definition , etiopathogenesis ( chart form ) , clinical features / triads , diagnosis ( gold standard investigation , MANAGEMENT ( NON PHARMACOLOGICAL ) , PHARMACOLOGICAL (TABLE FORM ) WITH DRUG NAME , DRUG CLASS , ITS DOSAGE OF NON ALCOHOLIC FATTY LIVER DISEASE.
"nonalcoholic fatty liver disease" AND management
Non-Alcoholic Fatty Liver Disease (NAFLD)
1. DEFINITION
| Stage | Description |
|---|---|
| NAFL (Simple Steatosis) | Macrovesicular steatosis only, no ballooning or fibrosis - benign course |
| NASH (Nonalcoholic Steatohepatitis) | Steatosis + ballooning degeneration + inflammation ± fibrosis |
| NASH-Cirrhosis | End-stage fibrosis (F4); risk of HCC and liver failure |
Prevalence: ~25% globally; ~30% of U.S. adults; up to 90% of morbidly obese individuals.
2. ETIOPATHOGENESIS (Chart Form)
Primary Risk Factors / Triggers
OBESITY / TYPE 2 DIABETES / METABOLIC SYNDROME / DYSLIPIDEMIA
|
▼
INSULIN RESISTANCE + HYPERINSULINEMIA
|
┌───────────────┼────────────────────┐
▼ ▼ ▼
↑ Adipose ↑ De novo ↑ Dietary free
lipolysis lipogenesis fatty acid intake
| | |
└───────────────┴────────────────────┘
|
▼
EXCESSIVE FREE FATTY ACIDS → HEPATOCYTES
|
▼
MACROVESICULAR STEATOSIS (NAFL)
|
┌────────────┴───────────────────┐
▼ ▼
LIPOTOXICITY (unesterified FFAs) CONTINUED METABOLIC STRESS
|
┌─────────┴─────────────────────┐
▼ ▼ ▼
Oxidative ER stress / Apoptosis
stress Mitochondrial
(ROS) dysfunction
|
┌─────────┴──────────┐
▼ ▼
Adipocytokines Gut dysbiosis /
(↓ Adiponectin, altered bile acids
↑ TNF-α, ↑ IL-6)
|
▼
HEPATIC INFLAMMATION + BALLOONING (NASH)
|
▼
Sonic hedgehog ↑ → Hepatic stellate cell activation
|
▼
SINUSOIDAL FIBROSIS → CIRRHOSIS → HCC
Genetic Modifiers
| Gene | Effect |
|---|---|
| PNPLA3 (rs738409:G) | ↑ severity of steatosis and fibrosis |
| TM6SF2 | ↑ NAFLD risk |
| GCKR | ↑ hepatic lipogenesis |
| MBOAT7 | ↑ NAFLD risk |
| HSD17B13 | Protective - reduces NAFLD severity |
Other Associations / Secondary Causes
| Category | Conditions |
|---|---|
| Endocrine | PCOS, hypothyroidism, hypopituitarism, hypogonadism |
| Sleep | Obstructive sleep apnea |
| Medications | Amiodarone, methotrexate, tamoxifen, corticosteroids |
| Gut | Dysbiosis, altered microbiome |
3. CLINICAL FEATURES / TRIADS
The Classic NASH Triad (Histological)
Steatosis + Ballooning Degeneration + Lobular Inflammation
| Feature | Details |
|---|---|
| 1. Hepatocyte Ballooning | Swollen, pale hepatocytes with cleared cytoplasm - hallmark of hepatocyte injury |
| 2. Macrovesicular Steatosis | Large fat vacuoles displacing nucleus to periphery (>5% hepatocytes) - predominantly centrilobular |
| 3. Lobular Inflammation | Mixed inflammatory infiltrate; ± Mallory-Denk hyaline bodies, neutrophilic infiltration |
Symptoms and Signs by Stage
| Feature | Simple Steatosis (NAFL) | NASH | Cirrhosis/Advanced |
|---|---|---|---|
| Symptoms | Often asymptomatic | Fatigue, vague RUQ discomfort, nausea | Ascites, encephalopathy |
| Hepatomegaly | May be present | Present | Present ± nodular |
| Palmar erythema | Absent | May be present | Present |
| Spider nevi | Absent | Rare | Present |
| Jaundice | Absent | Absent | Present (late) |
| Abdominal collaterals | Absent | Absent | Present (portal HTN) |
| Low platelet count | Normal | Normal | Reduced (hypersplenism) |
Laboratory Features
| Test | Finding |
|---|---|
| ALT, AST | Elevated (ALT > AST - opposite of alcoholic hepatitis); rarely >250 IU/L |
| ALT:AST ratio | >1 (unlike alcoholic hepatitis where AST:ALT >2) |
| Ferritin | Mildly elevated (hyperferritinemia) |
| ANA / ASMA | Low-grade positivity (not diagnostic of autoimmune hepatitis) |
| GGT, ALP | May be mildly elevated |
| Lipid profile | Dyslipidemia common |
| Fasting glucose / HbA1c | Elevated in many (insulin resistance / T2DM) |
4. DIAGNOSIS
Gold Standard Investigation
Percutaneous Liver Biopsy - the definitive test for diagnosing NASH, staging fibrosis, and distinguishing NASH from simple steatosis.
