How to reverse hypoxic brain injury..and its recovery time
Reading File
Searching PubMed
hypoxic brain injury recovery treatment
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough, textbook-grounded answer.
Hypoxic Brain Injury: Reversal & Recovery
What Is It?
Hypoxic (or hypoxic-ischemic) brain injury results from oxygen deprivation to the brain, most commonly from cardiac arrest, respiratory failure, near-drowning, asphyxiation, severe hypotension, or CO/cyanide poisoning. The brain depletes its oxygen reserve within seconds and energy stores (ATP) within 4-5 minutes, after which irreversible neuronal death begins in the most vulnerable areas: the CA1 hippocampus, globus pallidus, and neocortex.
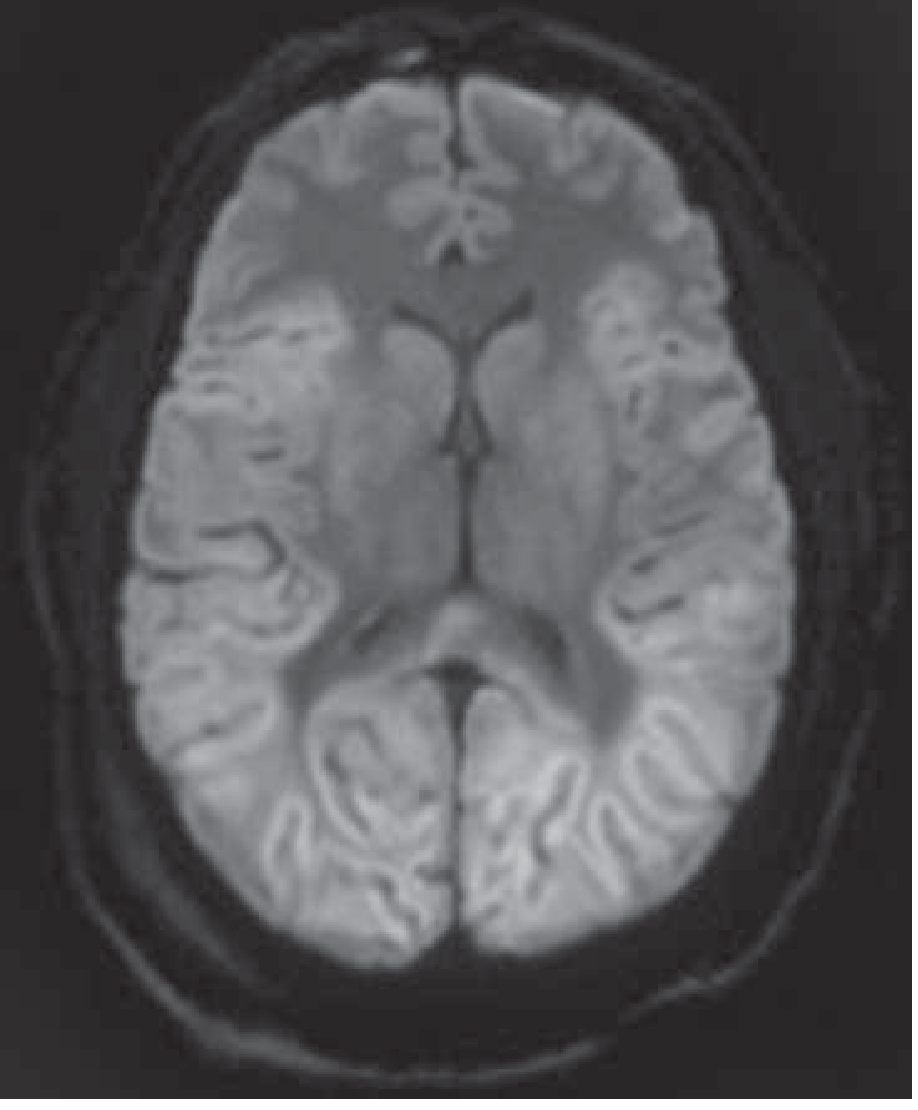
Below is a DWI-MRI showing diffuse hypoxic-ischemic injury after cardiac arrest - the bright signal throughout the cerebral cortex reflects reduced diffusion from cytotoxic edema:
Can It Be "Reversed"?
