontFace: "Calibri",
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 2 — Overview / Contents
// ─────────────────────────────────────────────────────────────────────────────
{
const s = darkSlide(pres);
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.35, h: 5.625, fill: { color: C.accentGold } });
s.addText("PRESENTATION OUTLINE", {
x: 0.6, y: 0.3, w: 9, h: 0.6,
fontSize: 26, bold: true, color: C.white, fontFace: "Calibri", charSpacing: 3,
});
const topics = [
["01", "Definition & Epidemiology"],
["02", "Risk Factors"],
["03", "Clinical Presentation"],
["04", "Pre-operative Management"],
["05", "Surgical Anatomy — Abdominal Wall Layers"],
["06", "Retention Suturing — Technique Step by Step"],
["07", "Suture Configurations (Diagrams)"],
["08", "Complications & Post-operative Care"],
["09", "Evidence & Summary"],
];
topics.forEach(([num, title], i) => {
const col = i < 5 ? 0 : 1;
const row = i < 5 ? i : i - 5;
const x = col === 0 ? 0.6 : 5.3;
const y = 1.1 + row * 0.82;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x, y, w: 4.4, h: 0.64, fill: { color: C.midBlue, transparency: 30 }, rectRadius: 0.05 });
s.addShape(pres.shapes.RECTANGLE, { x, y, w: 0.52, h: 0.64, fill: { color: C.accent } });
s.addText(num, { x, y, w: 0.52, h: 0.64, fontSize: 15, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri" });
s.addText(title, { x: x + 0.58, y, w: 3.8, h: 0.64, fontSize: 13, color: C.lightBlue, valign: "middle", fontFace: "Calibri" });
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 3 — Section: Definition & Epidemiology
// ─────────────────────────────────────────────────────────────────────────────
{
const s = darkSlide(pres);
sectionHeader(s, pres, "Definition &\nEpidemiology", "Section 01");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 4 — Definition content
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
slideHeader(s, pres, "Burst Abdomen — Definition & Epidemiology");
// Definition box
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 0.85, w: 9.3, h: 1.2,
fill: { color: C.midBlue },
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.15 },
});
s.addText([
{ text: "DEFINITION: ", options: { bold: true, color: C.accentGold } },
{ text: "Burst abdomen (abdominal wound dehiscence) is full or partial disruption of any or all layers of an abdominal wound, with or without evisceration of abdominal contents.", options: { color: C.white } },
], { x: 0.5, y: 0.92, w: 9, h: 1.05, fontSize: 14, fontFace: "Calibri" });
// Stats row
const stats = [
["Up to 3%", "Incidence in\nabdominal wounds"],
["Days 5–8", "Peak timing\npost-operatively"],
["10–40%", "Associated\nmortality"],
["\"Pink fluid\"", "Classic\nwarning sign"],
];
stats.forEach(([num, label], i) => {
const x = 0.35 + i * 2.35;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x, y: 2.2, w: 2.15, h: 1.6,
fill: { color: C.white },
shadow: { type: "outer", color: "000000", blur: 5, offset: 2, angle: 135, opacity: 0.12 },
rectRadius: 0.08,
});
s.addShape(pres.shapes.RECTANGLE, { x, y: 2.2, w: 2.15, h: 0.45, fill: { color: C.accent } });
s.addText(num, { x, y: 2.22, w: 2.15, h: 0.42, fontSize: 18, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri" });
s.addText(label, { x, y: 2.68, w: 2.15, h: 1.08, fontSize: 13, color: C.textDark, align: "center", valign: "middle", fontFace: "Calibri" });
});
// Pathophysiology note
s.addText([
{ text: "Key mechanism: ", options: { bold: true, color: C.accent } },
{ text: "Increased collagenolytic activity within 0.5–0.75 cm of wound edge causes suture cut-through. Wound tensile strength is at its lowest on days 5–8 post-op.", options: { color: C.textDark } },
], { x: 0.35, y: 3.95, w: 9.3, h: 0.75, fontSize: 13, fontFace: "Calibri" });
footer(s, "Bailey & Love's Short Practice of Surgery, 28th ed. • Current Surgical Therapy, 14th ed.");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 5 — Risk Factors
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
slideHeader(s, pres, "Risk Factors for Burst Abdomen");
// Systemic column
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 0.85, w: 4.35, h: 0.42, fill: { color: C.midBlue } });
s.addText("SYSTEMIC", { x: 0.35, y: 0.85, w: 4.35, h: 0.42, fontSize: 14, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri" });
const systemic = ["Malnutrition / hypoalbuminaemia", "Diabetes mellitus", "Obesity", "Malignancy", "Steroid / immunosuppressive therapy", "Renal failure / jaundice", "Sepsis", "Advanced age"];
systemic.forEach((item, i) => {
const bg = i % 2 === 0 ? C.white : C.lightBlue;
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 1.27 + i * 0.51, w: 4.35, h: 0.49, fill: { color: bg } });
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 1.27 + i * 0.51, w: 0.1, h: 0.49, fill: { color: C.accent } });
s.addText(item, { x: 0.55, y: 1.27 + i * 0.51, w: 4.1, h: 0.49, fontSize: 12.5, color: C.textDark, valign: "middle", fontFace: "Calibri" });
});
// Local column
s.addShape(pres.shapes.RECTANGLE, { x: 5.25, y: 0.85, w: 4.35, h: 0.42, fill: { color: C.accent } });
s.addText("LOCAL / TECHNICAL", { x: 5.25, y: 0.85, w: 4.35, h: 0.42, fontSize: 14, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri" });