NAFLD Activity Score (NAS) on Biopsy
| Component | Score |
|---|---|
| Steatosis (0-3) | 0 = <5%, 1 = 5-33%, 2 = 34-66%, 3 = >66% |
| Lobular inflammation (0-3) | 0-3 based on inflammatory foci |
| Hepatocyte ballooning (0-2) | 0 = none, 1 = few, 2 = many |
| NAS ≥ 5 | Consistent with NASH |
Fibrosis Staging (Metavir / Brunt)
| Stage | Description |
|---|---|
| F0 | No fibrosis |
| F1 | Perisinusoidal or periportal fibrosis |
| F2 | Both perisinusoidal AND portal/periportal |
| F3 | Bridging fibrosis |
| F4 | Cirrhosis |
Diagnostic Algorithm
| Step | Investigation | Finding |
|---|---|---|
| 1. Exclude alcohol / drugs / viral hepatitis | History + Serology (HBsAg, anti-HCV) | Negative |
| 2. Liver enzymes | ALT, AST, GGT, ALP | ALT > AST; rarely >250 IU/L |
| 3. Screen for metabolic syndrome | FBG, HbA1c, lipid profile, BMI | Often abnormal |
| 4. Imaging (1st line) | Abdominal Ultrasound | Echogenic / bright liver (PPV 77%) |
| 5. Advanced imaging | MRI / MR Spectroscopy | Most accurate non-invasive (limited by cost) |
| 6. Non-invasive fibrosis | Vibration-Controlled Transient Elastography (FibroScan) | Estimates liver stiffness / fibrosis |
| 7. Gold Standard | Percutaneous Liver Biopsy | Confirms NASH, grades inflammation, stages fibrosis |
- Persistently elevated aminotransferases
- Unable to exclude a competing diagnosis (iron overload, autoimmune hepatitis)
- Clinical suspicion of NASH with advanced fibrosis
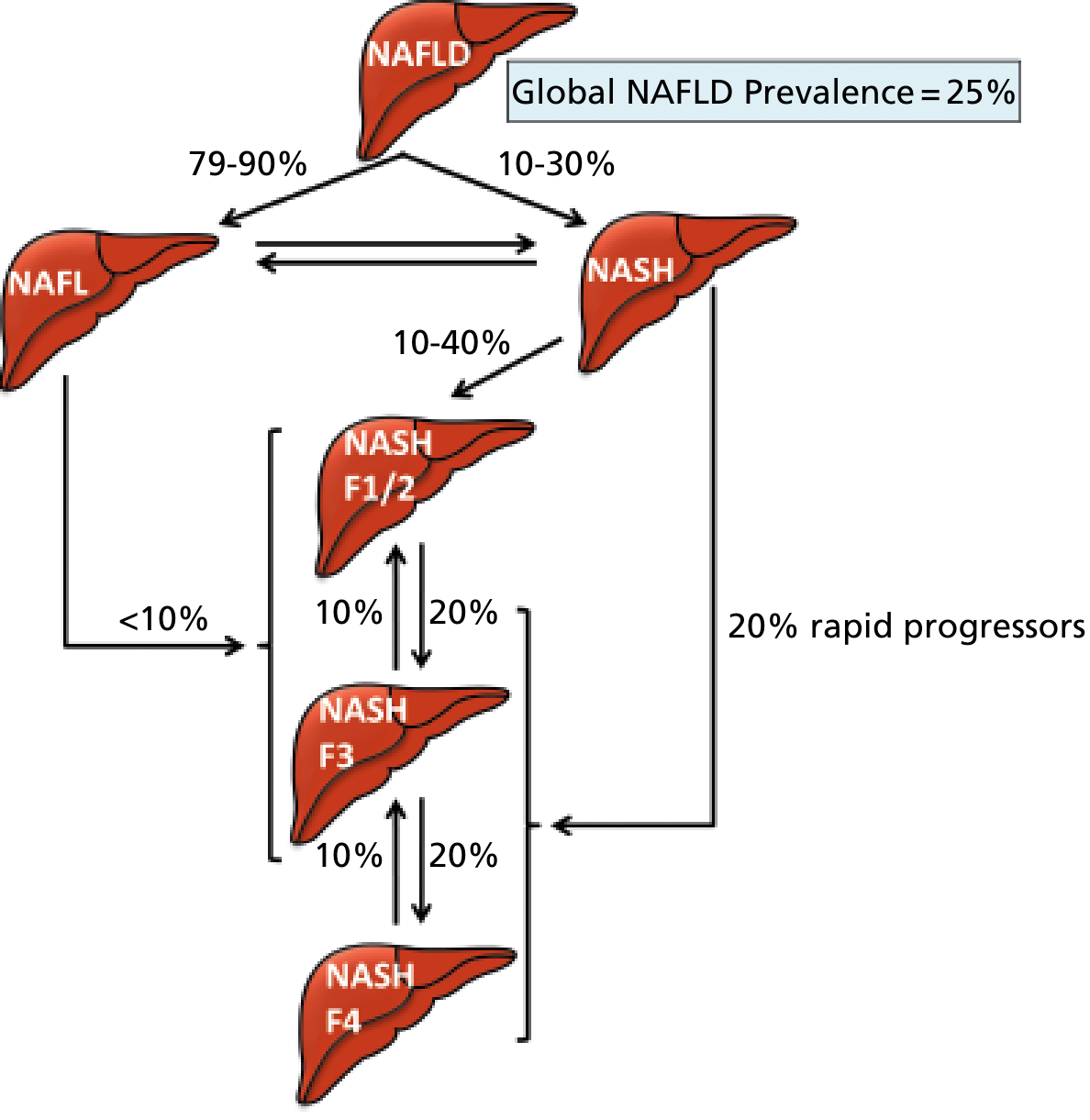
5. NAFLD Disease Progression
6. MANAGEMENT
A. NON-PHARMACOLOGICAL MANAGEMENT
1. Dietary Modification
| Recommendation | Detail |
|---|---|
| Weight loss target | 10% body weight reduction (gradual); minimum 5% for histological improvement in steatosis and inflammation; >10% for fibrosis resolution |
| Caloric restriction | 500-1000 kcal/day deficit from baseline intake |
| Low refined-sugar diet | Reduce fructose (soft drinks, processed foods) and simple carbohydrates |
| Avoid saturated fats | Replace with unsaturated fats; Mediterranean diet preferred |
| Avoid alcohol | Complete abstinence strongly recommended |
| Fructose restriction | High-fructose corn syrup specifically implicated in de novo lipogenesis |
2. Physical Activity / Exercise
| Recommendation | Detail |
|---|---|
| Aerobic exercise | 150-200 min/week of moderate intensity (brisk walking, cycling, swimming) |
| Resistance training | Adds additional benefit to aerobic exercise for insulin sensitivity |
| Reduce sedentary time | Break up prolonged sitting; physical activity independent of weight loss improves liver fat |
3. Behavioral / Multidisciplinary Approach
| Component | Detail |
|---|---|
| Behavioral therapy | Cognitive behavioral strategies for lifestyle change |
| Dietitian/Nutritionist | Structured dietary counseling more effective than prescriptive advice |
| Exercise specialist | Supervised exercise program |
| Monitoring | Regular follow-up with BMI, LFTs, imaging |
4. Bariatric Surgery (for Morbidly Obese)
| Indication | Outcome |
|---|---|
| BMI >40, or >35 with comorbidities | Resolves liver biopsy findings in ~80% of patients; progressive reduction in fibrosis |
| Pre-requisite | Must exclude portal hypertension before surgery |
