
Solve this mcq with reason as I am preparing for fcps part 1 anesthesiology
Reading File
Finding Sources
Reading File
Reading File
Answer: B) Cor Pulmonale Secondary to COPD
Clinical Reasoning — Mapping Each Clue to the Diagnosis
| Clinical Feature | Pathophysiological Explanation |
|---|---|
| 55-year-old chronic smoker | COPD is the #1 cause of cor pulmonale; smoking is its leading risk factor |
| Gradual dyspnea + dry cough × 2 years | Progressive airflow obstruction in COPD → chronic hypoxia |
| Raised JVP | Right ventricular failure → elevated right-sided filling pressures → raised venous pressure |
| Bilateral leg swelling | Right heart failure → sodium/water retention → peripheral edema |
| Right upper quadrant pain + tender hepatomegaly | Hepatic congestion from raised right atrial pressure (venous backflow) |
| Left parasternal heave | Right ventricular hypertrophy/enlargement — the hallmark sign of cor pulmonale |
Pathophysiology Chain (FCPS High-Yield)
Smoking → COPD → Chronic hypoxia → Hypoxic pulmonary vasoconstriction → Pulmonary arterial hypertension → RV pressure overload → RV hypertrophy (cor pulmonale) → Eventually RV failure
"Cor pulmonale results from pulmonary hypertension due to primary lung parenchymal (e.g., COPD) or vascular disorders. Hypertrophy of both the right ventricle and the right atrium is characteristic; dilation also may be seen when failure supervenes." — Robbins & Kumar Basic Pathology
"The 'blue bloater' phenotype, characterized by chronic airways disease with hypoxemia and hypercapnia, is more likely to have more overt pulmonary vascular disease." — Fuster and Hurst's The Heart, 15th Edition
Why the Other Options Are Wrong
| Option | Why Excluded |
|---|---|
| A) Acute pericarditis | Presents with sharp pleuritic chest pain, friction rub, and ST changes on ECG — none are present here |
| C) Constrictive pericarditis | Also causes raised JVP and hepatomegaly, but no smoking/COPD history, presents with Kussmaul's sign, pericardial knock, and calcification on imaging — not dyspnea × 2 years |
| D) Dilated cardiomyopathy | Causes biventricular failure, but the primary driver here is lung disease, not myocardial disease; no mention of dilated LV or reduced EF |
| E) Pulmonary embolism | Causes acute dyspnea and pleuritic pain, not a 2-year gradual history |
Key Exam Buzzword Clusters for FCPS
- Chronic smoker + gradual dyspnea + bilateral edema + raised JVP + hepatomegaly + left parasternal heave = Cor Pulmonale secondary to COPD
- Left parasternal heave = RV enlargement (the RV pushes the sternum forward)
- The edema in cor pulmonale is partly from hypercapnia-driven renal sodium retention, not just pump failure — making it distinct from left heart failure edema
Also explain the discussed topic
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Here is a comprehensive breakdown of the entire topic — Cor Pulmonale secondary to COPD — organized for FCPS Part 1 preparation.
Cor Pulmonale — Complete Topic Review
1. Definition
Cor pulmonale is right ventricular (RV) hypertrophy and dilation — often culminating in right heart failure — caused by pulmonary hypertension (PH) arising from primary lung disease or pulmonary vascular disease.
Key exclusion: RV enlargement due to left heart failure or congenital heart disease is NOT cor pulmonale — even if PH is present.
Normal mean pulmonary artery pressure = < 20 mmHg. PH is defined as mean PAP > 25 mmHg at rest on right heart catheterization.
2. Causes
| Category | Examples |
|---|---|
| Obstructive lung disease | COPD (most common), bronchiolitis, emphysema |
| Restrictive lung disease | Pulmonary fibrosis, sarcoidosis, kyphoscoliosis |
| Mixed obstructive + restrictive | Cystic fibrosis, combined pulmonary fibrosis & emphysema |
| Pulmonary vascular | Chronic thromboembolic PH (CTEPH), idiopathic PAH |
| Hypoxia without lung disease | High altitude, sleep apnea, obesity hypoventilation |
In the FCPS context: COPD is by far the most common cause.
