GERD from gastro intestinal tract
Reading File
search_medical_text
GERD gastroesophageal reflux disease pathophysiology diagnosis management
search_medical_image
GERD gastroesophageal reflux disease esophagus anatomy
GradeResponse
GradeResponse
Gastroesophageal Reflux Disease (GERD)
Overview
GERD is a family of conditions caused by the reflux of gastric contents into the esophagus, resulting in either troublesome symptoms or esophageal/extraesophageal manifestations. It affects 10–15% of adults in the United States. The spectrum of esophageal injury ranges from esophagitis to adenocarcinoma, with esophageal adenocarcinoma incidence rising two- to sixfold over the past 20 years (~9,200 cases/year in the U.S.) (Harrison's, p. 8868).
Anatomy & Pathophysiology
The key anatomical barrier against reflux is the lower esophageal sphincter (LES), supported by the crural diaphragm. GERD occurs when this barrier fails via:
| Mechanism | Description |
|---|---|
| Transient LES Relaxations (TLESRs) | The most common cause; LES relaxes independent of swallowing, allowing reflux |
| Hypotensive LES | Persistently low resting LES pressure (<10 mmHg) |
| Hiatal Hernia | Displaces the LES above the diaphragm, disrupting the anti-reflux barrier |
| Impaired Esophageal Clearance | Reduced peristalsis prolongs acid exposure time |
| Delayed Gastric Emptying | Increases intragastric pressure and volume |
Clinical Manifestations
Esophageal (Typical) Symptoms
- Heartburn (pyrosis) — substernal burning, the hallmark symptom
- Regurgitation — retrograde flow of gastric contents to mouth/pharynx
- Dysphagia — suggests stricture or motility disorder
- Odynophagia — pain on swallowing, suggests esophagitis
Extraesophageal (Atypical) Symptoms
- Chronic cough, hoarseness, laryngitis
- Non-cardiac chest pain
- Asthma exacerbations
- Dental erosions
- Globus sensation
Complications (Spectrum of Injury)
The GI complications progress along a well-defined spectrum:
- Erosive Esophagitis (EE) — mucosal breaks; graded by Los Angeles (LA) Classification (A–D)
- Peptic Stricture — fibrotic narrowing from chronic acid injury
- Barrett's Esophagus (BE) — intestinal metaplasia of the esophageal mucosa; precancerous
- Esophageal Adenocarcinoma — the most feared complication; highest-risk progression from BE with dysplasia
Diagnosis
1. Clinical Diagnosis
Typical heartburn + regurgitation → empiric PPI trial is sufficient in uncomplicated cases.
2. Upper Endoscopy (EGD) — Indications
- Alarm symptoms: dysphagia, weight loss, bleeding, anemia
- Failure to respond to PPI therapy
- Long-standing GERD (>5 years) to screen for Barrett's esophagus
- Age >60 with new-onset symptoms
3. Ambulatory pH Monitoring (Gold Standard)
- 24-hour pH-impedance testing — measures acid and non-acid reflux events
- Performed off PPI (for diagnosis) or on PPI (for treatment failure assessment)
- Key metric: DeMeester score and percentage time pH <4
4. High-Resolution Manometry (HRM)
- Not diagnostic for GERD but evaluates LES pressure and esophageal motility
- Required before anti-reflux surgery
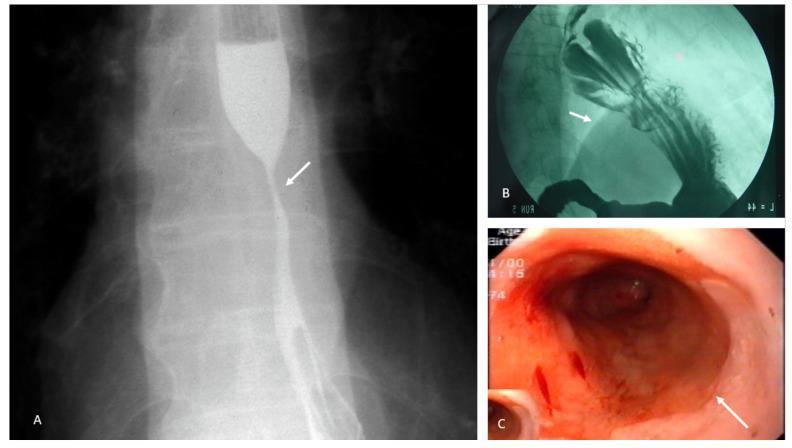
5. Barium Swallow
- Detects hiatal hernia, strictures, and severe reflux
- Low sensitivity; not recommended as primary diagnostic tool
Management
Step 1: Lifestyle Modifications
| Intervention | Rationale |
|---|---|
| Elevate head of bed 6–8 inches | Reduces nocturnal reflux |
| Avoid lying down within 3 hrs of eating | Reduces postprandial reflux |
| Weight loss | Decreases intraabdominal pressure |
| Avoid triggers (fatty foods, caffeine, alcohol, chocolate, mint) | Reduces LES relaxation |
| Smoking cessation | Improves LES tone |
Step 2: Pharmacological Therapy
| Drug Class | Examples | Notes |
|---|---|---|
| PPIs (first-line) | Omeprazole, Pantoprazole, Esomeprazole | Taken 30–60 min before meals; most effective acid suppression |
| H2 Receptor Antagonists | Famotidine, Ranitidine | Second-line or add-on for nocturnal breakthrough |
| Antacids/Alginates | Tums, Gaviscon | Rapid but short-lived symptom relief |
| Prokinetics | Metoclopramide | Rarely used; side-effect profile limits use |
- On-demand PPI for mild/intermittent GERD
- Daily PPI for erosive esophagitis, Barrett's esophagus, or frequent symptoms
- Long-term PPI use: monitor for Mg²⁺/B12 deficiency, bone density, and C. difficile risk
Step 3: Surgical / Procedural Therapy (Refractory GERD)
- Laparoscopic Nissen Fundoplication — gold standard surgical option; wraps gastric fundus 360° around LES
- Partial fundoplication (Toupet/Dor) — preferred when esophageal motility is impaired
- LINX device — magnetic sphincter augmentation; less invasive
- Transoral Incisionless Fundoplication (TIF) — endoscopic option for select patients
Barrett's Esophagus Surveillance
| Finding | Surveillance Interval |
|---|---|
| No dysplasia | Every 3–5 years |
| Low-grade dysplasia | Every 6–12 months or endoscopic eradication therapy |
| High-grade dysplasia | Endoscopic eradication therapy (RFA, EMR) |
Key Differentials
- Peptic ulcer disease (PUD)
- Achalasia / esophageal motility disorder
- Eosinophilic esophagitis (EoE)
- Non-cardiac chest pain / angina
- Functional dyspepsia
- Gastroparesis
Source: Harrison's Principles of Internal Medicine, 21st Edition, p. 8868
This is a shared conversation. Sign in to Orris to start your own chat.