| Recurrence risk | NAFLD can recur post-transplant if metabolic factors persist |
5. Cardiovascular Risk Management
- Treat dyslipidemia aggressively (statins are safe in NAFLD/NASH)
- Manage hypertension and T2DM
- Coronary artery disease is the most common cause of death in NAFLD
B. PHARMACOLOGICAL MANAGEMENT (Table Form)
| Drug Name | Drug Class | Dosage | Indication / Notes |
|---|---|---|---|
| Vitamin E (α-tocopherol) | Antioxidant | 800 IU/day orally for ≥2 years | Improves liver enzymes and histology in non-diabetic NASH; first-line pharmacotherapy in non-diabetic NASH (AASLD) |
| Pioglitazone | Thiazolidinedione (insulin sensitizer / PPARγ agonist) | 30-45 mg/day orally | Improves steatosis, inflammation, ballooning, and possibly fibrosis; use with caution - causes ~4.5 kg weight gain; avoid in T2DM patients with heart failure |
| Rosiglitazone | Thiazolidinedione (PPARγ agonist) | 4-8 mg/day orally | Similar mechanism to pioglitazone; weight gain side effect offsets histologic benefit; less favored due to cardiovascular concerns |
| Liraglutide | GLP-1 receptor agonist | 1.8 mg/day subcutaneous injection | Histologic resolution of NASH; improves steatosis, inflammation, and hepatocyte ballooning; also aids weight loss |
| Semaglutide | GLP-1 receptor agonist | 0.4 mg/day subcutaneous (for 72 weeks) | Highly effective in resolving steatohepatitis; does not significantly improve fibrosis in NASH with clinically significant fibrosis |
| Resmetirom (Rezdiffra) | Thyroid hormone receptor-β (THR-β) selective agonist | 80 mg orally twice daily | First FDA-approved drug specifically for NASH (2024); reduces hepatic fat and improves NASH histology; liver-directed action |
| Atorvastatin | HMG-CoA reductase inhibitor (Statin) | 20 mg/day orally | Treats dyslipidemia and reduces cardiovascular risk; improves liver test results; safe to use in NAFLD/NASH |
| Obeticholic acid (OCA) | FXR (Farnesoid X receptor) agonist | 25 mg/day orally | Histologic improvement in NASH; not yet fully approved for NASH (under ongoing study); note - can worsen pruritus and dyslipidemia |
| Lanifibranor | Pan-PPAR agonist (PPARα/γ/δ) | 1200 mg/day orally | Improves inflammatory components of NASH; may reduce fibrosis; in clinical trials |
| Pentoxifylline | Phosphodiesterase inhibitor / TNF-α antagonist | 400 mg three times daily | Improves liver enzymes and histologic findings in NASH; anti-inflammatory mechanism via TNF-α inhibition |
| Omega-3 polyunsaturated fatty acids | Lipid-modifying agent | 2-4 g/day orally | Reduces hepatic triglycerides and dyslipidemia; beneficial in small controlled trials; adjunct therapy |
| Metformin | Biguanide (insulin sensitizer) | 500-2000 mg/day orally | Improves insulin resistance; indirect benefit on liver fat; standard care if T2DM co-exists; not directly proven to improve NASH histology in non-diabetic patients |
Note on recent FDA approval: Resmetirom (Rezdiffra) received FDA approval in March 2024 as the first drug specifically indicated for NASH with liver fibrosis (F2-F3 stage), based on the MAESTRO-NASH trial (PMID: 38697306 - systematic review/meta-analysis supports its efficacy).
