Explain me 10 commen heart diseases with ecg changes and ecg images of those diseases
Reading File
Finding Sources
Searching Images
ECG myocardial infarction ST elevation
Finding Sources
Searching Images
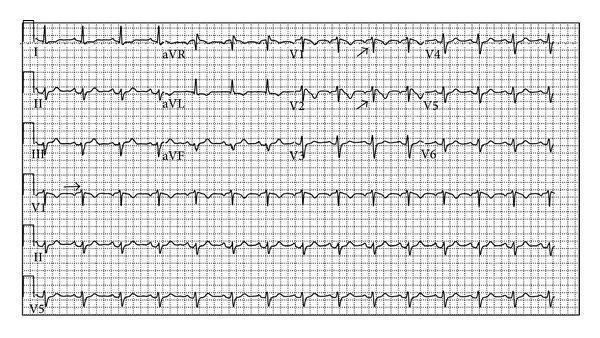
atrial fibrillation ECG irregular rhythm
Reading File
Searching Images
heart block complete AV block ECG bradycardia
Searching Images
ventricular tachycardia ECG wide complex
Searching Images
Wolff-Parkinson-White syndrome ECG delta wave pre-excitation
Searching Images
hypertrophic cardiomyopathy ECG left ventricular hypertrophy
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain
Searching Images
pericarditis ECG saddle-shaped ST elevation diffuse
Searching Images
heart failure dilated cardiomyopathy ECG left bundle branch block
Searching Images
Brugada syndrome ECG right bundle branch coved pattern V1 V2
Here is a comprehensive guide to 10 common heart diseases with their ECG changes and representative ECG images:
10 Common Heart Diseases — ECG Changes & Images
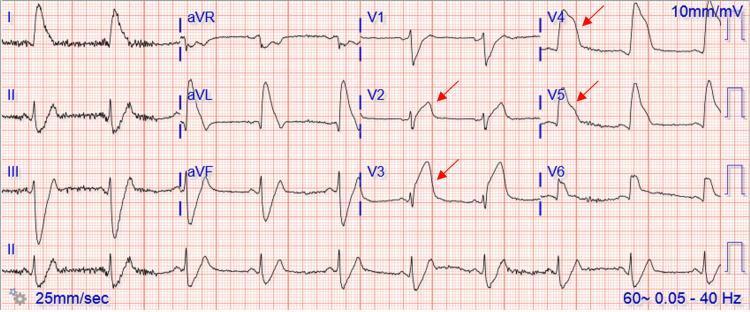
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
ECG Changes
| Phase | Finding |
|---|---|
| Hyperacute | Tall, peaked (hyperacute) T-waves; may precede ST elevation by minutes |
| Acute | Convex (tombstone) ST elevation ≥1 mm in ≥2 contiguous leads in the territory of the occluded artery |
| Evolving | Q-wave formation (pathological Q > 1 mm wide or >25% of R wave); T-wave inversion |
| Reciprocal | ST depression in leads opposite the infarct zone (e.g., inferior STEMI → ST depression in I, aVL) |
Territory Localization
- LAD occlusion → ST elevation in V1–V4 (anterior/anteroseptal)
- RCA occlusion → ST elevation in II, III, aVF (inferior)
- LCx occlusion → ST elevation in I, aVL, V5–V6 (lateral)
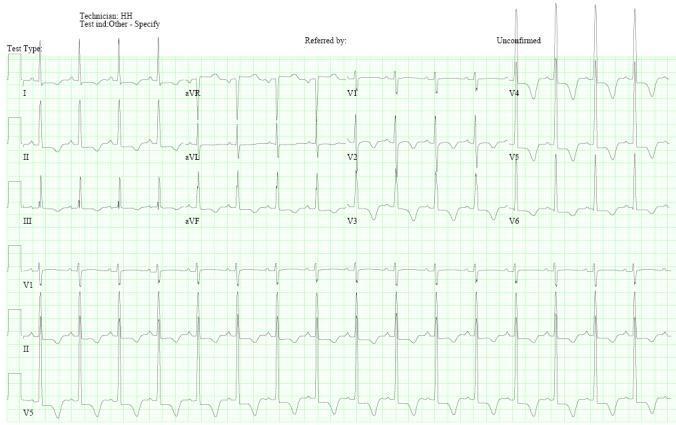
2. ❤️ Atrial Fibrillation (AF)
ECG Changes
- Absent P waves — replaced by chaotic fibrillatory (f) waves, most visible in V1 and lead II
- Irregularly irregular RR intervals (no two RR intervals are identical)
- Narrow QRS complexes (unless aberrant conduction or accessory pathway is present)
- Ventricular rate typically 100–160 bpm in uncontrolled AF (tachycardic response)
- Fibrillatory baseline best seen as "dirty" or undulating isoelectric line

3. 🔴 Complete (Third-Degree) AV Heart Block
ECG Changes
- Complete AV dissociation — P waves and QRS complexes march independently at different rates
- Atrial rate > ventricular rate (P waves are faster)
- No fixed PR interval — P waves bear no relationship to QRS complexes