const local = ["Poor closure technique / inadequate bites", "Wound infection / haematoma / seroma", "Raised intra-abdominal pressure", "Post-op coughing (COPD, chest infection)", "Bowel obstruction / ileus", "Contaminated / emergency surgery", "Fascial ischaemia", "Suture cut-through"];
local.forEach((item, i) => {
const bg = i % 2 === 0 ? C.white : C.lightBlue;
s.addShape(pres.shapes.RECTANGLE, { x: 5.25, y: 1.27 + i * 0.51, w: 4.35, h: 0.49, fill: { color: bg } });
s.addShape(pres.shapes.RECTANGLE, { x: 5.25, y: 1.27 + i * 0.51, w: 0.1, h: 0.49, fill: { color: C.midBlue } });
s.addText(item, { x: 5.45, y: 1.27 + i * 0.51, w: 4.1, h: 0.49, fontSize: 12.5, color: C.textDark, valign: "middle", fontFace: "Calibri" });
});
footer(s, "Bailey & Love's Short Practice of Surgery, 28th ed.");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 6 — Clinical Presentation + Photo
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
slideHeader(s, pres, "Clinical Presentation");
// Left content
s.addText("Warning Signs", { x: 0.35, y: 0.9, w: 4.8, h: 0.45, fontSize: 16, bold: true, color: C.accent, fontFace: "Calibri" });
const warnings = [
["🩸", "Serosanguinous (\"salmon-pink\") discharge", "CLASSIC — often 24–48 h before burst"],
["💥", "\"Popping\" or \"giving way\" sensation", "During coughing, straining, movement"],
["👁", "Visible wound gap", "Partial to complete separation"],
["🫀", "Exposed bowel / omentum (evisceration)", "Surgical EMERGENCY — cover immediately"],
];
warnings.forEach(([icon, title, sub], i) => {
const y = 1.45 + i * 0.9;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 0.35, y, w: 4.8, h: 0.78,
fill: { color: i === 3 ? "FFF0EE" : C.white },
shadow: { type: "outer", color: "000000", blur: 4, offset: 1, angle: 135, opacity: 0.1 },
rectRadius: 0.05,
});
if (i === 3) s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y, w: 0.1, h: 0.78, fill: { color: C.accent } });
else s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y, w: 0.1, h: 0.78, fill: { color: C.midBlue } });
s.addText(title, { x: 0.55, y: y + 0.04, w: 4.55, h: 0.35, fontSize: 13, bold: true, color: C.textDark, fontFace: "Calibri" });
s.addText(sub, { x: 0.55, y: y + 0.38, w: 4.55, h: 0.32, fontSize: 11, color: C.textMid, fontFace: "Calibri", italic: true });
});
// Right — clinical photo
s.addText("Clinical Photo: Complete Fascial Dehiscence", {
x: 5.4, y: 0.88, w: 4.2, h: 0.38,
fontSize: 12, bold: true, color: C.midBlue, fontFace: "Calibri", align: "center",
});
if (imgDehiscence) {
s.addImage({ data: imgDehiscence, x: 5.55, y: 1.3, w: 3.9, h: 3.6 });
}
s.addText("Complete fascial dehiscence with exposed bowel — requires urgent return to theatre", {
x: 5.3, y: 4.95, w: 4.4, h: 0.38,
fontSize: 9, color: C.subtleGray, align: "center", italic: true, fontFace: "Calibri",
});
footer(s, "Current Surgical Therapy, 14th ed. Fig. 7 — Complete fascial dehiscence after failure of primary closure");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 7 — Pre-operative Management
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
slideHeader(s, pres, "Pre-operative Management");
const steps = [
{ num: "1", title: "Cover the wound", body: "Moist warm saline-soaked packs over any eviscerated bowel. Do NOT attempt to push bowel back in.", color: C.accent },
{ num: "2", title: "NBM + IV Access", body: "Nil by mouth immediately. Establish wide-bore IV access. IV fluids for resuscitation.", color: C.midBlue },
{ num: "3", title: "Antibiotics", body: "Broad-spectrum IV antibiotics (e.g. co-amoxiclav or cefuroxime + metronidazole).", color: C.midBlue },
{ num: "4", title: "Correct deficiencies", body: "Correct electrolyte imbalances. Treat hypoglycaemia. Optimise coagulation.", color: C.midBlue },
{ num: "5", title: "Anaesthetic review", body: "General anaesthesia + full muscle relaxation mandatory. Spinal/local is INADEQUATE.", color: C.accent },
{ num: "6", title: "Consent & Theatre", body: "Explain procedure. Book urgent theatre. If evisceration is present — EMERGENCY slot.", color: C.accent },
];
steps.forEach((step, i) => {
const col = i % 2 === 0 ? 0 : 1;
const row = Math.floor(i / 2);
const x = 0.35 + col * 4.85;
const y = 0.88 + row * 1.5;
s.addShape(pres.shapes.RECTANGLE, { x, y, w: 4.55, h: 1.35,
fill: { color: C.white },
shadow: { type: "outer", color: "000000", blur: 5, offset: 2, angle: 135, opacity: 0.1 },
});
s.addShape(pres.shapes.RECTANGLE, { x, y, w: 0.55, h: 1.35, fill: { color: step.color } });
s.addText(step.num, { x, y, w: 0.55, h: 1.35, fontSize: 22, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri" });
s.addText(step.title, { x: x + 0.62, y: y + 0.08, w: 3.85, h: 0.38, fontSize: 14, bold: true, color: step.color, fontFace: "Calibri" });
s.addText(step.body, { x: x + 0.62, y: y + 0.46, w: 3.85, h: 0.82, fontSize: 12, color: C.textDark, fontFace: "Calibri" });
});
footer(s, "Tintinalli's Emergency Medicine • Bailey & Love's Surgery 28e");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 8 — Section: Anatomy
// ─────────────────────────────────────────────────────────────────────────────
{
const s = darkSlide(pres);
sectionHeader(s, pres, "Surgical Anatomy\nof the Abdominal Wall", "Section 05 — Understanding the Layers");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 9 — Anatomy layers diagram
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
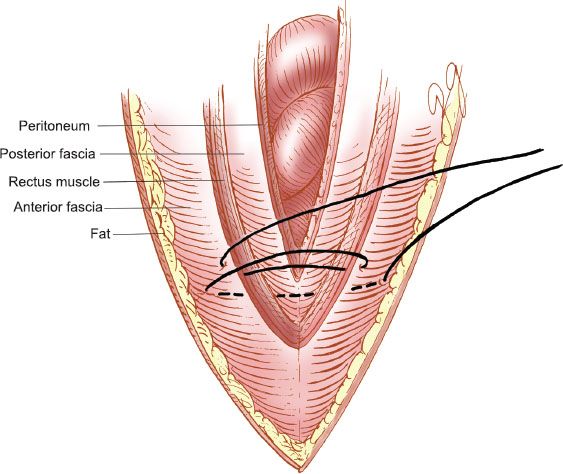