3. Pathophysiology — The Complete Chain
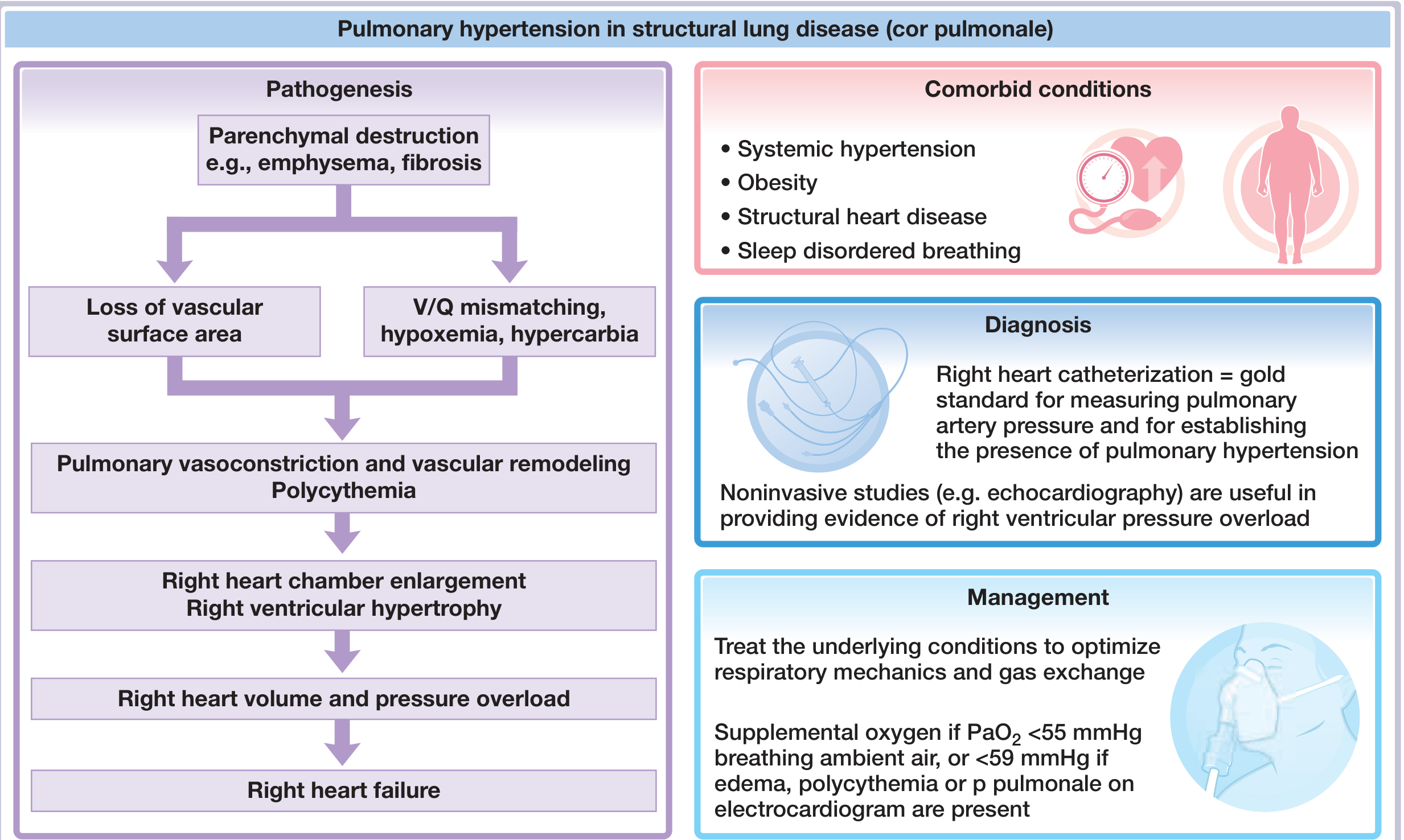
Step-by-step:
① Smoking → COPD
Airway obstruction, parenchymal destruction (emphysema) → loss of alveolar capillary bed → loss of vascular surface area
② V/Q Mismatch → Hypoxemia + Hypercapnia
Poorly ventilated alveoli still receive blood → wasted perfusion → low PaO₂, raised PaCO₂
③ Hypoxic Pulmonary Vasoconstriction (HPV)
The most critical mechanism. Hypoxia causes pulmonary arterioles to constrict (opposite to systemic vessels) — this is a protective reflex to divert blood from poorly ventilated lung, but in COPD it becomes widespread and sustained
④ Pulmonary Vascular Remodeling
Chronic HPV → intimal thickening, medial hypertrophy of pulmonary arteries → fixed, irreversible increase in pulmonary vascular resistance (PVR)
⑤ Polycythemia
Chronic hypoxia → ↑ EPO → ↑ red cell mass → increased blood viscosity → further raises PVR
⑥ Pulmonary Arterial Hypertension (PAH)
Elevated PVR → sustained ↑ pulmonary artery pressure
⑦ RV Pressure Overload → Cor Pulmonale
RV must pump against high resistance → RV hypertrophy (wall thickens) → eventually RV dilation when compensation fails
⑧ Right Heart Failure
RV can no longer maintain output → raised right atrial pressure → systemic venous hypertension → raised JVP, peripheral edema, hepatomegaly
4. Edema in Cor Pulmonale — Why It Happens
This is unique and tested in FCPS:
Edema in cor pulmonale is NOT simply from pump failure (unlike LV failure). Three mechanisms:
- Reduced renal plasma flow → ↓ urinary Na⁺ excretion → Na⁺ and water retention
- Hypercapnia → kidneys compensate for respiratory acidosis by retaining HCO₃⁻ and reabsorbing Na⁺ at the glomerulus
- RAAS activation → aldosterone-driven fluid retention
5. Clinical Features
Symptoms
- Gradual dyspnea on exertion (initially), then at rest
- Dry cough (from underlying COPD)
- Fatigue, reduced exercise tolerance
