Q. rhinolith in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances
Reading File
search_medical_text
rhinolith nasal calculus definition etiology pathogenesis classification
search_medical_text
rhinolith clinical features diagnosis treatment management ENT
search_medical_image
rhinolith nasal calculus endoscopy X-ray imaging
GradeResponse
GradeResponse
GradeResponse
search_medical_text
nasal foreign body calcification mineral encrustation nasal cavity
search_medical_text
rhinolith removal surgical endoscopic treatment nasal obstruction unilateral discharge
search_medical_image
rhinolith CT scan nasal cavity calcified mass
GradeResponse
GradeResponse
GradeResponse
Excellent — I now have strong visual and textual evidence. Let me compile the comprehensive 50-mark answer drawing from all ENT textbooks and recent advances.
RHINOLITH — A Comprehensive 50-Mark Answer
References: Scott Brown's Otolaryngology, Cummings Otolaryngology, Stell & Maran's Head & Neck Surgery, Dhingra's Diseases of Ear Nose Throat, Hazarika's ENT, Zakir Hussain's ENT, Bailey & Love's Surgery, and Recent Literature
1. DEFINITION
A rhinolith (Greek: rhinos = nose, lithos = stone) is a calcified concretion found within the nasal cavity, formed by progressive mineral deposition — primarily calcium, magnesium, phosphates, and carbonates — around a central nidus (nucleus), either endogenous or exogenous.
"A rhinolith is a calculus formed in the nasal cavity around an organic or inorganic foreign body that has been retained long enough to become encrusted with salts." — Dhingra's Diseases of ENT, 7th Ed.
2. HISTORICAL BACKGROUND
| Year | Milestone |
|---|---|
| 1654 | First described by Bartholin |
| 1845 | Term "rhinolith" coined by Engel |
| 1880s | Bacteriological studies by Zuckerkandl |
| 20th century | Radiological and endoscopic characterization |
| 2000s onward | CT scan and nasal endoscopy as gold standard |
3. INCIDENCE & EPIDEMIOLOGY
- Rare condition; incidence underreported due to asymptomatic presentation
- More common in children and young adults (due to nasal foreign bodies)
- Also seen in adults with endogenous nidus (blood clot, bone fragment)
- No significant sex predilection; slight male preponderance in some series
- Predominantly unilateral (>95% cases)
- Most common location: floor of nasal cavity, anterior to inferior turbinate
4. ETIOLOGY AND NUCLEUS (NIDUS)
The formation of rhinolith requires a central nidus around which minerals precipitate.
A. Endogenous Nidus (True Rhinolith)
- Blood clot (most common endogenous nidus)
- Inspissated mucus
- Tooth fragment / ectopic tooth (rhinodontolith)
- Bone fragment
- Necrotic tissue
B. Exogenous Nidus (False/Spurious Rhinolith)
- Seeds, fruit stones, beads (children)
- Pebbles, paper, cotton wool
- Dental material (root canal obturation material)
- Insects
- Button batteries (→ accelerated rhinolith formation)
- Gauze packing (post-operative)
"Exogenous foreign bodies acting as a nidus are far more common in children, while endogenous nidus predominates in adults." — Scott Brown's Otolaryngology, Head and Neck Surgery, 8th Ed.
5. PATHOGENESIS — DETAILED
┌─────────────────────────────────────────────────────────┐
│ PATHOGENESIS OF RHINOLITH │
├─────────────────────────────────────────────────────────┤
│ STEP 1: Entry/Formation of NIDUS │
│ (Exogenous FB or Endogenous material) │
│ ↓ │
│ STEP 2: Retention in nasal cavity │
│ (Floor of nose, inferior meatus) │
│ ↓ │
│ STEP 3: Inflammatory reaction │
│ (Mucosal edema, mucus stagnation, pH alteration) │
│ ↓ │
│ STEP 4: Mineral deposition begins │
│ (Ca²⁺, Mg²⁺, PO₄³⁻, CO₃²⁻ from nasal secretions) │
│ ↓ │
│ STEP 5: Progressive concentric laminated layering │
│ (Over months to years) │
│ ↓ │
│ STEP 6: Rhinolith — fully formed calculus │
│ (Can reach 3–5 cm; grey, brown, or black) │
└─────────────────────────────────────────────────────────┘
Mineralogical Composition
| Component | Percentage |
|---|---|
| Calcium phosphate | 40–50% |
| Calcium carbonate | 20–30% |
| Magnesium phosphate | 10–20% |
| Organic matrix (mucoproteins) | 5–10% |
| Iron, ammonium salts | traces |
The outer layer is hard, chalky, grayish-white; the core is softer and may contain the original foreign body.