- Escape rhythm character depends on escape focus:
- Junctional escape: narrow QRS ~40–60 bpm
- Ventricular escape: wide QRS (RBBB/LBBB morphology) ~20–40 bpm
- Prolonged QTc may be present

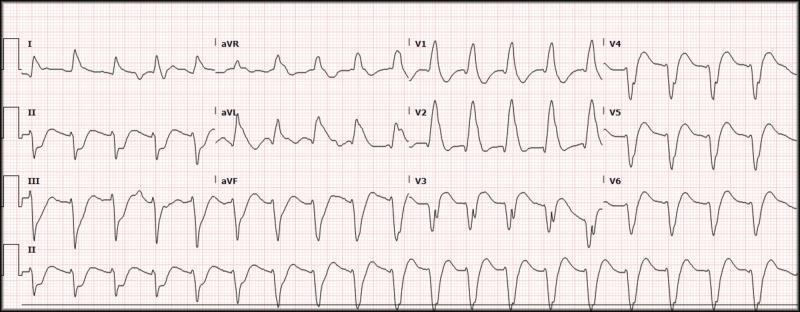
4. ⚡ Ventricular Tachycardia (VT)
ECG Changes
- Wide QRS tachycardia — QRS duration >120 ms (often >160 ms), rate 100–250 bpm
- AV dissociation — P waves present at slower rate, unrelated to QRS (hallmark of VT)
- Fusion beats — partial ventricular capture creating a "hybrid" QRS (diagnostic of VT)
- Capture beats — normal narrow QRS intermittently (sinus captures ventricle briefly)
- Concordance — all precordial leads point in same direction (positive or negative = VT)
- Monomorphic VT: all QRS complexes are identical
- Polymorphic VT (Torsades): sinusoidal twisting QRS axis around baseline
5. 💙 Wolff-Parkinson-White (WPW) Syndrome
ECG Changes
- Short PR interval (<120 ms) — accessory pathway bypasses AV node delay
- Delta wave — slurred, slow upstroke at the beginning of the QRS complex
- Widened QRS (>120 ms total) due to ventricular pre-excitation
- Secondary ST-T changes — discordant to delta wave direction
- Pseudo-infarct pattern — negative delta waves in inferior leads can mimic Q waves
- Pathway localization: delta wave polarity in specific leads localizes the accessory pathway
- Negative delta in II, III, aVF → posterior/posteroseptal pathway
- Positive delta in V1 → left lateral pathway

6. 🫁 Acute Pulmonary Embolism (PE)
ECG Changes
- Sinus tachycardia — most common finding (>50% of cases)
- S1Q3T3 pattern — prominent S-wave in lead I, Q-wave in lead III, T-wave inversion in lead III (right heart strain sign)
- Right axis deviation — axis shifts rightward due to acute RV pressure overload
- Incomplete/complete RBBB — conduction delay in the RV
- T-wave inversions in V1–V4 — anterior RV strain
- P pulmonale — tall peaked P waves in II (>2.5 mm) — right atrial dilation
- Normal ECG does NOT rule out PE

7. 🧡 Hypertrophic Cardiomyopathy (HCM)
ECG Changes
- LVH voltage criteria — Sokolow-Lyon: S(V1) + R(V5/V6) >35 mm
- Giant T-wave inversions (deep symmetric) in precordial leads V1–V6 — especially in apical HCM (Yamaguchi syndrome)
- ST-segment depression — "strain pattern" in lateral leads
- Absent septal Q waves in I, aVL, V5–V6 (reversed septal depolarization)
- Abnormal Q waves in inferior and/or lateral leads (simulating prior MI)
- Atrial fibrillation may develop with disease progression
8. 💚 Acute Pericarditis
ECG Changes (4 Classic Stages)
| Stage | Finding |
|---|---|