slideHeader(s, pres, "Abdominal Wall — Layers Traversed by Retention Sutures");
if (imgAnatomy) {
s.addImage({ data: imgAnatomy, x: 0.35, y: 0.85, w: 4.0, h: 4.2 });
}
s.addText("Anatomical Layers (deep to superficial):", {
x: 4.6, y: 0.88, w: 5.0, h: 0.38,
fontSize: 14, bold: true, color: C.midBlue, fontFace: "Calibri",
});
const layers = [
["1", "Peritoneum", "Serous lining — optional to close", C.accent],
["2", "Posterior rectus sheath", "Below arcuate line — merges with transversalis fascia", C.midBlue],
["3", "Rectus abdominis muscle", "Segmental innervation (T7–T12)", C.midBlue],
["4", "Anterior rectus sheath", "Main tensile layer — must be included in retention suture", C.accent],
["5", "Subcutaneous fat", "Variable depth; poor tensile strength", C.midBlue],
["6", "Skin", "Full-thickness external retention suture exits here", C.midBlue],
];
layers.forEach((layer, i) => {
const y = 1.35 + i * 0.67;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 4.6, y, w: 5.0, h: 0.58,
fill: { color: i % 2 === 0 ? C.lightBlue : C.white }, rectRadius: 0.04,
});
s.addShape(pres.shapes.RECTANGLE, { x: 4.6, y, w: 0.38, h: 0.58, fill: { color: layer[3] } });
s.addText(layer[0], { x: 4.6, y, w: 0.38, h: 0.58, fontSize: 14, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri" });
s.addText(layer[1], { x: 5.04, y: y + 0.03, w: 3.8, h: 0.25, fontSize: 12, bold: true, color: C.textDark, fontFace: "Calibri" });
s.addText(layer[2], { x: 5.04, y: y + 0.28, w: 3.8, h: 0.24, fontSize: 10, color: C.textMid, italic: true, fontFace: "Calibri" });
});
footer(s, "Retention sutures pass through ALL 6 layers (full-thickness) or layers 2–4 (internal/extraperitoneal)");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 10 — Abdominal wall layered closure diagram
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
slideHeader(s, pres, "Layered Abdominal Wall Closure — Context for Retention Sutures");
if (imgLayers) {
s.addImage({ data: imgLayers, x: 0.5, y: 0.88, w: 5.5, h: 4.1 });
}
s.addText("Closure Sequence:", { x: 6.25, y: 0.9, w: 3.4, h: 0.38, fontSize: 14, bold: true, color: C.midBlue, fontFace: "Calibri" });
const seq = [
["A", "Peritoneum (optional)"],
["B", "Muscle (rarely separate)"],
["C", "Anterior fascia — KEY layer"],
["D", "Subcutaneous tissue"],
["E", "Skin — loosely approximated"],
["F", "With external retention sutures"],
];
seq.forEach(([ltr, desc], i) => {
s.addShape(pres.shapes.RECTANGLE, { x: 6.25, y: 1.36 + i * 0.56, w: 3.4, h: 0.5,
fill: { color: ltr === "C" || ltr === "F" ? "FFF0EE" : (i % 2 === 0 ? C.white : C.lightBlue) },
});
if (ltr === "C" || ltr === "F") {
s.addShape(pres.shapes.RECTANGLE, { x: 6.25, y: 1.36 + i * 0.56, w: 0.06, h: 0.5, fill: { color: C.accent } });
}
s.addText(ltr, { x: 6.28, y: 1.36 + i * 0.56, w: 0.38, h: 0.5, fontSize: 14, bold: true, color: C.accent, valign: "middle", fontFace: "Calibri" });
s.addText(desc, { x: 6.7, y: 1.36 + i * 0.56, w: 2.9, h: 0.5, fontSize: 12, color: C.textDark, valign: "middle", fontFace: "Calibri" });
});
footer(s, "Mass closure (single fascial layer, continuous) is now preferred over layered closure");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 11 — Section: Retention Suturing
// ─────────────────────────────────────────────────────────────────────────────
{
const s = darkSlide(pres);
sectionHeader(s, pres, "Retention Suturing\nTechnique", "Section 06 — Step-by-Step Operative Guide");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 12 — What Are Retention Sutures
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
slideHeader(s, pres, "Retention Sutures — What, Why, and When");
// Large definition box
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 0.85, w: 9.3, h: 1.05, fill: { color: C.midBlue } });
s.addText([
{ text: "DEFINITION: ", options: { bold: true, color: C.accentGold } },
{ text: "Heavy, non-absorbable, full-thickness sutures placed through all layers of the abdominal wall — lateral to, and across, the primary fascial closure line — to prevent evisceration if the fascial repair fails.", options: { color: C.white } },
], { x: 0.5, y: 0.92, w: 9, h: 0.9, fontSize: 14, fontFace: "Calibri" });
// CRITICAL box
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 2.05, w: 9.3, h: 0.78, fill: { color: C.accent, transparency: 15 } });
s.addText([
{ text: "⚠ CRITICAL DISTINCTION: ", options: { bold: true, color: C.white } },
{ text: "Retention sutures do NOT prevent fascial dehiscence.", options: { bold: true, color: C.accentGold } },
{ text: " They prevent EVISCERATION if the fascial closure fails.", options: { color: C.white } },
], { x: 0.5, y: 2.1, w: 9, h: 0.65, fontSize: 14, fontFace: "Calibri" });
// Three indication boxes
const cards = [
["WHEN TO USE", "High-risk patients at secondary closure:\nMalnutrition • Malignancy • Sepsis\nEmergency surgery • Obesity • Steroids", C.accent],
["TYPES", "External (full thickness — through skin)\nInternal (extraperitoneal — subfascial)\nBoth placed 3–4 cm from fascial edge", C.midBlue],
["TIMING OF\nREMOVAL", "After 6–8 weeks\nOnly once skin wound has been well healed for at least 3–4 weeks", C.midBlue],
];
cards.forEach((card, i) => {
const x = 0.35 + i * 3.15;
s.addShape(pres.shapes.RECTANGLE, { x, y: 2.98, w: 3.0, h: 2.12,
fill: { color: C.white },
shadow: { type: "outer", color: "000000", blur: 5, offset: 2, angle: 135, opacity: 0.12 },