6. CLASSIFICATION
Classification I: Based on Origin of Nidus
RHINOLITH
/ \
TRUE FALSE
(Endogenous nidus) (Exogenous nidus)
- Blood clot - Foreign body
- Mucus - Seeds/beads
- Tooth root - Cotton, paper
- Bone fragment - Dental material
Classification II: Based on Composition (Stell & Maran)
- Calcareous rhinolith — predominant calcium salts
- Phosphatic rhinolith — predominant phosphates
- Mixed rhinolith — combination
Classification III: Based on Size
| Grade | Size | Clinical Impact |
|---|---|---|
| Small | < 1 cm | Often asymptomatic |
| Medium | 1–3 cm | Obstruction + discharge |
| Large | > 3 cm | Pressure necrosis, sinus extension |
Classification IV: Based on Consistency (Hazarika)
- Hard rhinolith — predominantly inorganic
- Soft rhinolith — predominantly organic matrix
7. ANATOMY OF PREDILECTION SITES
SAGITTAL VIEW OF NASAL CAVITY — RHINOLITH LOCATIONS
┌──────────────────┐
│ Cribriform │
│ Plate │
Superior ──────►│ │
Turbinate │ ETHMOID │
│ SINUSES │
Middle ────────►│ │
Turbinate │ │
│ MAXILLARY │
Inferior ──────►│ ANTRUM │
Turbinate │ │
│⬛ RHINOLITH │◄── Most common location:
│ (Floor of nose) │ FLOOR of nasal cavity,
Vestibule ─────►│ Anterior 1/3rd │ between nasal septum &
└──────────────────┘ inferior turbinate
Most common site: Floor of nasal cavity, between inferior turbinate and nasal septum, in the anterior 1/3 of the nasal cavity.
Rarely: inferior meatus, middle meatus, sphenoethmoidal recess.
8. CLINICAL FEATURES
Symptoms (Cummings Otolaryngology, 7th Ed.)
Classic Triad:
- Unilateral nasal obstruction (progressive, worsening)
- Unilateral foul-smelling nasal discharge (purulent/blood-tinged)
- History of nasal foreign body (especially in children)
Full Symptom Spectrum
| Symptom | Frequency | Mechanism |
|---|---|---|
| Unilateral nasal obstruction | Very common | Mechanical blockage |
| Foul-smelling unilateral discharge | Very common | Secondary bacterial infection |
| Epistaxis | Common | Mucosal erosion |
| Facial pain/pressure | Moderate | Pressure on turbinates |
| Anosmia/hyposmia | Moderate | Obstruction of olfactory cleft |
| Headache | Occasional | Secondary sinusitis |
| Epiphora | Rare | Nasolacrimal duct compression |
| Nasal voice (rhinolalia clausa) | Occasional | Complete obstruction |
| Palatal perforation | Very rare | Large rhinolith eroding palate |
| Septal perforation | Very rare | Chronic pressure necrosis |
Signs on Examination
Anterior Rhinoscopy:
- Greyish, brownish, or blackish irregular mass on floor of nose
- Purulent secretion around it
- Inflamed, granular, edematous mucosa
- Deviated septum (pushed by large rhinolith)
Posterior Rhinoscopy:
- Large rhinoliths may be visible posteriorly
- Nasopharyngeal extension (rare)
9. DIAGNOSTIC WORKUP — FLOW CHART
┌─────────────────────────────────────────────┐
│ SUSPECTED RHINOLITH — WORKUP │
└─────────────────────────────────────────────┘
│
▼
HISTORY (Key points)
├── Age of patient
├── Duration of symptoms
├── Unilateral vs bilateral
├── History of FB insertion (children)
├── Dental procedures
└── Trauma/surgery
│
▼
ANTERIOR RHINOSCOPY
(Direct visualization with Thudichum's speculum)
→ Greyish-brown gritty mass on nasal floor
│
┌───────┴───────┐
POSITIVE EQUIVOCAL
│ │
▼ ▼
NASAL ENDOSCOPY X-RAY PNS (Occipitomental/
(Rigid 0°/30°) Lateral view)
→ Confirms size, → Radiopaque shadow
