Management of HRS
Reading File
Finding Sources
Searching PubMed
"hepatorenal syndrome" AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative content from multiple major textbooks. Let me compile the full response.
Management of Hepatorenal Syndrome (HRS)
Pathophysiology (Brief Overview)
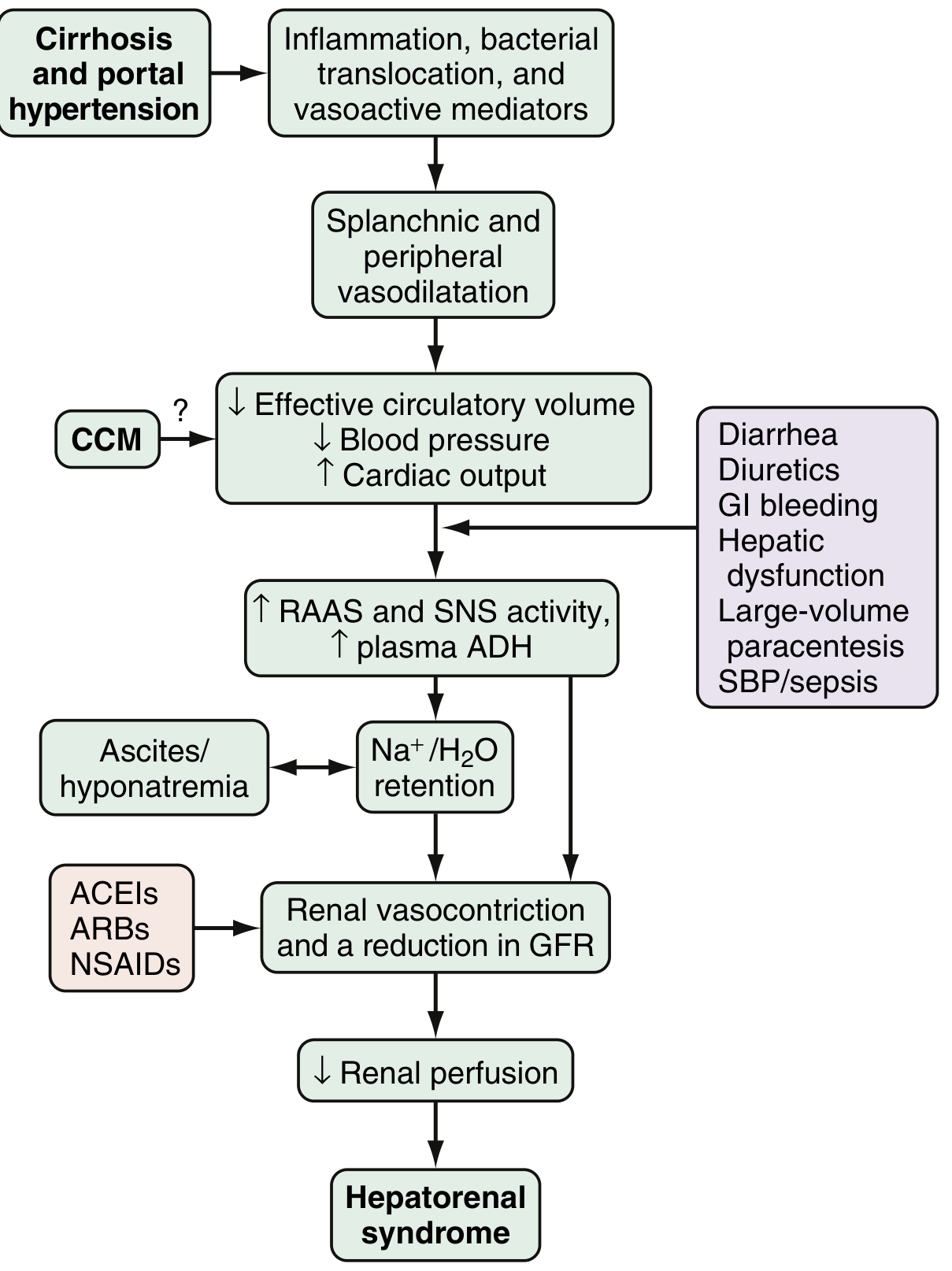
HRS is a functional form of renal failure without intrinsic renal pathology, arising from the hemodynamic consequences of advanced cirrhosis and portal hypertension. The key mechanism is splanchnic and peripheral arterial vasodilation (mediated by NO, CO, glucagon, prostacyclin, and other vasoactive mediators), which reduces effective circulating volume, activates the RAAS, sympathetic nervous system, and ADH release, culminating in intense renal vasoconstriction and reduced GFR.