});
s.addShape(pres.shapes.RECTANGLE, { x, y: 2.98, w: 3.0, h: 0.5, fill: { color: card[2] } });
s.addText(card[0], { x, y: 2.98, w: 3.0, h: 0.5, fontSize: 12, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri" });
s.addText(card[1], { x: x + 0.1, y: 3.53, w: 2.8, h: 1.52, fontSize: 12, color: C.textDark, fontFace: "Calibri" });
});
footer(s, "Current Surgical Therapy, 14th ed. p. 1422 • Sabiston Textbook of Surgery p. 2059");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 13 — Step-by-step technique (Steps 1–3)
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
slideHeader(s, pres, "Operative Technique — Steps 1 to 3");
const steps = [
{
n: "01",
title: "Anaesthesia & Theatre Setup",
color: C.accent,
points: [
"General anaesthesia — MANDATORY",
"Full muscle relaxation required to approximate retracted fascia",
"Cannot be done under local or spinal anaesthesia",
"IV broad-spectrum antibiotics pre-operatively",
"Supine position; full sterile prep and draping",
],
},
{
n: "02",
title: "Wound Exploration & Debridement",
color: C.midBlue,
points: [
"Open the entire skin incision",
"Trace fascial suture back to intact, non-dehisced fascia at both ends",
"Debride ALL non-viable, infected, or necrotic tissue at fascial edges",
"Fresh, bleeding fascia must be exposed for a good suture bite",
"Anatomy must be clearly identified before closure",
],
},
{
n: "03",
title: "Abdominal Exploration & Lavage",
color: C.midBlue,
points: [
"Purulent / feculent / bilious discharge → FIND & MANAGE the source",
"Gentle downward bowel pressure for limited visualisation if wound is clean",
"Lavage peritoneal cavity with warm normal saline (2–3 litres)",
"Limit exploration if clean — avoid iatrogenic bowel injury",
"Remove all loose necrotic material",
],
},
];
steps.forEach((step, i) => {
const y = 0.88 + i * 1.52;
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y, w: 9.3, h: 1.38,
fill: { color: C.white },
shadow: { type: "outer", color: "000000", blur: 4, offset: 2, angle: 135, opacity: 0.08 },
});
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y, w: 0.75, h: 1.38, fill: { color: step.color } });
s.addText(step.n, { x: 0.35, y, w: 0.75, h: 1.38, fontSize: 24, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri" });
s.addText(step.title, { x: 1.18, y: y + 0.06, w: 8.4, h: 0.38, fontSize: 14, bold: true, color: step.color, fontFace: "Calibri" });
const bullets = step.points.map((p, pi) => ({
text: p,
options: { bullet: true, breakLine: pi < step.points.length - 1, fontSize: 11.5, color: C.textDark, fontFace: "Calibri" },
}));
s.addText(bullets, { x: 1.18, y: y + 0.48, w: 8.35, h: 0.84 });
});
footer(s, "VUMC Global Surgical Atlas — Closure of Laparotomy Wound Dehiscence (Davis R.)");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 14 — Steps 4–5: Placing & Tying the Sutures
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
slideHeader(s, pres, "Operative Technique — Steps 4 & 5: Placing Retention Sutures");
// Step 4 header
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 0.85, w: 9.3, h: 0.45, fill: { color: C.accent } });
s.addText("STEP 04 — Place Retention Sutures FIRST (Before Tying)", { x: 0.4, y: 0.85, w: 9.2, h: 0.45, fontSize: 14, bold: true, color: C.white, valign: "middle", fontFace: "Calibri" });
const specTable = [
["Suture material", "Heavy No. 1 or No. 2 monofilament nylon OR braided nylon / Prolene"],
["Distance from edge", "3–4 cm lateral to the fascial edge (some texts: 4–6 cm)"],
["Spacing", "3–5 cm apart along the wound length"],
["Depth", "Full-thickness: skin → subcutaneous fat → anterior fascia → muscle → posterior fascia → peritoneum"],
["Position", "Extraperitoneal placement preferred — avoids bowel contact & cheese-wire effect"],
["Needle safety", "Malleable retractor protects bowel during each pass — needle ALWAYS in direct vision"],
["Timing", "DO NOT TIE — park sutures until fascia is fully closed"],
];
specTable.forEach(([label, value], i) => {
const bg = i % 2 === 0 ? C.lightBlue : C.white;
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 1.35 + i * 0.42, w: 9.3, h: 0.4, fill: { color: bg } });
s.addText(label, { x: 0.4, y: 1.35 + i * 0.42, w: 2.5, h: 0.4, fontSize: 12, bold: true, color: C.textMid, valign: "middle", fontFace: "Calibri" });
s.addShape(pres.shapes.RECTANGLE, { x: 2.9, y: 1.35 + i * 0.42, w: 0.03, h: 0.4, fill: { color: C.subtleGray } });
s.addText(value, { x: 2.98, y: 1.35 + i * 0.42, w: 6.6, h: 0.4, fontSize: 12, color: C.textDark, valign: "middle", fontFace: "Calibri" });
});
// Step 5 note
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 4.35, w: 9.3, h: 0.65, fill: { color: C.midBlue } });
s.addText([
{ text: "STEP 05 — Fascial Closure: ", options: { bold: true, color: C.accentGold } },
{ text: "Mass closure with large bites of No. 1 Prolene or PDS. Interrupted sutures preferred over continuous in contaminated/high-risk cases — single stitch failure cannot unzip the whole wound.", options: { color: C.white } },
], { x: 0.45, y: 4.37, w: 9.1, h: 0.6, fontSize: 12.5, fontFace: "Calibri" });
footer(s, "Current Surgical Therapy 14e • VUMC Global Surgical Atlas");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 15 — Steps 6–7: Bolster & Skin
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