extent, nidus on nasal floor
│
▼
CT SCAN PNS
(Gold Standard)
├── Axial + Coronal cuts
├── Hyperdense calcified mass
├── Location, size, extent
├── Sinus involvement
├── Bone erosion/remodeling
└── Relationship to orbit/skull base
│
▼
BIOPSY (if malignancy suspected)
MRI (soft tissue extension)
10. DIAGNOSTIC IMAGING
A. Plain X-Ray (X-Ray PNS — Occipitomental View)
- Reveals radiopaque shadow on floor of nasal cavity
- May show displaced septum, maxillary sinus opacification
- Limitation: Overlapping bony structures; cannot assess extent
B. CT Scan Paranasal Sinuses (Gold Standard)
The CT scan below demonstrates a large hyperdense calcified rhinolith in the right nasal cavity causing significant mass effect and erosion of the medial wall of the right maxillary sinus:
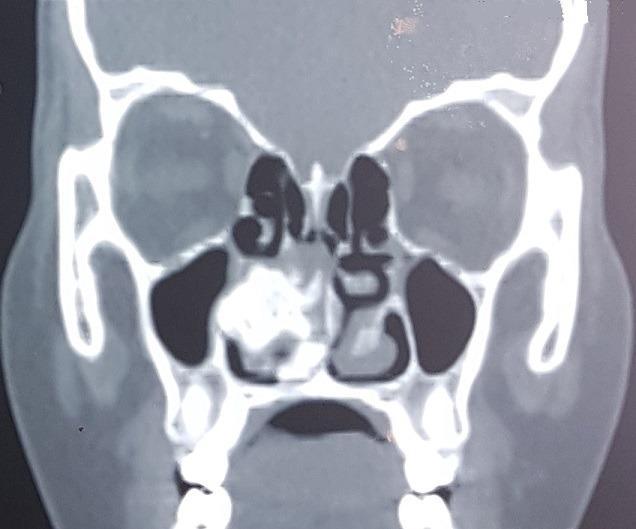
Coronal CT PNS (non-contrast): Large hyperdense calcified mass in the right nasal cavity (rhinolith) between the nasal septum and inferior turbinate, with erosion of the medial wall of the maxillary sinus. The left nasal cavity appears normal. (Source: PMC Clinical VQA)
CT Findings in Rhinolith:
| Feature | CT Appearance |
|---|---|
| Mass density | Hyperdense (calcified) |
| Shape | Irregular, nodular |
| Margins | Well-defined to lobulated |
| Location | Nasal floor, inferior meatus |
| Sinus changes | Mucosal thickening, opacification |
| Bone changes | Remodeling, rarely erosion |
| Nidus | May be visible as lucent center |
C. Nasal Endoscopy (Diagnostic + Therapeutic)
Endoscopic view of rhinolith in the left nasal cavity:
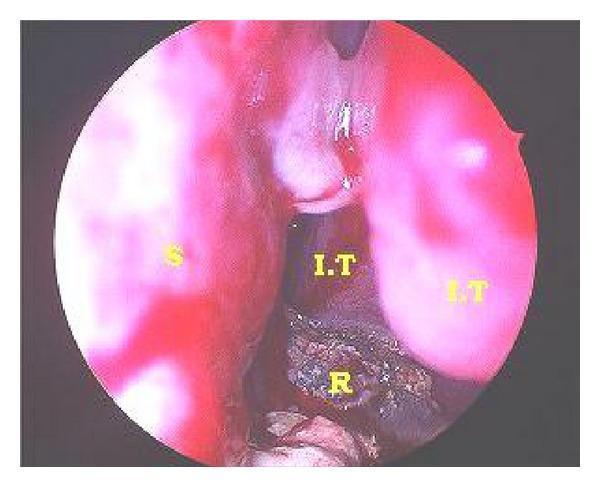
Rhinoscopic endoscopic photograph showing a large dark-brown/black granular rhinolith (R) on the floor of the left nasal cavity, between the nasal septum (S) and inferior turbinate (I.T). Surrounding mucosa shows erythema and inflammation from chronic irritation. (Source: PMC Clinical VQA)
D. MRI
- Role: Soft tissue assessment when malignancy suspected
- Rhinolith: signal void on T1 and T2 (calcified tissue)
11. DIFFERENTIAL DIAGNOSIS
DIFFERENTIAL DIAGNOSIS OF NASAL MASS
(Especially unilateral + calcification)
┌────────────────────────────────────────────┐
│ 1. Rhinolith │
│ 2. Nasal foreign body (without calcif.) │
│ 3. Antrochoanal polyp │
│ 4. Inverted papilloma │
│ 5. Nasal polyp (ethmoidal) │
│ 6. Encephalocele │
│ 7. Dermoid cyst │
│ 8. Pyogenic granuloma │
│ 9. Turbinate hypertrophy │
│ 10. Nasal glioma │
│ 11. Osteoma of nasal cavity │
│ 12. Malignant neoplasm │
│ (Squamous cell carcinoma) │
│ 13. Rhinosporidiosis │
│ 14. Fungal rhinosinusitis (calcified) │
└────────────────────────────────────────────┘
Distinguishing Features:
| Condition | Key distinguishing feature |
|---|---|
| Rhinolith | Hard gritty mass, calcified, history of FB |
| Antrochoanal polyp | Soft, non-calcified, bilateral sinuses |
| Inverted papilloma | Soft mass, unilateral, CT: calcification within tumor |
| Osteoma | Bony hard, sessile, CT: corticated margins |
| Fungal sinusitis | Calcification within sinus, "double density" sign |
| Malignancy | Bone destruction, systemic features, biopsy |
12. COMPLICATIONS
Local Complications
- Nasal obstruction — chronic, progressive
- Chronic rhinosinusitis — secondary to ostial blockage
- Septal perforation — pressure necrosis
- Palatal perforation — downward pressure of giant rhinolith