Classification
| Type | New Terminology | Course | Prognosis |
|---|---|---|---|
| Type 1 HRS | HRS-AKI | Rapid, progressive | Median survival ~2 weeks without treatment |
| Type 2 HRS | HRS-CKD | Gradual, stable | Median survival ~4-6 months; risk of progressing to type 1 |
Type 1 HRS (HRS-AKI) is defined as stage 2 or 3 AKI (creatinine rise >2-fold above baseline, or >3-fold, or >4 mg/dL with acute increase ≥0.3 mg/dL). Type 2 is considered a form of CKD. - Sleisenger & Fordtran's, p. 1819
Diagnostic Criteria (ICA 2019)
All of the following must be present:
- Cirrhosis, acute liver failure, or acute-on-chronic liver failure (ACLF) with ascites
- AKI: serum creatinine rise ≥0.3 mg/dL within 48 h, OR ≥50% from baseline within 7 days; or urine output ≤0.5 mL/kg/h for ≥6 h
- No full or partial response after at least 2 days of diuretic withdrawal + albumin (1 g/kg/day, max 100 g/day)
- Absence of shock
- No current or recent nephrotoxic drugs (NSAIDs, aminoglycosides, contrast)
- No parenchymal kidney disease (proteinuria >500 mg/day, microhematuria >50 RBC/hpf, abnormal renal US)
- FENa <0.2% (highly predictive if <0.1%)
- Comprehensive Clinical Nephrology, 7th Ed., Box 76.2
Prevention
Prevention is the most important strategy given the high mortality once HRS is established.
Avoid precipitants:
- Over-diuresis (stepwise approach: spironolactone 100 mg/day → max 400 mg/day; furosemide added → max 160 mg/day)
- Large-volume paracentesis without albumin replacement (give albumin 8 g per liter of ascites removed)
- NSAIDs, ACEIs, ARBs, aminoglycosides, IV contrast
- GI bleeding (use beta-blockers, band ligation for varices)
- Cautious use of beta-blockers in refractory ascites (reduce MAP and GFR)
Specific prophylactic measures:
-
SBP: Give IV albumin 1.5 g/kg on day 1 + 1.0 g/kg on day 3 to prevent HRS in patients with SBP - reduces risk of renal failure and improves survival
-
Severe alcoholic hepatitis: Pentoxifylline has been used
-
High-risk patients with low ascites protein (<1 g/L) + advanced liver dysfunction: long-term antibiotic prophylaxis (ciprofloxacin 500 mg/day or rifaximin 600 mg BID)
-
Harrison's 22E; Sleisenger & Fordtran's; Comprehensive Clinical Nephrology 7th Ed.
Treatment
Step 1: Immediate Measures (all patients)
- Stop all diuretics, NSAIDs, ACEIs, ARBs, lactulose (if contributing to volume depletion)
- Treat underlying precipitants (infection, GI bleed)
- Volume expansion: IV albumin 1 g/kg/day (max 100 g/day) for 48 h - if no improvement, HRS is confirmed
Step 2: Pharmacological (Vasoconstrictors + Albumin)
The rationale is to reverse splanchnic vasodilation and restore effective arterial blood volume. Vasodilators are contraindicated in HRS (ineffective and cause hypotension).
First-Line: Terlipressin + Albumin (preferred globally; FDA-approved in USA 2022)
| Parameter | Detail |
|---|---|
| Mechanism | V1-receptor vasopressin analog; preferential splanchnic vasoconstriction |
| Dose (bolus) | 0.5-1 mg IV every 4-6 h; increase to maximum 2 mg every 4 h if creatinine does not improve by 25% at day 3 |
| Dose (infusion) | 2 mg/24 h continuous IV, titrating up to max 12 mg/24 h (better tolerability, lower ischemic SE) |
| Albumin | 1 g/kg on day 1 (max 100 g), then 20-40 g/day |
| Duration | Until creatinine returns to within 0.3 mg/dL of baseline, or max 14 days |
| Efficacy | ~60% HRS reversal; 37% survival at 1 month |
| Key adverse effects | Respiratory failure (watch for pulmonary edema), systemic ischemia (peripheral, cardiac, mesenteric) |
| Contraindications | Ischemic heart disease, peripheral arterial disease, active respiratory failure |
- Comprehensive Clinical Nephrology 7th Ed., Box 76.3; Goldman-Cecil Medicine
Second-Line: Norepinephrine + Albumin (ICU setting)
| Parameter | Detail |
|---|---|
| Mechanism | Alpha-adrenergic agonist; systemic vasoconstriction |
| Dose | 0.1-0.7 mcg/kg/min IV; increase by 0.05 mcg/kg/min every 4 h; target MAP increase ≥10 mmHg |
| Albumin | Same as above |
| Duration | Max 14 days |
| Note | Requires ICU monitoring; comparable efficacy to terlipressin in several RCTs |
Third-Line (especially when terlipressin unavailable): Midodrine + Octreotide + Albumin
| Parameter | Detail |
|---|---|
| Midodrine | Start 2.5-5 mg PO TID → max 15 mg TID (alpha-1 agonist) |
| Octreotide | 100 mcg SC TID → max 200 mcg SC TID (or 25 mcg IV bolus + 25 mcg/h infusion) |
| Target | MAP increase ≥15 mmHg |
| Duration | Max 14 days |
| Note | Now considered third-line per Harrison's 22E 2025; widely used in the USA historically |
Per Harrison's 22E (2025): Midodrine + octreotide + albumin are now third line behind terlipressin (first) and norepinephrine (second).