7. Liver Biopsy - Histology of NASH
Quick Summary Box
| Domain | Key Point |
|---|---|
| Definition | Hepatic steatosis (>5% hepatocytes) without alcohol, drugs, or other causes |
| Hallmark triad (NASH) | Steatosis + Ballooning + Lobular inflammation |
| Gold standard diagnosis | Percutaneous liver biopsy |
| Non-pharm cornerstone | Weight loss ≥10% body weight + exercise |
| First-line pharmacotherapy | Vitamin E (non-diabetic NASH); Pioglitazone (diabetic NASH) |
| Newest approved drug | Resmetirom (THR-β agonist) - FDA approved 2024 |
| Most common cause of death | Cardiovascular disease (in NAFLD); liver-related (in NASH with cirrhosis) |
| Prognosis | Simple steatosis - benign; NASH - 20% develop cirrhosis over 10-15 years |
- Goldman-Cecil Medicine International Edition (2-Volume Set), pp. 1610-1612
- Yamada's Textbook of Gastroenterology, 7th ed., pp. 2229-2230
- Robbins & Kumar Basic Pathology, p. 635
- Tintinalli's Emergency Medicine, p. 235-237
- PubMed: Dutta D et al., Endocr Pract 2024 (Resmetirom meta-analysis, PMID: 38697306)
definition , etiopathogenesis ( chart form ) , clinical features / triads , diagnosis ( gold standard investigation , MANAGEMENT ( NON PHARMACOLOGICAL ) , PHARMACOLOGICAL (TABLE FORM ) WITH DRUG NAME , DRUG CLASS , ITS DOSAGE OF NON ALCOHOLIC STEATO HEPATITIS
"nonalcoholic steatohepatitis" AND treatment
Non-Alcoholic Steatohepatitis (NASH)
Note on Nomenclature: In 2023, major hepatology societies (AASLD, EASL) adopted new terminology - NASH is now called MASH (Metabolic dysfunction-Associated SteatoHepatitis), and NAFLD is now called MASLD (Metabolic dysfunction-Associated Steatotic Liver Disease). Both terms are used interchangeably in current literature.