- Right upper quadrant pain (hepatic capsule distension from congestion)
Signs
| Sign | Mechanism |
|---|---|
| Raised JVP | Right atrial pressure overload → venous congestion |
| Left parasternal heave | RV hypertrophy pushes sternum anteriorly |
| Loud P2 | Pulmonary HTN → forceful pulmonary valve closure |
| Pansystolic murmur at left sternal edge | Tricuspid regurgitation from dilated RV annulus |
| Bilateral pitting edema | Systemic venous congestion + Na retention |
| Tender hepatomegaly | Hepatic venous congestion |
| Cyanosis | Chronic hypoxemia |
Left parasternal heave = the single most important exam sign of RV hypertrophy
6. Gross Pathology
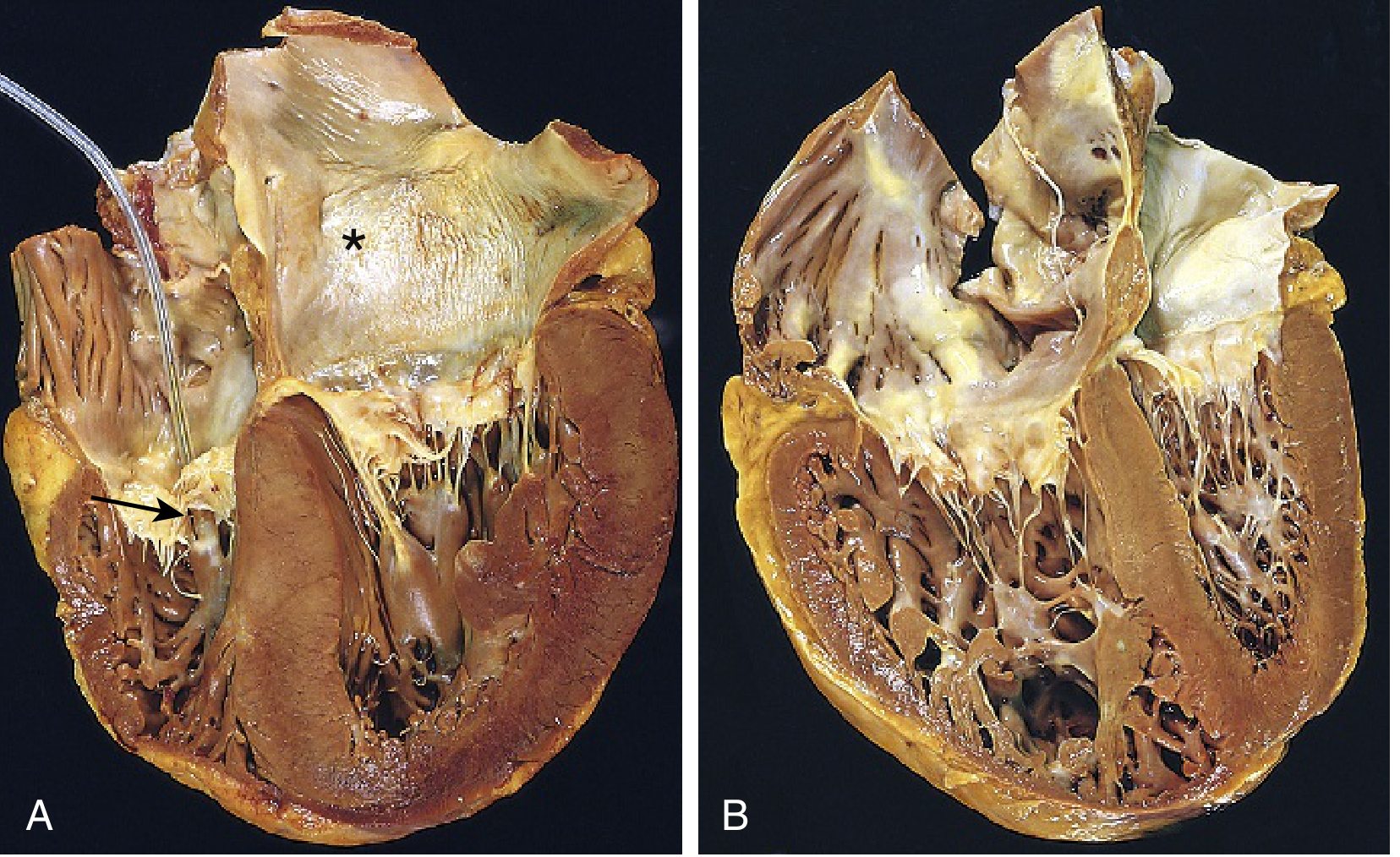
- Acute cor pulmonale (e.g., massive PE): RV dilation only — no time for hypertrophy
- Chronic cor pulmonale (e.g., COPD): RV hypertrophy + dilation; wall thickness may equal or exceed the LV
- Right atrium also hypertrophied and dilated
- Pulmonary arteries show intimal thickening
7. Investigations
| Investigation | Finding |
|---|---|
| ECG | P pulmonale (tall P in II), right axis deviation, RV strain (ST depression V1–V3), RBBB |
| CXR | Prominent pulmonary arteries, enlarged RA/RV, hyperinflated lungs (COPD) |
| Echocardiography | RV enlargement, RV hypertrophy, ↑ tricuspid regurgitant jet velocity (estimates PAP), reduced TAPSE (<16 mm = RV dysfunction), D-shaped LV (septal flattening) |
| Right Heart Catheterization | Gold standard — directly measures mean PAP (>25 mmHg), PVR, confirms diagnosis |
| ABG | ↓ PaO₂, ↑ PaCO₂, compensated respiratory acidosis |
| Spirometry | Obstructive pattern (↓ FEV₁/FVC) confirming COPD |
8. Management
Primary goal: Treat the underlying cause (COPD)
- Bronchodilators (LABA, LAMA) — reduce airflow obstruction
- Inhaled corticosteroids — reduce exacerbations
- Smoking cessation — most important modifier
Specific to Cor Pulmonale:
| Treatment | Indication/Mechanism |
|---|---|
| Supplemental oxygen (LTOT) | #1 treatment; PaO₂ < 55 mmHg or < 59 mmHg with edema/polycythemia/p pulmonale on ECG; reverses HPV |
| Diuretics | Volume overload, peripheral edema — loop diuretics |
| Anticoagulation | If CTEPH is contributing |
| Pulmonary vasodilators (e.g., sildenafil, bosentan) | Controversial in COPD-associated PH — risk of worsening V/Q mismatch |
| Calcium channel blockers | Only in responders to acute vasodilator challenge; not used routinely in COPD |
| Phlebotomy | If haematocrit > 55% causing symptomatic hyperviscosity |
| Lung transplantation | For end-stage disease |
Key FCPS point: Oxygen therapy is the ONLY intervention proven to improve survival in cor pulmonale from COPD. Vasodilators can worsen oxygenation by blunting HPV.
9. Prognosis
Once cor pulmonale is established:
- If mean PAP > 25 mmHg → 5-year survival reduced by 50%
- Development of overt RV failure is a very late and ominous sign
- Survival improves significantly with LTOT
10. FCPS High-Yield Summary Points
| Point | Fact |
|---|---|
| Most common cause | COPD |
| Key mechanism | Hypoxic pulmonary vasoconstriction → PAH → RV overload |
| Most important physical sign | Left parasternal heave (RV hypertrophy) |
| Gold standard for diagnosis | Right heart catheterization |
| Best screening tool | Echocardiography |
| Only survival-improving treatment | Long-term oxygen therapy (LTOT) |
| Edema mechanism in cor pulmonale | Not just pump failure — hypercapnia + renal Na retention |
| Vasodilators | Controversial — may worsen V/Q mismatch |
| Acute cor pulmonale vs chronic | Acute = dilation only (PE); Chronic = hypertrophy + dilation (COPD) |
— Fuster & Hurst's The Heart, 15th Ed. | Robbins & Kumar Basic Pathology | Fishman's Pulmonary Diseases & Disorders
This is a shared conversation. Sign in to Orris to start your own chat.