| Stage I | Diffuse concave (saddle-shaped) ST elevation in all leads except aVR and V1; PR depression in same leads; PR elevation in aVR |
| Stage II | ST returns to baseline; T waves flatten |
| Stage III | Diffuse T-wave inversions |
| Stage IV | Normalization (may take weeks) |
- Spodick's sign — downsloping TP segment in multiple leads
- No reciprocal ST depression (unlike STEMI) — helps differentiate from MI
- No Q waves (no myocardial necrosis)

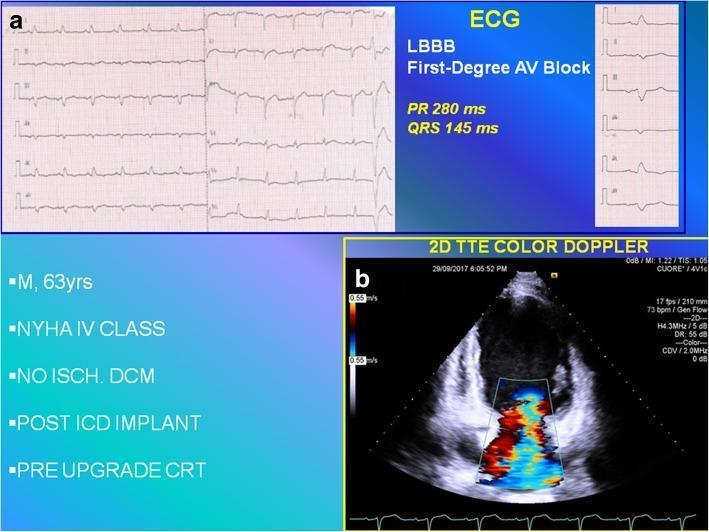
9. 🩵 Dilated Cardiomyopathy (DCM) / Heart Failure
ECG Changes
- Left Bundle Branch Block (LBBB) — most characteristic; wide QRS >120 ms, broad monophasic R in I, aVL, V5–V6; deep QS in V1–V3
- First-degree AV block — prolonged PR interval (>200 ms)
- Poor R-wave progression in precordial leads (simulates anterior MI)
- Left axis deviation
- Non-specific ST-T changes — secondary repolarization abnormalities
- Atrial fibrillation — common in advanced DCM
- Ventricular ectopy / NSVT — reflects myocardial remodeling
10. 🟣 Brugada Syndrome
ECG Changes
- Type 1 (Diagnostic) — "Coved" ST elevation ≥2 mm in V1–V2, with a downward convex slope into inverted T-wave with no isoelectric separation (pathognomonic)
- Type 2 ("Saddle-back") — ST elevation ≥2 mm but with a positive/biphasic T-wave — not diagnostic alone
- Pseudo-RBBB pattern — rSr' in V1–V2 mimicking RBBB
- Pattern may be concealed (only appears after sodium channel blockers: ajmaline, flecainide, procainamide challenge)
- Associated with ventricular fibrillation and sudden cardiac death, especially at rest/sleep
- SCN5A gene mutation (cardiac sodium channel) in ~25% of cases
Quick Reference Summary Table
| # | Disease | Key ECG Feature |
|---|---|---|
| 1 | STEMI | Convex ST elevation + reciprocal changes + Q waves |
| 2 | Atrial Fibrillation | No P waves, irregularly irregular RR |
| 3 | Complete Heart Block | P-QRS dissociation, escape rhythm |
| 4 | Ventricular Tachycardia | Wide QRS, AV dissociation, fusion beats |
| 5 | WPW Syndrome | Short PR, delta wave, wide QRS |
| 6 | Pulmonary Embolism | S1Q3T3, sinus tachycardia, RBBB pattern |
| 7 | Hypertrophic Cardiomyopathy | LVH voltage, giant T-wave inversions |
| 8 | Acute Pericarditis | Diffuse concave ST elevation, PR depression |
| 9 | Dilated Cardiomyopathy | LBBB, poor R progression, AF |
| 10 | Brugada Syndrome | Coved ST elevation V1–V2, pseudo-RBBB |
Sources: Braunwald's Heart Disease (9th/12th ed.), Rosen's Emergency Medicine — ECG interpretation sections; ECG images from peer-reviewed clinical literature (PMC).
