
Screenshot_20260603-131559.png
Solve with reason
Answer: B) Decreased venous return (preload)
Reasoning:
The scenario describes the Valsalva maneuver - forcefully contracting skeletal muscles while holding the breath (straining against a closed glottis).
Here is the hemodynamic chain of events:
-
Breath-holding + forceful muscle contraction raises intrathoracic pressure dramatically (this rules out option D - intrathoracic pressure actually increases, not decreases).
-
Elevated intrathoracic pressure compresses the great veins (superior and inferior vena cava) entering the thorax.
-
This compression reduces venous return to the right heart - preload drops sharply (option B).
-
By the Frank-Starling mechanism, reduced preload → reduced stroke volume (rules out C - stroke volume decreases, not increases).
-
Reduced stroke volume → decreased cardiac output → decreased mean arterial pressure.
-
The sudden fall in cerebral perfusion pressure causes syncope within seconds.
Why not A (Increased SVR)?
SVR actually reflex-increases (baroreceptor response to the BP drop), but this is a compensatory response - not the primary trigger. The syncope occurs before this compensation can restore adequate perfusion.
Why not D (Decreased intrathoracic pressure)?
The opposite is true - intrathoracic pressure increases during the Valsalva maneuver, which is precisely what compresses the venous system.
The correct answer is B - Decreased venous return (preload) is the primary hemodynamic trigger. The increased intrathoracic pressure mechanically impedes venous return to the heart, dropping cardiac output and cerebral perfusion rapidly enough to cause loss of consciousness.
Also explain the discussed topic in this question
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive textbook information. Let me compile the full explanation.
The Valsalva Maneuver and Syncope - Complete Explanation
Part 1: What is the Valsalva Maneuver?
The Valsalva maneuver is a forced expiration against a closed glottis - meaning you strain hard while NOT letting air escape. It occurs naturally during:
- Heavy weightlifting / muscle flexing (as in the question)
- Coughing
- Defecation / straining on the toilet
- Childbirth pushing
When you forcefully contract all skeletal muscles AND hold your breath simultaneously, you create a powerful Valsalva effect.
Part 2: The 4 Phases of the Valsalva Maneuver
| Phase | What Happens | Blood Pressure | Heart Rate |
|---|---|---|---|
| I - Onset of strain | Intrathoracic pressure rises, mechanically squeezes aorta | Rises briefly | Slight fall |
| II - Sustained strain | Veins compressed → venous return drops → CO drops | Falls progressively | Rises (reflex) |
| III - Release | Intrathoracic pressure falls suddenly, blood pools in pulmonary vessels | Brief further dip | Brief rise |
| IV - Recovery | Venous return normalizes, sympathetic vasoconstriction still active | Overshoots above normal | Slows (baroreceptor reflex) |
In the scenario: The boy is stuck in Phase II - sustained straining. He never reaches Phase IV.
Part 3: The Hemodynamic Chain Leading to Syncope
Here is the exact sequence that causes loss of consciousness:
Forceful muscle contraction + breath-hold
↓
↑ Intrathoracic pressure
↓
Compression of great veins (SVC + IVC)
↓
↓ Venous return to right heart ← PRIMARY TRIGGER (Answer B)
↓
↓ Right ventricular filling (↓ preload)
↓
↓ Right ventricular stroke volume
↓
↓ Pulmonary blood flow
↓
↓ Left ventricular filling
↓
↓ Left ventricular stroke volume (Frank-Starling Law)
↓
↓ Cardiac output
↓
↓ Systemic blood pressure
↓
↓ Cerebral perfusion pressure
↓
SYNCOPE (loss of consciousness in 6-8 seconds)
As confirmed by Harrison's Principles: "Cessation of blood flow for 6-8 s will result in loss of consciousness" and "a fall in systolic blood pressure ~50 mmHg or lower will usually result in syncope."