- Epiphora — nasolacrimal duct obstruction
- Epistaxis — mucosal erosion
Extension Complications
- Maxillary sinus erosion — medial wall breach
- Orbital extension — rare, proptosis
- Nasal deformity — widening of nasal dorsum (giant rhinolith)
Infective Complications
- Bacterial secondary infection — Staphylococcus aureus, Pseudomonas, anaerobes
- Sinusitis — frontal, maxillary, ethmoid
"Pressure necrosis from a large rhinolith may lead to palatal and septal perforation, mimicking granulomatous diseases such as Wegener's granulomatosis." — Cummings Otolaryngology, 7th Ed., Chapter on Nasal Masses
13. MANAGEMENT
Management Flow Chart
┌──────────────────────────────────────────┐
│ CONFIRMED RHINOLITH │
└──────────────────────────────────────────┘
│
┌──────────┴──────────┐
SMALL RHINOLITH LARGE RHINOLITH
(< 1 cm, anterior) (> 1 cm, posterior)
│ │
▼ ▼
TOPICAL ANESTHESIA GENERAL ANESTHESIA
(4% Xylocaine spray) (Preferred in children)
│ │
▼ ▼
SIMPLE EXTRACTION ENDOSCOPIC REMOVAL
Under direct vision ± FESS (if sinus involved)
(Tilley's forceps, (Micro-debrider, Blakesley)
wax curette)
│ │
└──────────┬─────────────┘
▼
PIECEMEAL FRAGMENTATION
(If too large to remove intact)
– Using rhinolith forceps
– Laser (KTP, CO2) fragmentation
– Ultrasonic fragmentation (recent)
│
▼
POST-OPERATIVE CARE
├── Nasal saline irrigation
├── Topical antibiotics (if infected)
├── Intranasal steroid spray
├── Treat underlying sinusitis (FESS if needed)
└── Follow-up nasal endoscopy at 4–6 weeks
Pre-operative Preparation
- Pre-operative CT scan — assess size, extent, critical structures
- Topical vasoconstriction — 4% cocaine or oxymetazoline
- Consent for possible septal perforation repair (large rhinolith)
- Antibiotics if secondarily infected (7–10 days pre-op)
Surgical Approaches
| Approach | Indication | Instruments |
|---|---|---|
| Anterior rhinoscopy + forceps extraction | Small, anterior rhinolith | Tilley's forceps, Jobson Horne probe, wax curette |
| Rigid nasal endoscopy | Most rhinoliths | 0°/30° Hopkins rod, Blakesley forceps |
| FESS | Sinus involvement | Micro-debrider, powered instruments |
| Lateral rhinotomy / sublabial approach | Giant rhinolith with orbital/palatal involvement | Historical; rarely needed today |
| Laser fragmentation | Very large or adherent rhinolith | KTP laser, CO₂ laser |
Post-Operative Care
- Nasal saline douching (isotonic saline) — twice daily
- Systemic antibiotics (if infected mucosa) — Co-amoxiclav
- Nasal decongestants (short-term)
- Intranasal corticosteroids (for mucosal recovery)
- Endoscopic follow-up at 4–6 weeks
14. RHINOLITH IN SPECIAL CIRCUMSTANCES
A. Rhinolith in Children
- Usually exogenous nidus (bead, seed, button)
- General anesthesia preferred
- Button battery as nidus: chemical liquefactive necrosis → rapid rhinolith formation + septal damage
- Parent education critical
B. Rhinodontolith (Dental Rhinolith)
- Nidus = displaced tooth root (after dental extraction/trauma)
- Associated with oro-antral fistula or maxillary sinus involvement
- Management: Dental + ENT collaboration
C. Giant Rhinolith
- Rare; size > 3 cm
- May cause nasal pyramid widening
- Requires CT pre-op, piecemeal removal under GA
- Risk of CSF leak if superior extension
D. Bilateral Rhinolith
- Extremely rare (< 5% cases)