All understood in gujrati
૧૦ સામાન્ય હૃદય રોગો — ECG ફેરફારો અને ચિત્રો સાથે
૧. 🫀 ST-એલિવેશન મ્યોકાર્ડિયલ ઇન્ફાર્ક્શન (STEMI) — હૃદયનો હુમલો
ECG ફેરફારો
| તબક્કો | ફેરફાર |
|---|---|
| તીવ્ર શરૂઆત | ઊંચા, નુકીળા T-waves (hyperacute T) |
| તીવ્ર તબક્કો | ST elevation — ઉપર ઊઠેલું ST segment (ટોમ્બસ્ટોન આકાર) |
| વિકસતો તબક્કો | Q-wave બને — હૃદયના સ્નાયુ મૃત્યુની નિશાની; T-wave ઊંધું થાય |
| સામેની બાજુ | Reciprocal ST depression — વિરુદ્ધ leads માં ST નીચે જાય |
કઈ ધમની બંધ — ક્યાં ફેરફાર
- LAD (આગળની ધમની) → V1–V4 માં ST elevation
- RCA (નીચેની ધમની) → II, III, aVF માં ST elevation
- LCx (બાજુની ધમની) → I, aVL, V5–V6 માં ST elevation
૨. ❤️ એટ્રિયલ ફિબ્રિલેશન (AF) — હૃદયની ઉપરની ચેમ્બરની ધ્રૂજારી
ECG ફેરફારો
- P-wave ગાયબ — નિયમિત P-waves દેખાતા નથી; ની જગ્યાએ ધ્રૂજતી (fibrillatory) baseline
- અનિયમિત-અનિયમિત RR અંતર — દરેક ધબકારો અલગ-અલગ સમયે
- સાંકડા QRS complexes (સામાન્ય)
- હૃદયના ધબકારા ઝડપી: ૧૦૦–૧૬૦ per minute (uncontrolled)
- V1 lead માં "ગંદી" baseline સ્પષ્ટ દેખાય
૩. 🔴 સંપૂર્ણ AV હાર્ટ બ્લોક (Third-Degree Heart Block)
ECG ફેરફારો
- P-wave અને QRS સ્વતંત્ર — બંને અલગ-અલગ ગતિથી ચાલે, કોઈ સંબંધ નહીં
- Atrial rate > Ventricular rate — P-waves ઝડપી, QRS ધીમા
- PR interval સ્થિર નહીં — P અને QRS વચ્ચેનું અંતર બદલાતું રહે
- Escape rhythm:
- Junctional: સાંકડો QRS ~40–60 bpm
- Ventricular: પહોળો QRS ~20–40 bpm
- QTc interval લંબાઈ શકે
૪. ⚡ વેન્ટ્રિક્યુલર ટેકિકાર્ડિયા (VT)
ECG ફેરફારો
- પહોળો QRS — QRS >120 ms (ઘણીવાર >160 ms); ઝડપ 100–250 bpm
- AV dissociation — P-waves ધીમા, QRS ઝડપા, કોઈ સંબંધ નહીં (VT ની સૌથી ચોક્કસ નિશાની)
- Fusion beats — સામાન્ય + VT QRS ભળે (VT સાબિત કરે)
- Capture beats — સાઇનસ rhythm ક્ષણ માટે ventricle ને capture કરે
- Concordance — બધી chest leads એક જ દિશામાં (ઉપર/નીચે)
- Monomorphic VT: દરેક QRS સરખો
- Polymorphic VT (Torsades): QRS dhuri ફરે
૫. 💙 વુલ્ફ-પાર્કિન્સન-વ્હાઇટ સિન્ડ્રોમ (WPW)
ECG ફેરફારો
- ટૂંકો PR interval (<120 ms) — accessory pathway AV node ને bypass કરે
- Delta wave — QRS ના શરૂઆતમાં ધીમો, slurred ઉભાર (ચોક્કસ નિશાની)
- પહોળો QRS (>120 ms) — early ventricular activation ના કારણે
- ST-T ફેરફારો — secondary, delta wave ની વિરુદ્ધ દિશામાં
- Pseudo-infarct — inferior leads માં negative delta waves MI જેવા Q-wave બનાવે
- Delta wave ની polarity pathway ની location બતાવે
૬. 🫁 તીવ્ર પલ્મોનરી એમ્બોલિઝમ (PE) — ફેફસાની ધમની બ્લોક
ECG ફેરફારો
- Sinus tachycardia — સૌથી સામાન્ય (>50% cases)
- S1Q3T3 pattern — Lead I માં deep S-wave + Lead III માં Q-wave + Lead III માં inverted T-wave (જમણા હૃદય પર ભાર)
- Right axis deviation — axis જમણી બાજુ
- Incomplete/complete RBBB — RV conduction delay
- V1–V4 માં T-wave inversion — anterior RV strain
- P pulmonale — lead II માં ઊંચા P-waves (right atrium ફૂલ્યો)
- ⚠️ Normal ECG PE ને નકારી ન શકે
૭. 🧡 હાઇપરટ્રોફિક કાર્ડિઓમાયોપથી (HCM) — જાડું હૃદય
ECG ફેરફારો
- LVH voltage — Sokolow-Lyon: S(V1) + R(V5/V6) >35 mm