1. DEFINITION
- Macrovesicular hepatic steatosis (>5% of hepatocytes)
- Hepatocyte ballooning degeneration (cytological injury)
- Lobular inflammation (with or without fibrosis)
"NASH is a more advanced form of NAFLD, histologically characterized by macrovesicular steatosis, ballooning degeneration of hepatocytes, and sinusoidal fibrosis." - Goldman-Cecil Medicine
2. ETIOPATHOGENESIS (Chart Form)
The "Multiple-Hit" Hypothesis
════════════════════════════════════════════════════
PREDISPOSING RISK FACTORS (FIRST HIT)
════════════════════════════════════════════════════
Obesity → Type 2 Diabetes → Metabolic Syndrome
Dyslipidemia → Sedentary lifestyle → Excess caloric intake
Genetic factors (PNPLA3, TM6SF2, MBOAT7, GCKR)
│
▼
════════════════════════════════════════════════════
INSULIN RESISTANCE + HYPERINSULINEMIA
════════════════════════════════════════════════════
│ │
▼ ▼
↑ Adipose tissue ↑ De novo lipogenesis
lipolysis → ↑ FFA in liver (via SREBP-1c)
delivery to liver
│ │
└───────────┬─────────────┘
▼
════════════════════════════════════════════════════
HEPATIC STEATOSIS (SIMPLE STEATOSIS)
Macrovesicular fat in >5% of hepatocytes
(predominantly zone 3 / centrilobular)
════════════════════════════════════════════════════
│
─────────────────────────────
SECOND HITS (Multiple Parallel Insults)
─────────────────────────────
┌─────────┬───────────┬────────────┬──────────┐
▼ ▼ ▼ ▼ ▼
Oxidative Endo- Lipotoxicity Adipocyto- Gut
stress plasmic (unester- kines dysbiosis
(ROS from reticulum ified FFAs ↓ Adiponec- & altered
mitochondria/stress & ceramides) tin bile acid
microsomes) apoptosis ↑ TNF-α signaling
↑ IL-6, IL-1β
└─────────┴───────────┴────────────┴──────────┘
│
▼
════════════════════════════════════════════════════
HEPATOCELLULAR INJURY + BALLOONING
Sonic hedgehog ↑ from ballooned hepatocytes
│
▼
HEPATIC STELLATE CELL ACTIVATION (TGF-β ↑)
│
▼
════════════════════════════════════════════════════
NASH (STEATOHEPATITIS)
Steatosis + Ballooning + Lobular Inflammation
════════════════════════════════════════════════════
│
▼
PROGRESSIVE SINUSOIDAL FIBROSIS
F1 → F2 → F3 (Bridging) → F4 (CIRRHOSIS)
│
▼
HEPATOCELLULAR CARCINOMA (HCC)
════════════════════════════════════════════════════
Specific Pathogenic Mechanisms
| Mechanism | Detail |