slideHeader(s, pres, "Operative Technique — Steps 6 & 7: Bolster, Tying & Skin");
// Step 6 block
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 0.85, w: 9.3, h: 0.45, fill: { color: C.midBlue } });
s.addText("STEP 06 — Tie Retention Sutures Over a Bolster", { x: 0.4, y: 0.85, w: 9.2, h: 0.45, fontSize: 14, bold: true, color: C.white, valign: "middle", fontFace: "Calibri" });
const bolsterSteps = [
"Cut sterile IV tubing (or red rubber catheter) into 4–5 cm strips",
"Thread each retention suture through a strip of IV tubing",
"Tie firmly — NO excessive tension. The bolster spreads force over a wide skin area",
"Overtightening causes pressure necrosis, skin breakdown, and wound complications",
"Purpose of bolster: prevents the heavy suture from acting as a 'cheese wire' through skin",
];
bolsterSteps.forEach((item, i) => {
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 1.38 + i * 0.44, w: 9.3, h: 0.42,
fill: { color: i % 2 === 0 ? C.white : C.lightBlue },
});
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 1.38 + i * 0.44, w: 0.4, h: 0.42, fill: { color: C.accent } });
s.addText(String(i + 1), { x: 0.35, y: 1.38 + i * 0.44, w: 0.4, h: 0.42, fontSize: 13, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri" });
s.addText(item, { x: 0.82, y: 1.38 + i * 0.44, w: 8.76, h: 0.42, fontSize: 12.5, color: C.textDark, valign: "middle", fontFace: "Calibri" });
});
// Step 7 skin
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 3.62, w: 9.3, h: 0.45, fill: { color: C.midBlue } });
s.addText("STEP 07 — Skin Closure", { x: 0.4, y: 3.62, w: 9.2, h: 0.45, fontSize: 14, bold: true, color: C.white, valign: "middle", fontFace: "Calibri" });
const skinNotes = [
["Clean wound", "Loose interrupted sutures or clips — never close tightly"],
["Infected wound", "Leave skin OPEN — pack with saline-soaked gauze"],
["Deep contamination", "Consider superficial subcutaneous drain"],
["Ostomy present", "Place retention sutures ≥3 cm from stoma edge to preserve appliance adherence"],
];
skinNotes.forEach(([type, note], i) => {
const x = 0.35 + (i % 2) * 4.7;
const y = 4.15 + Math.floor(i / 2) * 0.55;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x, y, w: 4.5, h: 0.48,
fill: { color: i === 1 ? "FFF0EE" : C.white }, rectRadius: 0.04,
});
s.addText([
{ text: type + ": ", options: { bold: true, color: C.accent } },
{ text: note, options: { color: C.textDark } },
], { x: x + 0.1, y, w: 4.3, h: 0.48, fontSize: 12, valign: "middle", fontFace: "Calibri" });
});
footer(s, "VUMC Global Surgical Atlas • Bailey & Love's Surgery 28e");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 16 — Section: Suture Configurations
// ─────────────────────────────────────────────────────────────────────────────
{
const s = darkSlide(pres);
sectionHeader(s, pres, "Suture Configurations\n& Diagrams", "Section 07 — Cross-Sectional Anatomy of Retention Sutures");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 17 — Cross-sectional configurations diagram
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
slideHeader(s, pres, "Retention Suture Configurations — Cross-Sectional Diagrams");
if (imgConfigs) {
s.addImage({ data: imgConfigs, x: 0.35, y: 0.85, w: 3.5, h: 4.35 });
}
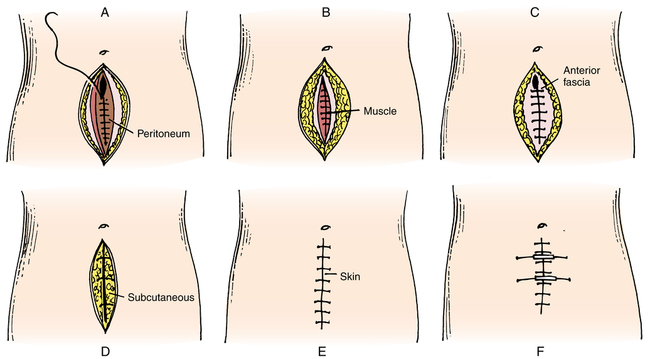
s.addText("Four Configurations:", { x: 4.1, y: 0.9, w: 5.5, h: 0.38, fontSize: 14, bold: true, color: C.midBlue, fontFace: "Calibri" });
const configs = [
{ ltr: "A", name: "Simple Interrupted (Full-Thickness)", desc: "Passes through all layers from skin to peritoneum. Most common. Bolster applied on skin surface.", color: C.accent },
{ ltr: "B", name: "Internal Retention / Smead-Jones Far-Near", desc: "Far-near-near-far suture through fascia only. Skin not included. Avoids surface scarring.", color: C.midBlue },
{ ltr: "C", name: "Modified Mattress", desc: "Horizontal mattress variant with extraperitoneal subfascial component. Spreads tension widely.", color: C.midBlue },
{ ltr: "D", name: "Extraperitoneal 'U' Shape", desc: "Needle enters 10 cm lateral, loops deep through preperitoneal space, exits opposite side. No peritoneal entry.", color: C.midBlue },
];
configs.forEach((cfg, i) => {
const y = 1.36 + i * 1.0;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x: 4.1, y, w: 5.5, h: 0.88,
fill: { color: i % 2 === 0 ? C.lightBlue : C.white }, rectRadius: 0.05,
});
s.addShape(pres.shapes.RECTANGLE, { x: 4.1, y, w: 0.45, h: 0.88, fill: { color: cfg.color } });
s.addText(cfg.ltr, { x: 4.1, y, w: 0.45, h: 0.88, fontSize: 18, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri" });
s.addText(cfg.name, { x: 4.62, y: y + 0.06, w: 4.9, h: 0.3, fontSize: 12.5, bold: true, color: C.textDark, fontFace: "Calibri" });
s.addText(cfg.desc, { x: 4.62, y: y + 0.38, w: 4.9, h: 0.44, fontSize: 11, color: C.textMid, fontFace: "Calibri" });
});
footer(s, "AMA GLOWM Atlas of Operative Surgery — Retention suture cross-sectional configurations");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 18 — All abdominal closure techniques overview
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
slideHeader(s, pres, "Abdominal Closure Techniques — Overview Comparison");
if (imgTechniques) {
s.addImage({ data: imgTechniques, x: 0.35, y: 0.85, w: 9.3, h: 3.5 });
}
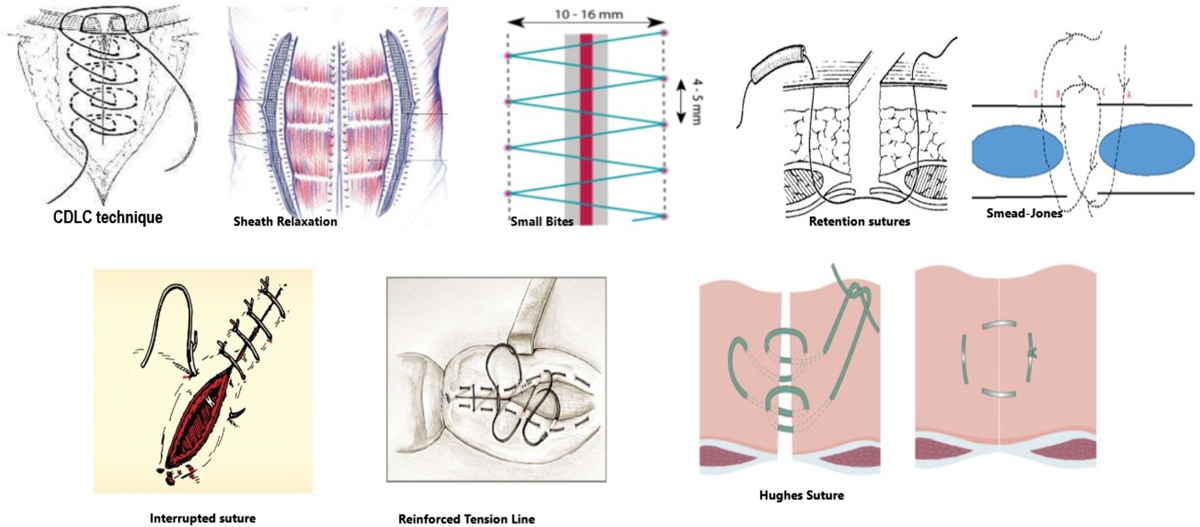