- Giant T-wave inversions — ઊંડા, symmetric inverted T-waves V1–V6 (ખાસ કરીને apical HCM / Yamaguchi syndrome)
- ST depression — lateral leads માં "strain pattern"
- Absent septal Q waves — I, aVL, V5–V6 માં septal Q-waves ગાયબ
- Abnormal Q waves — inferior/lateral leads — MI ની નકલ
- AF: રોગ વધતા atrial fibrillation થઈ શકે
૮. 💚 તીવ્ર પેરિકાર્ડિટિસ — હૃદયના આવરણની સોજ
ECG ફેરફારો — ૪ ક્લાસિક તબક્કા
| તબક્કો | ફેરફાર |
|---|---|
| Stage I | Diffuse concave (saddle-shaped) ST elevation — aVR અને V1 સિવાય બધા leads; PR depression (inflammatory signature); aVR માં PR elevation |
| Stage II | ST baseline પર આવે; T-waves flat થાય |
| Stage III | Diffuse T-wave inversions |
| Stage IV | Normalization (અઠવાડિયા લાગે) |
- Spodick's sign — TP segment નીચે ઢળે
- Reciprocal ST depression નહીં — STEMI થી અલગ
- Q-waves નહીં — myocardium નષ્ટ નથી
૯. 🩵 ડાઇલેટેડ કાર્ડિઓમાયોપથી (DCM) / હૃદય નિષ્ફળતા
ECG ફેરફારો
- Left Bundle Branch Block (LBBB) — સૌથી ખાસ; QRS >120 ms; I, aVL, V5–V6 માં broad monophasic R; V1–V3 માં deep QS
- First-degree AV block — PR interval >200 ms
- Poor R-wave progression — precordial leads માં — anterior MI ની નકલ
- Left axis deviation
- Non-specific ST-T changes — secondary repolarization abnormalities
- Atrial fibrillation — advanced DCM માં
- Ventricular ectopy / NSVT — myocardial remodeling ની નિશાની
૧૦. 🟣 બ્રુગાડા સિન્ડ્રોમ — આનુવંશિક વીજળી ખામી
ECG ફેરફારો
- Type 1 (Diagnostic — "Coved type") — V1–V2 માં ≥2 mm ST elevation; ઉપરથી નીચે convex ઢળણ → inverted T-wave (isoelectric gap નહીં) — pathognomonic
- Type 2 ("Saddle-back") — ST elevation ≥2 mm પણ T-wave positive/biphasic — એકલું diagnostic નહીં
- Pseudo-RBBB — V1–V2 માં rSr' pattern
- Pattern concealed રહી શકે — sodium channel blockers (ajmaline/flecainide) થી unmask
- Ventricular fibrillation અને sudden cardiac death નો ભય — ખાસ ઊંઘ/આરામ દરમ્યાન
- SCN5A gene mutation — ~25% cases
⚡ ઝડપી સંદર્ભ કોષ્ટક
| # | રોગ | ECG ની ખાસ નિશાની |
|---|---|---|
| ૧ | STEMI | Convex ST elevation + Q-waves + Reciprocal changes |
| ૨ | Atrial Fibrillation | P-waves ગાયબ, અનિયમિત-અનિયમિત RR |
| ૩ | Complete Heart Block | P-QRS dissociation, escape rhythm |
| ૪ | Ventricular Tachycardia | Wide QRS, AV dissociation, fusion beats |
| ૫ | WPW Syndrome | Short PR, Delta wave, Wide QRS |
| ૬ | Pulmonary Embolism | S1Q3T3, Sinus tachycardia, RBBB pattern |
| ૭ | Hypertrophic Cardiomyopathy | LVH voltage, Giant T-wave inversions |
| ૮ | Acute Pericarditis | Diffuse concave ST elevation, PR depression |
| ૯ | Dilated Cardiomyopathy | LBBB, Poor R progression, AF |
| ૧૦ | Brugada Syndrome | Coved ST elevation V1–V2, Pseudo-RBBB |
સ્ત્રોત: Braunwald's Heart Disease, Rosen's Emergency Medicine — ECG વિભાગ; ECG ચિત્રો peer-reviewed clinical literature (PMC) માંથી.
This is a shared conversation. Sign in to Orris to start your own chat.