- Harrison's Principles of Internal Medicine 22E, p. 556
Part 4: The Baroreceptor Reflex - The Body's Emergency Response
When BP drops during the strain, the body tries to fight back via the baroreceptor reflex:
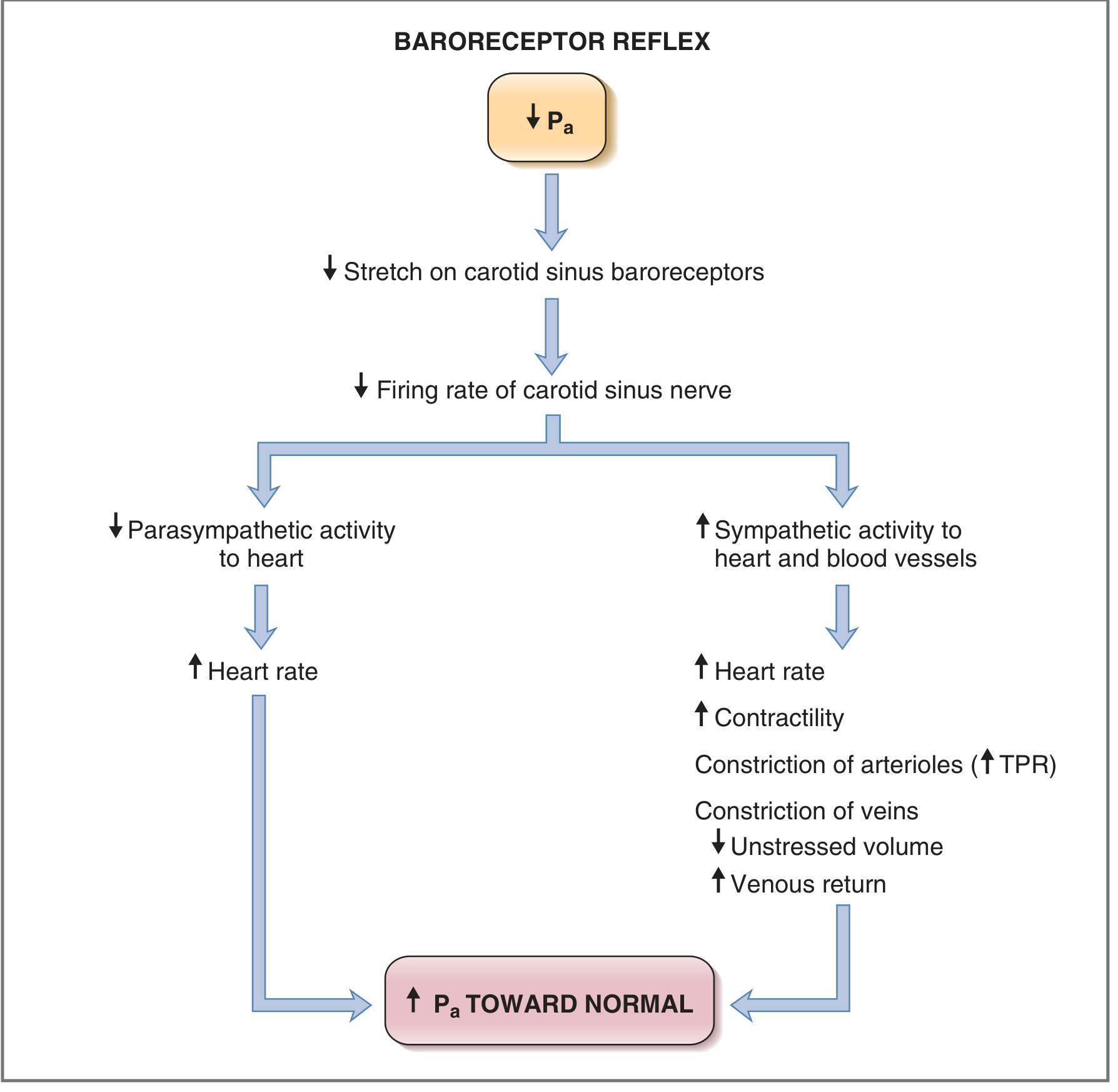
As shown in the diagram (Costanzo Physiology):
- ↓ Arterial pressure → ↓ stretch on carotid sinus baroreceptors
- → ↓ firing of carotid sinus nerve (CN IX)
- → Nucleus tractus solitarius activates ↑ sympathetic + ↓ parasympathetic outflow
- → ↑ Heart rate, ↑ contractility, ↑ TPR (arteriolar constriction), ↑ venous constriction
However, in the scenario - the strain is so sudden and intense that this reflex cannot compensate fast enough before consciousness is lost.
Part 5: Why Each Wrong Answer is Wrong
| Option | Why Wrong |
|---|---|
| A) Increased SVR | SVR actually reflex-increases as a compensatory response to the BP drop - it is the effect, not the cause. And it is trying to help, not hurt. |
| C) Increased stroke volume | Stroke volume decreases because preload drops (Frank-Starling - less filling = less output). |
| D) Decreased intrathoracic pressure | The opposite occurs - intrathoracic pressure dramatically increases during the Valsalva maneuver. This increased pressure is what compresses the veins. |
Part 6: Frank-Starling Law (The Mechanism Behind Option C being Wrong)
The Frank-Starling Law states:
The force of myocardial contraction is proportional to the initial stretch (filling) of the ventricle.
- More filling (preload) → greater stretch of myocardial fibers → stronger contraction → more stroke volume
- Less filling (preload) → less stretch → weaker contraction → less stroke volume
In the Valsalva scenario: preload drops → stroke volume drops (not increases).
Part 7: Syncope - The Clinical Picture
Definition (Harrison's): Syncope is "a form of transient loss of consciousness (TLOC) that is a consequence of global cerebral hypoperfusion."
In this case it is classified as: Situational syncope (a type of neurally-mediated syncope) - triggered by a specific physical maneuver.
Key features:
- Onset within seconds (as described in the question)
- Patient falls backward (sudden, postural collapse)
- Self-terminating - when he falls and straining stops, venous return restores, and consciousness returns
- No seizure activity (though brief myoclonic jerks can occur at onset of syncope - this is NOT a seizure)
Summary in One Sentence
Forceful straining raises intrathoracic pressure → compresses great veins → reduces venous return (preload) → reduces cardiac output by Frank-Starling law → drops blood pressure → drops cerebral perfusion → syncope within seconds.
Sources: Ganong's Review of Medical Physiology 26th Ed. | Costanzo Physiology 7th Ed. | Harrison's Principles of Internal Medicine 22E | Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.