s.addText("Key techniques shown: CDLC, Sheath Relaxation, Small Bites, Retention Sutures, Smead-Jones, Interrupted, Hughes Suture", {
x: 0.35, y: 4.42, w: 9.3, h: 0.35,
fontSize: 11, color: C.textMid, align: "center", italic: true, fontFace: "Calibri",
});
// Highlight box
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y: 4.85, w: 9.3, h: 0.42, fill: { color: C.accent, transparency: 20 } });
s.addText("For burst abdomen secondary suturing: Retention sutures + interrupted mass closure of fascia is the standard", {
x: 0.45, y: 4.87, w: 9.1, h: 0.38, fontSize: 12.5, bold: true, color: C.white, valign: "middle", fontFace: "Calibri",
});
footer(s, "Springer Nature Langenbeck's Archives of Surgery 2023 — Abdominal wall closure techniques");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 19 — Section: Complications
// ─────────────────────────────────────────────────────────────────────────────
{
const s = darkSlide(pres);
sectionHeader(s, pres, "Complications &\nPost-operative Care", "Section 08");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 20 — Complications of Retention Sutures
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
slideHeader(s, pres, "Complications of Retention Sutures");
const complications = [
{ title: "Pressure Necrosis / Skin Breakdown", severity: "HIGH", body: "Heavy suture cuts into skin without a bolster. Use IV tubing / rubber catheter. Avoid overtightening.", color: C.accent },
{ title: "Pain & Discomfort", severity: "HIGH", body: "Constant tension on skin. Patients find these very uncomfortable. Adequate analgesia is essential.", color: C.accent },
{ title: "Raised Intra-Abdominal Pressure", severity: "MOD", body: "Reduces abdominal wall compliance → IAH. Monitor bladder pressure (normal 5–7 mmHg). Remove early if IAH develops.", color: "E8A020" },
{ title: "Bowel Entrapment / Cut-Through", severity: "HIGH", body: "Loop of bowel caught under suture acts as cheese-wire. Keep sutures extraperitoneal. Use malleable retractor.", color: C.accent },
{ title: "Wound Infection & Sinus", severity: "MOD", body: "Foreign body reaction with non-absorbable suture. Strict aseptic technique. Drain early if infection suspected.", color: "E8A020" },
{ title: "Ugly Scar / Ladder Pattern", severity: "LOW", body: "Full-thickness external sutures leave railroad-track scars. Consider internal (subfascial) sutures for cosmesis.", color: "4A9E6B" },
];
complications.forEach((c, i) => {
const col = i % 2;
const row = Math.floor(i / 2);
const x = 0.35 + col * 4.85;
const y = 0.88 + row * 1.55;
s.addShape(pres.shapes.RECTANGLE, { x, y, w: 4.55, h: 1.42,
fill: { color: C.white },
shadow: { type: "outer", color: "000000", blur: 5, offset: 2, angle: 135, opacity: 0.1 },
});
s.addShape(pres.shapes.RECTANGLE, { x, y, w: 0.75, h: 1.42, fill: { color: c.color } });
s.addText(c.severity, { x, y, w: 0.75, h: 1.42, fontSize: 9, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri" });
s.addText(c.title, { x: x + 0.82, y: y + 0.06, w: 3.65, h: 0.38, fontSize: 12.5, bold: true, color: C.textDark, fontFace: "Calibri" });
s.addText(c.body, { x: x + 0.82, y: y + 0.48, w: 3.65, h: 0.88, fontSize: 11, color: C.textMid, fontFace: "Calibri" });
});
footer(s, "PMC6114125 — Effect of retention sutures on abdominal pressure • Current Surgical Therapy 14e");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 21 — Post-operative care
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
slideHeader(s, pres, "Post-operative Care After Secondary Retention Suturing");
const care = [
{ icon: "🥗", title: "Aggressive Nutrition", body: "High-protein diet + multivitamins from day 1. Correct hypoalbuminaemia. Use NG/TPN if oral not tolerated.", highlight: true },
{ icon: "💊", title: "Antibiotics", body: "Continue targeted antibiotics. Wound surveillance daily. Swab if discharge changes character.", highlight: false },
{ icon: "📊", title: "Monitor IAP", body: "Bladder pressure (intra-vesical pressure) monitoring. Normal ≤7 mmHg. IAH (>12 mmHg) → remove sutures early.", highlight: true },
{ icon: "🩹", title: "Skin Care Under Bolsters", body: "Inspect skin under every bolster daily. Early signs: erythema, blanching. Release tension if necrosis starts.", highlight: false },
{ icon: "🫁", title: "Respiratory Physiotherapy", body: "Incentive spirometry. Chest physio for COPD patients. Control post-op coughing (splinting).", highlight: false },
{ icon: "💉", title: "DVT Prophylaxis", body: "LMWH + compression stockings from day 1. Early mobilisation as soon as patient able.", highlight: false },
{ icon: "✂", title: "Suture Removal", body: "Retention sutures: 6–8 weeks minimum. Remove only once skin wound well healed for 3–4 weeks.", highlight: true },
{ icon: "🏥", title: "Long-term", body: "43% develop incisional hernia after burst abdomen. Plan elective hernia repair at 6–12 months if needed.", highlight: false },
];
care.forEach((item, i) => {
const col = i % 2;
const row = Math.floor(i / 2);
const x = 0.3 + col * 4.9;
const y = 0.88 + row * 1.15;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x, y, w: 4.65, h: 1.05,
fill: { color: item.highlight ? "EEF5FF" : C.white },
shadow: { type: "outer", color: "000000", blur: 4, offset: 1, angle: 135, opacity: 0.08 },
rectRadius: 0.05,
});