|---|---|
| Insulin resistance | Impairs suppression of lipolysis → excess FFA to liver; promotes de novo lipogenesis via SREBP-1c |
| Lipotoxicity | Unesterified FFAs, diacylglycerols, ceramides directly injure hepatocytes |
| Oxidative stress | ROS from mitochondrial β-oxidation and CYP2E1 microsomes cause DNA damage |
| ER stress | Activates unfolded protein response → apoptosis (JNK pathway) |
| Adipocytokines | ↓ Adiponectin (anti-fibrotic, anti-inflammatory), ↑ TNF-α, ↑ IL-6 → inflammation |
| Gut dysbiosis | Altered microbiome → ↑ LPS → Toll-like receptor 4 activation → NF-κB → inflammation |
| Sonic hedgehog | Released by ballooned hepatocytes → activates hepatic stellate cells → fibrosis |
| TGF-β | Key fibrogenic cytokine from stellate cells → collagen deposition |
Genetic Risk Factors
| Gene | Variant | Effect |
|---|---|---|
| PNPLA3 | I148M (rs738409) | Strongest genetic risk; ↑ hepatic fat & fibrosis; most prevalent in Hispanics |
| TM6SF2 | E167K (rs58542926) | ↑ NASH severity and fibrosis risk |
| MBOAT7 | rs641738 | ↑ Steatosis and disease severity |
| GCKR | Variant | ↑ Hepatic lipogenesis |
| HSD17B13 | rs72613567:TA | Protective - lower odds of NASH, fibrosis, and NASH cirrhosis |
| KLF6, NCAN, LYPLA1 | Various | Associated with NAFLD spectrum (evidence evolving) |
Secondary / Drug-Induced Causes of Steatohepatitis
| Category | Examples |
|---|---|
| Steatogenic drugs | Amiodarone, methotrexate, tamoxifen, corticosteroids, HAART |
| Endocrine | PCOS, hypothyroidism, hypopituitarism, hypogonadism, Cushing syndrome |
| Nutritional | Rapid weight loss, TPN, starvation, bariatric surgery complications |
| Metabolic disorders | Lipodystrophy, abetalipoproteinemia, glycogen storage disease |
| Other | Obstructive sleep apnea, Wilson disease (can mimic NASH) |
3. CLINICAL FEATURES / TRIADS
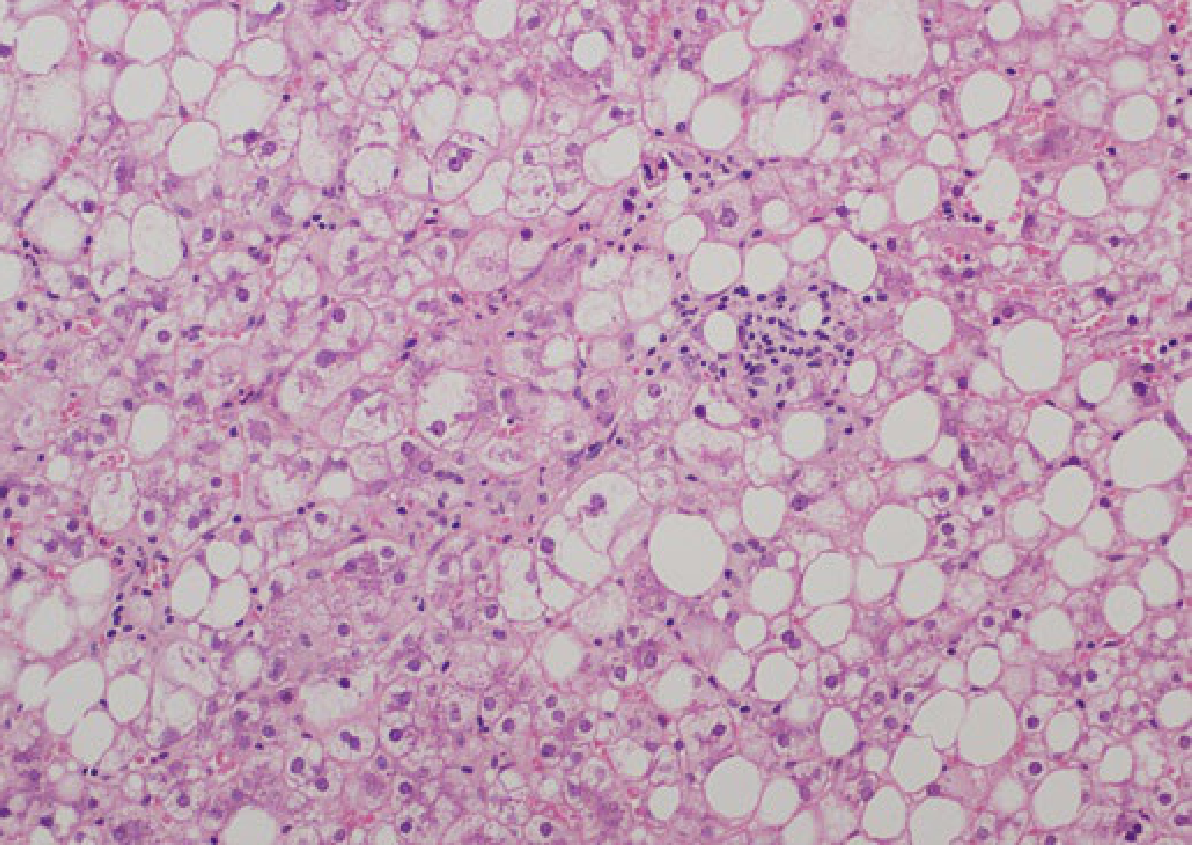
The Diagnostic Histological Triad of NASH
Triad = Macrovesicular Steatosis + Hepatocyte Ballooning + Lobular Inflammation
| Triad Component | Histological Features | Significance |
|---|---|---|
| 1. Macrovesicular Steatosis | Large fat vacuoles pushing nucleus to periphery; >5% hepatocytes; predominant in zone 3 (centrilobular) | Obligatory for diagnosis |
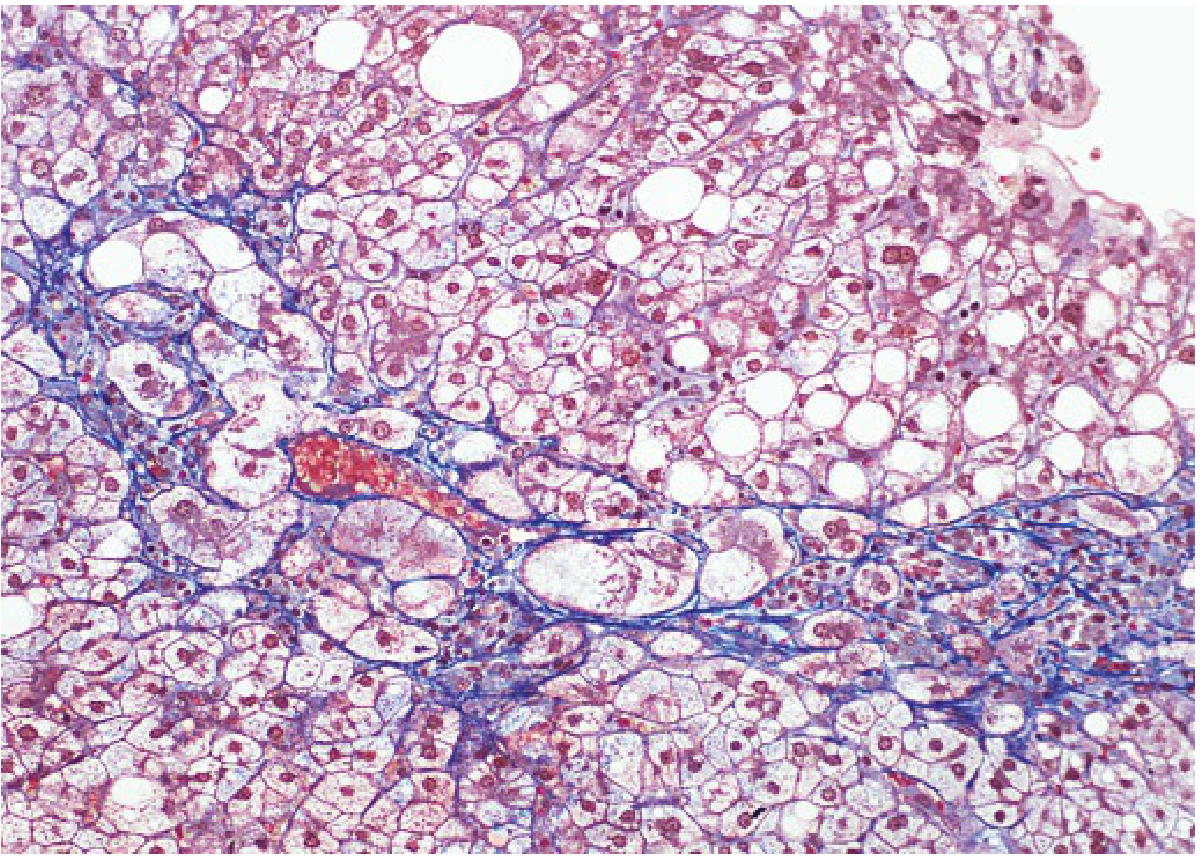