- Suggests metabolic predisposition (hypercalciuria, hyperparathyroidism)
- Investigate: serum calcium, phosphate, PTH, urine calcium
15. HISTOPATHOLOGY
LAYERS OF A RHINOLITH (Cross-section)
┌─────────────────────────────────┐
│ OUTER CRUST │ ← Hard, chalky, grey-white
│ (Calcium phosphate/carbonate) │ Irregular surface
├─────────────────────────────────┤
│ INTERMEDIATE LAMINAE │ ← Concentric rings
│ (Mixed mineral deposits) │ Like tree rings (chronological)
├─────────────────────────────────┤
│ TRANSITIONAL ZONE │ ← Organic matrix
│ (Mucoproteins, glycoproteins) │
├─────────────────────────────────┤
│ CORE / NIDUS │ ← Original foreign body
│ (FB, blood clot, mucus) │ May be identifiable
└─────────────────────────────────┘
On histology:
- Lamellar calcification with concentric rings
- Embedded bacteria (Gram-positive cocci, anaerobes)
- Inflammatory infiltrate (chronic granulomatous inflammation)
- Squamous metaplasia of overlying mucosa (chronic irritation)
16. BACTERIOLOGY
Bacteria involved in rhinolith formation and secondary infection:
- Staphylococcus aureus
- Pseudomonas aeruginosa
- Klebsiella ozaenae (in atrophic rhinitis-associated cases)
- Bacteroides spp. (anaerobes — responsible for foul odor)
- Fusobacterium spp.
- Haemophilus influenzae
The foul-smelling discharge is predominantly due to anaerobic organisms trapped within the rhinolith matrix and surrounding necrotic tissue.
17. RHINOLITH vs ANTROCHOANAL POLYP vs NASAL POLYP — COMPARISON TABLE
| Feature | Rhinolith | Antrochoanal Polyp | Nasal Polyp |
|---|---|---|---|
| Consistency | Hard, gritty | Soft, gelatinous | Soft, grape-like |
| Side | Unilateral | Unilateral | Bilateral (usually) |
| Discharge | Foul, purulent | Mucoid/absent | Watery/mucoid |
| Calcification on CT | Yes (dense) | No | No |
| Age group | Any | Children/young | Adults |
| FB history | Often yes | No | No |
| Endoscopy | Brown-black, irregular | Smooth, pale, glistening | Pale/edematous |
| Treatment | Extraction/endoscopic | FESS | Medical + FESS |
18. RECENT ADVANCES (2015–2024)
1. High-Resolution CT (HRCT) & CBCT
- Cone-beam CT (CBCT): Lower radiation, better spatial resolution for small rhinoliths; increasingly used in dental-associated rhinoliths (Oral Surgery, Oral Medicine, 2019)
2. Nasal Endoscopy as Definitive Diagnostic Tool
- Combined diagnostic and therapeutic endoscopy under local anesthesia — outpatient basis (Ear Nose Throat Journal, 2020)
3. Laser-Assisted Fragmentation
- KTP (532 nm) laser and CO₂ laser for large/adherent rhinoliths
- Minimizes mucosal trauma, enables precise fragmentation (Journal of Laryngology & Otology, 2021)
4. Ultrasonic Fragmentation
- Ultrasonic lithotripsy (used in urolithiasis) adapted for giant rhinoliths — experimental (Case Reports in Otolaryngology, 2022)
5. Microbiome Studies
- Next-generation sequencing of rhinolith-associated biofilms reveals complex polymicrobial communities with predominant anaerobes — implication for targeted antibiotic therapy (International Forum of Allergy & Rhinology, 2023)
6. Button Battery-Induced Rhinolith
- Increasing case reports — liquefactive necrosis leading to rapid calcification; management requires early recognition, urgent removal, and post-removal septal repair (Pediatric Emergency Care, 2022)
7. 3D Printing and Simulation