s.addText(item.title, { x: x + 0.12, y: y + 0.06, w: 4.4, h: 0.3, fontSize: 12.5, bold: true, color: item.highlight ? C.midBlue : C.textDark, fontFace: "Calibri" });
s.addText(item.body, { x: x + 0.12, y: y + 0.38, w: 4.4, h: 0.6, fontSize: 11, color: C.textMid, fontFace: "Calibri" });
});
footer(s, "Bailey & Love 28e • Sabiston Textbook of Surgery • PMC6114125");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 22 — Evidence Summary
// ─────────────────────────────────────────────────────────────────────────────
{
const s = lightSlide(pres);
slideHeader(s, pres, "Evidence Base — Retention Sutures");
s.addText("Key Clinical Trials & Evidence", {
x: 0.35, y: 0.88, w: 9.3, h: 0.4,
fontSize: 16, bold: true, color: C.midBlue, fontFace: "Calibri",
});
const evidence = [
{ study: "Khorgami et al. (2013) RCT — 300 patients", finding: "Dehiscence: 4% (with RS) vs 13.3% (without RS) — p=0.007. Evisceration rates did NOT differ significantly.", type: "FAVOURS", color: "4A9E6B" },
{ study: "Rink et al. (2000) RCT — 95 high-risk patients", finding: "No difference in wound failure rates. Retention sutures associated with significantly increased patient morbidity and discomfort.", type: "NEUTRAL", color: "E8A020" },
{ study: "Gislason et al. (1995) — Burst abdomen closure", finding: "43% developed incisional hernia after resuture. Interrupted sutures: 34% hernia; continuous: 6% hernia. RS did not reduce hernia.", type: "AGAINST", color: C.accent },
{ study: "PMC6114125 (2018) — IAP study", finding: "Retention sutures increase intra-vesical pressure and reduce abdominal wall compliance → risk of IAH in susceptible patients.", type: "CAUTION", color: C.accent },
];
evidence.forEach((ev, i) => {
const y = 1.36 + i * 1.0;
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y, w: 9.3, h: 0.88,
fill: { color: i % 2 === 0 ? C.white : C.lightBlue },
shadow: { type: "outer", color: "000000", blur: 3, offset: 1, angle: 135, opacity: 0.07 },
});
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y, w: 0.9, h: 0.88, fill: { color: ev.color } });
s.addText(ev.type, { x: 0.35, y, w: 0.9, h: 0.88, fontSize: 9, bold: true, color: C.white, align: "center", valign: "middle", fontFace: "Calibri" });
s.addText(ev.study, { x: 1.3, y: y + 0.05, w: 8.3, h: 0.3, fontSize: 12, bold: true, color: C.textDark, fontFace: "Calibri" });
s.addText(ev.finding, { x: 1.3, y: y + 0.38, w: 8.3, h: 0.44, fontSize: 11.5, color: C.textMid, fontFace: "Calibri" });
});
footer(s, "Mixed evidence — routine use not advocated; reserve for selected high-risk patients");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 23 — Summary / Key Take-Home Points
// ─────────────────────────────────────────────────────────────────────────────
{
const s = darkSlide(pres);
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 0.35, h: 5.625, fill: { color: C.accentGold } });
s.addText("KEY TAKE-HOME POINTS", {
x: 0.6, y: 0.22, w: 9, h: 0.55,
fontSize: 26, bold: true, color: C.white, fontFace: "Calibri", charSpacing: 3,
});
s.addShape(pres.shapes.RECTANGLE, { x: 0.6, y: 0.82, w: 8.5, h: 0.04, fill: { color: C.accentGold } });
const points = [
["⚡", "Burst abdomen is a surgical emergency — occurs days 5–8; warning sign is salmon-pink wound discharge"],
["🎯", "Retention sutures PREVENT EVISCERATION — they do NOT prevent fascial dehiscence"],
["📐", "Placement: No. 1–2 nylon, 3–4 cm from edge, 3–5 cm apart, full-thickness, extraperitoneal"],
["🔒", "Always tie over a bolster (IV tubing) — NEVER overtighten"],
["🔑", "Place sutures FIRST, close fascia NEXT, THEN tie the retention sutures"],
["🥗", "Nutrition is as important as the surgical technique — treat malnutrition aggressively"],
["⏱", "Remove after 6–8 weeks — only once skin fully healed for 3–4 weeks"],
["📊", "Evidence is mixed — trend away from routine use; reserve for truly high-risk patients"],
];
points.forEach((pt, i) => {
const col = i < 4 ? 0 : 1;
const row = i < 4 ? i : i - 4;
const x = col === 0 ? 0.6 : 5.35;
const y = 1.0 + row * 1.1;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x, y, w: 4.55, h: 0.95,
fill: { color: C.midBlue, transparency: 30 }, rectRadius: 0.06,
});
s.addShape(pres.shapes.RECTANGLE, { x, y, w: 0.52, h: 0.95, fill: { color: i < 2 ? C.accent : C.midBlue, transparency: 0 } });
s.addText(pt[0], { x, y, w: 0.52, h: 0.95, fontSize: 18, align: "center", valign: "middle", fontFace: "Calibri" });
s.addText(pt[1], { x: x + 0.58, y, w: 3.9, h: 0.95, fontSize: 12, color: C.white, valign: "middle", fontFace: "Calibri" });
});
s.addText("Sources: Bailey & Love 28e • Current Surgical Therapy 14e • Sabiston 21e • Pye's 22e • Khorgami 2013 RCT • PMC6114125", {
x: 0, y: 5.32, w: 10, h: 0.25,
fontSize: 8, color: C.subtleGray, align: "center", fontFace: "Calibri",
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 24 — Video Resources
// ─────────────────────────────────────────────────────────────────────────────
{
const s = darkSlide(pres);
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.75, fill: { color: C.accent } });
s.addText("VIDEO RESOURCES", {
x: 0.4, y: 0.1, w: 9.2, h: 0.55,
fontSize: 26, bold: true, color: C.white, fontFace: "Calibri", charSpacing: 4,
});
s.addText("Scan or click to watch — recommended for seminar demonstration", {
x: 0.4, y: 0.82, w: 9.2, h: 0.35,
fontSize: 13, color: C.lightBlue, fontFace: "Calibri", italic: true,