Alternative: Vasopressin + Albumin (less commonly used)
- IV infusion starting at 0.01 U/min, titrating up to 0.8 U/min to achieve MAP increase ≥10 mmHg; max 11 days
Step 3: Renal Replacement Therapy (RRT)
- Indicated if pharmacotherapy fails and the patient develops uremia, severe hyperkalemia, acidosis, or fluid overload
- Not definitive - used as bridge to transplantation
- Patients requiring hemodialysis carry a 1.77x higher post-transplant mortality vs. those who do not need dialysis
Step 4: Transjugular Intrahepatic Portosystemic Shunt (TIPS)
- Best evidence for Type 2 HRS (HRS-CKD) / diuretic-resistant ascites
- Benefits: reduces portal pressure, improves serum creatinine, increases sodium excretion, improves neurohumoral responses
- Pilot studies in Type 1 HRS show some benefit, especially when combined with midodrine + octreotide + albumin followed by TIPS
- Limitations: Risk of worsening hepatic function (worsening hepatic encephalopathy) in decompensated cirrhosis; not suitable for high MELD score patients
Step 5: Liver Transplantation (Definitive Treatment)
- The only treatment with potential to reverse both liver dysfunction and HRS
- Any patient with HRS should be immediately evaluated for transplant and prioritized on the waiting list
- Outcomes:
- HRS reverses in 83% after liver transplantation (systematic review of 20 studies)
- 3-year survival ~60% (vs. 70-80% for non-HRS transplant patients)
- Up to 35% of HRS patients require long-term RRT post-transplant
- Pre-transplant dialysis is an independent predictor of worse survival (RR 1.77)
- Simultaneous liver-kidney transplantation (SLK) may be considered in appropriate candidates with prolonged renal failure
- Medical therapy (vasoconstrictors) serves as a bridge to transplantation
Step 6: Experimental / Salvage Options
- Extracorporeal albumin dialysis (MARS - Molecular Adsorbent Recirculating System): Experimental; mixed results in small trials; may reduce creatinine and improve survival in some patients; not effective as salvage after vasoconstrictor failure in HRS-AKI
- ET receptor antagonists (e.g., tezosentan): Studied but found to worsen renal function in HRS; not used clinically
Summary Algorithm
HRS suspected (AKI in cirrhosis with ascites)
↓
Stop diuretics, NSAIDs, ACEIs/ARBs
Albumin challenge: 1 g/kg/day × 2 days
Treat infections, GI bleeding
↓
No response → Confirm HRS-AKI diagnosis
↓
Vasoconstrictor + Albumin:
1st: Terlipressin (0.5-2 mg IV q4-6h) + Albumin
2nd: Norepinephrine (ICU) + Albumin
3rd: Midodrine + Octreotide + Albumin
↓
Evaluate for LIVER TRANSPLANTATION (all patients)
↓
If failing / uremia → RRT as bridge
TIPS: consider for HRS-CKD or as bridge
Prognosis
- Without treatment, median survival HRS-AKI: ~2 weeks; HRS-CKD: ~4-6 months
- Reversal of HRS is associated with improved survival regardless of modality used
- Patients who do not achieve creatinine reversal within 14 days of vasoconstrictor therapy have very poor outcomes
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), McGraw-Hill
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Saunders
- Comprehensive Clinical Nephrology, 7th Edition, Elsevier
- Goldman-Cecil Medicine International Edition
Recent guideline note: The 2024 AGA Clinical Practice Update (PMID 37978969 - Garcia-Tsao et al., Gastroenterology 2024) addresses the use of vasoactive drugs and IV albumin in cirrhosis, affirming terlipressin + albumin as the primary pharmacological bridge therapy for HRS-AKI.
This is a shared conversation. Sign in to Orris to start your own chat.