Partial or full reversal is possible only when oxygen is restored quickly and the insult is not too severe. The key window:
| Duration of Hypoxia-Ischemia | Expected Outcome |
|---|---|
| Restored within 3-5 minutes | Full recovery possible |
| 5-10 minutes | Variable; some achieve near-full recovery |
| Beyond 10+ minutes | Likely permanent damage; rare exceptions exist |
| Pure hypoxia (no ischemia) | Brain more tolerant - a PaO2 as low as 20 mmHg can be survived if gradual and BP maintained |
The brain is significantly less tolerant to combined hypoxia+ischemia than to pure hypoxia alone. - Harrison's Principles of Internal Medicine, 22E
Acute Treatment (Reversal Strategies)
1. Restore Oxygenation and Circulation - First Priority
- Secure airway, begin CPR immediately - "every second counts"
- Restore cardiopulmonary function with supplemental oxygen, IV fluids, vasopressors (norepinephrine is commonly used)
- Target SpO2 94-98% - hyperoxia (>98%) is harmful and worsens functional outcomes
- Maintain systolic BP >90 mmHg (MAP >60 mmHg)
- Normoglycemia (glucose target 140-180 mg/dL) - both hypo- and hyperglycemia worsen outcome
2. Targeted Temperature Management (TTM) - Core Neuroprotective Strategy
- Goal: Reduce cerebral metabolic demand and interrupt the neuronal injury cascade (glutamate toxicity, free radicals, calcium influx)
- Target temperature: 32-37.5°C; most centers use 33°C or 36°C - current guidelines show similar outcomes between the two
- Duration: 24 hours of temperature control
- Methods: Surface cooling (ice packs, cooling pads/blankets), IV chilled saline infusion, or endovascular cooling devices with real-time temperature feedback
- Critical rule: Fever must be prevented in ALL cases - even low-grade fever worsens outcome
- Complications to watch: coagulopathy, infection risk, electrolyte shifts (especially K+, Mg2+, PO4), bradycardia
High-dose barbiturates have NOT shown the same neuroprotective benefit as hypothermia - Adams & Victor's Principles of Neurology, 12E
3. Treat Seizures
- Myoclonic status epilepticus and burst-suppression EEG patterns are common after severe injury and indicate poor prognosis
- Treat with standard anticonvulsants; continuous EEG monitoring is recommended
4. Treat the Underlying Cause
- ST-elevation MI post-arrest: emergent cardiac catheterization
- Head CT to rule out hemorrhagic stroke or SAH (note: diffuse hypoxic injury can mimic SAH on CT - "pseudo-SAH" appearance)
- MRI with DWI is the most sensitive imaging to assess extent of injury
5. Emerging/Investigational Therapies
- Repetitive TMS (rTMS) targeting the dorsolateral prefrontal cortex shows promise for recovery of consciousness in disorders of consciousness - a 2025 meta-analysis (PMID 41094293) found benefit from rTMS in patients with prolonged consciousness disorders
- GLP-1 receptor agonists are being studied post-ischemic stroke as neuroprotective agents (2026 systematic review, PMID 41263069)
- Erythropoietin, hypothermia optimization, and stem cell approaches are under investigation but not established
Recovery Timeline
Recovery is highly variable and depends on the severity of injury, duration of hypoxia, age of the patient, and rapidity of treatment.
General Timeline
| Timeframe | What May Happen |
|---|---|
| Hours-Days | Stabilization; patient in coma; brainstem reflexes reassessed |
| 3-7 days | Most meaningful prognostic assessment (after sedation is cleared) |
| 1-4 weeks | Transition from coma to vegetative/minimally conscious state or early awakening |
| 3-6 months | Major neurological recovery phase; most functional gains occur here |
| 6-12 months | Continued but slower improvement; ~13% of post-cardiac arrest survivors reach independent function |
| Beyond 1 year | Recovery is possible but slower; some patients in minimally conscious states can still improve |
Long-Term Outcomes (Post-Cardiac Arrest Data)
Based on Adams & Victor's and Harrison's 22E:
- ~13% of patients post-cardiac arrest achieve independent function within 1 year
- Patients with intact brainstem reflexes on admission (reactive pupils, eye movements, any motor response) had favorable outcomes in ~50% of cases
- None of the patients with absent pupillary light reflexes on admission regained independent function
- Some patients treated with hypothermia may awaken after a week or longer - prognostic assessment should not be rushed
Long-Term Consequences
- Persistent coma or unresponsive wakefulness (vegetative state)
- Dementia and memory impairment
- Visual agnosia
- Parkinsonism (basal ganglia involvement)
- Delayed post-anoxic leukoencephalopathy (rare - worsening days to weeks after apparent initial recovery)
- Depression (prevalence >25% after recovery from hypoxic events)
Prognostic Markers (Poor Outcome)
The following at 5-7 days post-injury (or earlier if no hypothermia used) strongly predict poor outcome:
- Absent pupillary light reflex
- Absent corneal reflexes
- No withdrawal or absent motor response to pain
- Bilateral absence of N20 SSEP waves
- EEG showing burst-suppression or myoclonic status epilepticus
- Serum NSE >60 µg/L in the first 1-3 days
Important caveat: In patients treated with hypothermia, these signs can be falsely pessimistic. The false-positive rate for predicting poor outcome based on 3-day motor function can be as high as 21%. Always use a multimodal approach (clinical + EEG + imaging + biomarkers) and allow sufficient observation time. - Harrison's 22E
Rehabilitation (Recovery Support)
- Neuroplasticity allows partial rewiring of function, especially in younger patients
- Multidisciplinary rehab: physiotherapy, occupational therapy, speech-language therapy, cognitive rehabilitation
- Spasticity management, nutritional support, prevention of secondary complications (DVT, pneumonia, pressure ulcers)
- Family presence in the ICU can help with orientation and reducing agitation
- Sensory stimulation programs for patients in low-consciousness states
Bottom line: The most effective "reversal" of hypoxic brain injury is rapid restoration of circulation and oxygenation, combined with fever prevention and targeted temperature management. There is no pharmacological agent proven to fully reverse established hypoxic brain damage. Meaningful neurological recovery can occur over 6-12+ months, but the extent depends heavily on how long the brain was deprived of oxygen.
Sources: Harrison's Principles of Internal Medicine 22E (2025), Adams & Victor's Principles of Neurology 12E, Plum & Posner's Diagnosis and Treatment of Stupor and Coma, Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.