| 2. Hepatocyte Ballooning | Swollen, pale, rounded hepatocytes with rarefied cytoplasm; loss of cytoskeletal keratin 8/18; Mallory-Denk bodies (MDBs) present | Key distinguishing feature from simple steatosis; correlates with fibrosis |
| 3. Lobular Inflammation | Mixed inflammatory infiltrate: lymphocytes, neutrophils (in perivenular area); ± microgranulomas | Reflects active hepatocyte injury |
| + Fibrosis | Perisinusoidal / pericellular fibrosis (zone 3, "chicken-wire" pattern) → portal fibrosis → bridging → cirrhosis | Most important determinant of clinical outcomes |
- Mallory-Denk bodies (hyaline inclusions) - more prominent in ASH than NASH
- Megamitochondria
- Glycogenated nuclei (especially in pediatric NASH)
- Microvesicular steatosis (less common)
Clinical Symptoms and Signs by Stage
| Feature | NASH (Early) | NASH (Advanced/Cirrhosis) |
|---|---|---|
| Symptoms | Often asymptomatic (majority); fatigue, malaise | Fatigue, weakness, muscle wasting |
| RUQ pain | Vague right upper quadrant discomfort | Persistent RUQ pain |
| Hepatomegaly | Present (smooth, non-tender) | Present ± nodular |
| Jaundice | Absent | Present (late/decompensation) |
| Palmar erythema | May be present | Present |
| Spider nevi | Absent to rare | Present |
| Ascites | Absent | Present (portal hypertension) |
| Encephalopathy | Absent | Present (decompensation) |
| Collateral vessels | Absent | Present (caput medusae) |
| Thrombocytopenia | Normal | Low platelets (hypersplenism) |
| Obesity signs | BMI >25-30, central adiposity | Usually present |
| Acanthosis nigricans | May be present (insulin resistance) | May be present |
Laboratory Features
| Investigation | Finding in NASH |
|---|---|
| ALT | Elevated (ALT > AST; unlike alcoholic hepatitis) - rarely >250 IU/L |
| AST:ALT ratio | <1 (ratio >2 suggests alcoholic hepatitis) |
| GGT | Often mildly elevated |
| ALP | Mildly elevated |
| Serum ferritin | Mild hyperferritinemia (not diagnostic of hemochromatosis) |
| Fasting glucose / HbA1c | Often elevated (insulin resistance / T2DM) |
| Lipid profile | Dyslipidemia: ↑ triglycerides, ↓ HDL |
| ANA / ASMA | Low-grade positivity (not diagnostic of AIH) |
| Hyaluronic acid | Elevated (component of ELF panel - fibrosis biomarker) |