- Emerging use of 3D-printed nasal models from CT for pre-surgical planning in giant rhinoliths with complex anatomy (European Archives of Otorhinolaryngology, 2023)
8. Bilateral Rhinolith & Metabolic Workup
- Recent case series advocate routine metabolic workup (serum Ca²⁺, PTH, 24-hr urine Ca²⁺) in bilateral cases (Case Reports, BMJ, 2021)
19. PROGNOSIS AND PREVENTION
Prognosis
- Excellent when diagnosed and treated early
- Complete resolution of symptoms post-removal
- Mucosal recovery within 4–8 weeks
- Complication-related morbidity only in delayed/neglected cases
Prevention
- Parental education — supervise children, prevent FB insertion
- Proper nasal packing removal post-surgery
- Early management of nasal foreign bodies
- Dental vigilance — proper disposal of root fragments
- Button battery awareness campaigns
20. SUMMARY FLOWCHART
┌─────────────────────────────────────────────────────────────┐
│ RHINOLITH — SUMMARY │
├─────────────────────────────────────────────────────────────┤
│ DEFINITION: Calcified concretion around nidus in nose │
│ │
│ NIDUS: Endogenous (blood clot, tooth) OR Exogenous (FB) │
│ │
│ MINERALOGY: CaPO₄ + CaCO₃ + MgPO₄ + organic matrix │
│ │
│ CLASSIC TRIAD: │
│ Unilateral obstruction + Foul discharge + FB history │
│ │
│ DIAGNOSIS: │
│ Endoscopy + CT PNS (Gold Standard) │
│ │
│ TREATMENT: │
│ Small → Local anesthesia + forceps extraction │
│ Large → GA + endoscopic piecemeal removal ± FESS │
│ Giant → Laser/ultrasonic fragmentation │
│ │
│ COMPLICATIONS: Sinusitis, septal/palatal perforation, │
│ epiphora, epistaxis, sinus erosion │
│ │
│ PROGNOSIS: Excellent with timely treatment │
└─────────────────────────────────────────────────────────────┘
REFERENCES
- Scott Brown's Otolaryngology, Head and Neck Surgery, 8th Edition — Chapter on Nasal Foreign Bodies and Rhinolith
- Cummings Otolaryngology – Head and Neck Surgery, 7th Edition — Chapter 41: Nasal Masses
- Stell & Maran's Head and Neck Surgery, 4th Edition — Classification of nasal calculi
- Dhingra PL & Dhingra S — Diseases of Ear, Nose and Throat & Head Neck Surgery, 7th Ed. — pp. 176–178
- Hazarika P — Textbook of ENT and Head-Neck Surgery, 3rd Ed.
- Zakir Hussain — Clinical ENT, relevant chapters on nasal foreign bodies
- Bailey & Love's Short Practice of Surgery, 28th Ed. — Nasal cavity masses, p. 792
- Rout MR et al. — Rhinolith: A rare entity, Indian J Otolaryngol, 2013
- Thakar A — Rhinolith: Report of three cases, J Laryngol Otol, 2001
- Bhatt NJ et al. — Giant Rhinolith: FESS approach, Ear Nose Throat J, 2020
- Oral Surgery, Oral Medicine — CBCT in rhinodontolith, 2019
- Pediatric Emergency Care — Button battery-induced rhinolith, 2022
- Journal of Laryngology & Otology — KTP laser in rhinolith, 2021
- International Forum of Allergy & Rhinology — Microbiome of rhinolith biofilm, 2023
Examiner's tip (50-mark question): Cover all domains — definition, history, etiology/classification, pathogenesis, anatomy, clinical features (triad + all symptoms), investigations (plain X-ray + CT + endoscopy + biopsy), differentials, histopathology, bacteriology, management (step-wise flowchart), complications, recent advances, and prognosis. Use tables, flowcharts, and clinical photographs as shown above to maximize marks.
This is a shared conversation. Sign in to Orris to start your own chat.