});
const videos = [
{ title: "Secondary Suturing for Burst Abdomen", author: "Dr Jay Mehta — Cancer Surgeon", url: "https://www.youtube.com/watch?v=t4TsctmZE-E", note: "⭐ MOST RELEVANT — live operative technique", highlight: true },
{ title: "Retention Sutures (Mass Closure) — Burst Abdomen", author: "Surgical Anatomy Channel", url: "https://www.youtube.com/watch?v=XqHJNH7WmE0", note: "Anatomy + retention suture placement", highlight: false },
{ title: "How to Apply Retention Sutures", author: "Dr Tayyab Riaz Ch", url: "https://www.youtube.com/watch?v=i7hKwsAM6dw", note: "Step-by-step focused tutorial", highlight: false },
{ title: "Abdominal Wall Closure — Mass Closure & Jenkins' Rule", author: "Prof. Chintamani", url: "https://www.youtube.com/watch?v=_FHJK3lAABM", note: "Mass closure technique with retention sutures", highlight: false },
];
videos.forEach((v, i) => {
const y = 1.3 + i * 1.0;
s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y, w: 9.3, h: 0.88,
fill: { color: v.highlight ? C.accent : C.midBlue, transparency: v.highlight ? 15 : 40 },
});
if (v.highlight) s.addShape(pres.shapes.RECTANGLE, { x: 0.35, y, w: 0.1, h: 0.88, fill: { color: C.accentGold } });
s.addText([
{ text: v.title, options: { bold: true, color: C.white, breakLine: true } },
{ text: v.author + " | " + v.note, options: { color: C.lightBlue } },
], { x: 0.55, y: y + 0.1, w: 6.8, h: 0.7, fontSize: 13, fontFace: "Calibri" });
// URL as hyperlink text
s.addText(v.url.replace("https://www.youtube.com/watch?v=", "youtu.be/"), {
x: 7.4, y: y + 0.22, w: 2.2, h: 0.44,
fontSize: 9, color: C.accentGold, italic: true, fontFace: "Calibri",
hyperlink: { url: v.url },
});
});
footer(s, "All links verified — YouTube publicly available content");
}
// ─────────────────────────────────────────────────────────────────────────────
// WRITE FILE
// ─────────────────────────────────────────────────────────────────────────────
const outPath = "/home/daytona/workspace/burst-abdomen-ppt/Burst_Abdomen_Retention_Suturing.pptx";
pres.writeFile({ fileName: outPath }).then(() => {
console.log("✅ Presentation written to: " + outPath);
}).catch(err => {
console.error("❌ Error:", err);
process.exit(1);
});
cd /home/daytona/workspace/burst-abdomen-ppt && node build.js 2>&1
cd /home/daytona/workspace/burst-abdomen-ppt && node -e " const { execSync } = require('child_process'); const fs = require('fs'); const urls = [ 'https://cdn.orris.care/cdss_images/49fc1f3c6f0d85667052744536224df2f9cd16ebec6f0068079c586f40e36fca.png', 'https://basicmedicalkey.com/wp-content/uploads/2017/04/B9780323073585000371_f28-09af-9780323073585.jpg', 'https://resources.ama.uk.com/glowm_www/graphics/figures/v1/0560/008f.gif', 'https://media.springernature.com/lw1200/springer-static/image/art%3A10.1007%2Fs00423-023-02954-w/MediaObjects/423_2023_2954_Fig2_HTML.png', 'https://oncohemakey.com/wp-content/uploads/2016/12/image01770.jpeg', ]; urls.forEach((url, i) => { try { const result = JSON.parse(execSync(\`node /home/daytona/skills/shared/scripts/fetch_images.js \"\${url}\"\`).toString()); const b64 = result[0].base64; const ext = b64.startsWith('image/png') ? 'png' : b64.startsWith('image/gif') ? 'gif' : 'jpg'; fs.writeFileSync(\`img\${i}.\${ext}\`, b64); console.log('OK img' + i + '.' + ext + ' (' + b64.length + ' chars)'); } catch(e) { console.log('FAIL img' + i + ': ' + e.message.substring(0,80)); } }); " 2>&1
~/burst-abdomen-ppt/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/burst-abdomen-ppt/build.js'
~/burst-abdomen-ppt/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/burst-abdomen-ppt/build.js'
cd /home/daytona/workspace/burst-abdomen-ppt && node build.js 2>&1
ls -lh /home/daytona/workspace/burst-abdomen-ppt/Burst_Abdomen_Retention_Suturing.pptx
Burst Abdomen Retention Suturing
Presentation · PPTX
Burst Abdomen Retention Suturing
Presentation · PPTX
What's inside (24 slides):
| # | Slide |
|---|---|
| 1 | Title slide - dark blue/crimson theme |
| 2 | Outline - 9 numbered topic cards |
| 3 | Section divider - Definition & Epidemiology |
| 4 | Definition & Epidemiology - stat cards (3%, days 5-8, 10-40% mortality) |
| 5 | Risk Factors - dual-column table (systemic vs local) |
| 6 | Clinical Presentation - warning signs + clinical photo of fascial dehiscence |
| 7 | Pre-operative Management - 6-step action grid |
| 8 | Section divider - Surgical Anatomy |
| 9 | Anatomy - layers diagram + labeled layer table |
| 10 | Layered closure context - closure sequence diagram |
| 11 | Section divider - Retention Suturing |
| 12 | What are retention sutures + critical distinction box |
| 13 | Operative steps 1-3 (GA, exploration, lavage) |
| 14 | Operative steps 4-5 (suture placement specs + fascial closure) |
| 15 | Operative steps 6-7 (bolster tying, skin closure) |
| 16 | Section divider - Configurations & Diagrams |
| 17 | Cross-sectional configurations A-D with diagram |
| 18 | All closure techniques overview - Springer Nature diagram |
| 19 | Section divider - Complications |
| 20 | Complications - 6 cards with severity tags |
| 21 | Post-operative care - 8 care domains |
| 22 | Evidence summary - 4 key trials (Khorgami, Rink, Gislason, PMC6114125) |
| 23 | Key take-home points - 8 summary cards |
| 24 | Video resources - 4 YouTube links with hyperlinks |