| Platelets | Low in cirrhosis/hypersplenism |
| INR / Albumin | Abnormal in decompensated disease |
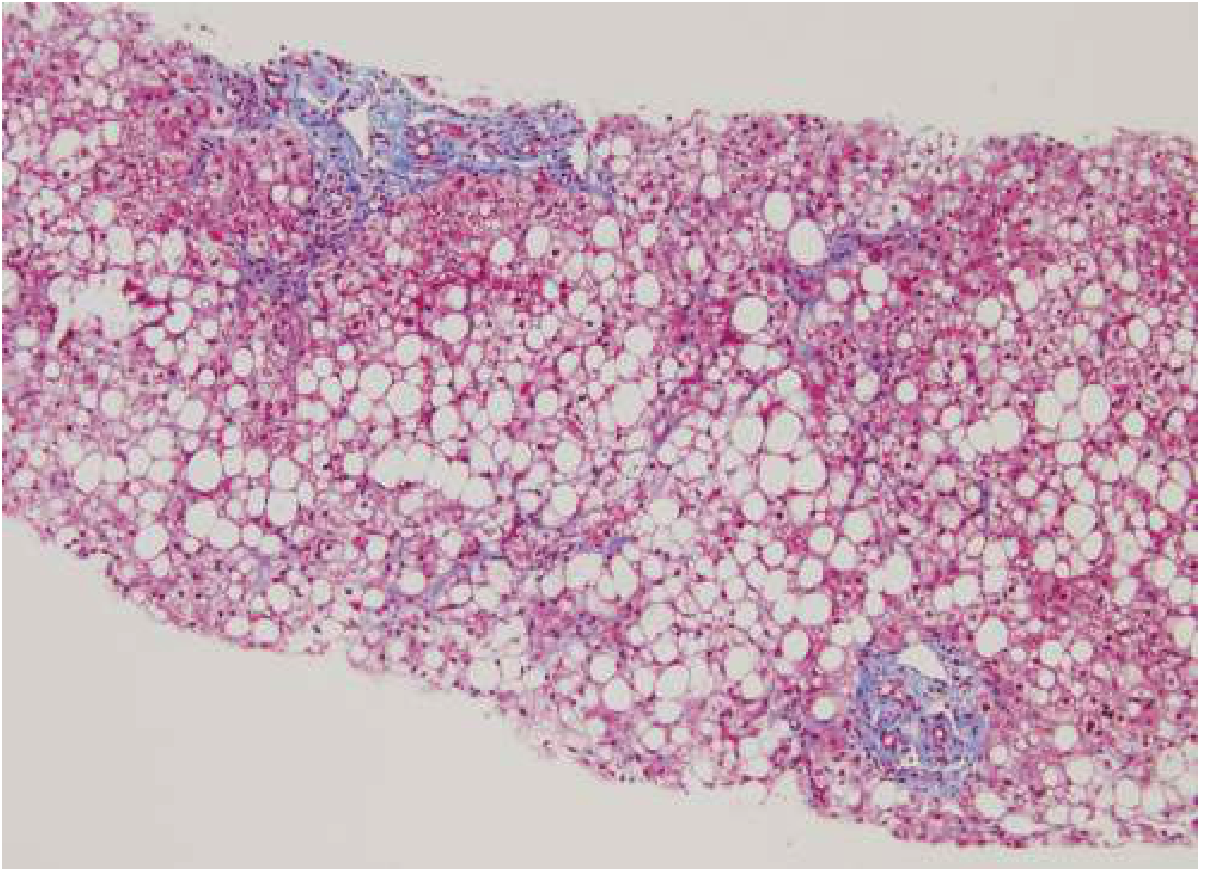
4. HISTOPATHOLOGY IMAGES
5. DIAGNOSIS
Gold Standard Investigation
Percutaneous Liver Biopsy - the only test that can definitively confirm NASH, grade activity, and stage fibrosis.
NAFLD Activity Score (NAS) - Brunt/NASH-CRN Scoring System
| Component | Score | Detail |
|---|---|---|
| Steatosis | 0-3 | 0=<5%, 1=5-33%, 2=34-66%, 3=>66% |
| Lobular Inflammation | 0-3 | 0=none, 1=<2 foci/200×, 2=2-4 foci/200×, 3=>4 foci/200× |
| Hepatocyte Ballooning | 0-2 | 0=none, 1=few, 2=many/prominent |
| Total NAS | 0-8 | NAS ≥5 = NASH; NAS <3 = not NASH |
Fibrosis Staging (NASH-CRN)
| Stage | Description |
|---|---|
| F0 | No fibrosis |
| F1a | Mild perisinusoidal (zone 3) |
| F1b | Moderate perisinusoidal (zone 3) |
| F1c | Portal/periportal only |
| F2 | Perisinusoidal AND portal/periportal |
| F3 | Bridging fibrosis |
| F4 | Cirrhosis |
Diagnostic Algorithm
| Step | Tool | Result / Interpretation |
|---|---|---|
| 1. Exclude competing diagnoses | History + serology (HBsAg, anti-HCV, ANA, ceruloplasmin in <45 yrs) | Negative / normal |
| 2. Metabolic risk assessment | BMI, waist circumference, FBG, HbA1c, lipid profile, BP | Identifies metabolic syndrome |
| 3. Liver enzymes | ALT, AST, GGT, ALP | ALT>AST; rarely >250 IU/L |
| 4. Imaging (First-line) | Abdominal Ultrasound | Bright/echogenic liver = steatosis (PPV ~77%) |
| 5. Non-invasive fibrosis (Step 1) | FIB-4 Index [Age × AST / (Platelets × √ALT)] | FIB-4 <1.3 = low risk; ≥2.67 = high risk |
| 6. Non-invasive fibrosis (Step 2) | FibroScan (VCTE) or MR Elastography | LSM <8 kPa = no advanced fibrosis; >12 kPa = likely advanced fibrosis |
| 7. ELF Panel | Hyaluronic acid + TIMP-1 + N-terminal procollagen III | ELF ≥9.8 = significant fibrosis (FDA approved) |
| 8. Advanced imaging | MRI / MR Spectroscopy (MRS) | Most accurate non-invasive for fat quantification |
| 9. GOLD STANDARD | Percutaneous Liver Biopsy | Confirms NASH, grades NAS, stages fibrosis |
- Persistently elevated transaminases
- Suspicion of NASH with advanced fibrosis
- Unable to exclude competing diagnosis
- Before initiating specific pharmacotherapy
- Assessment of treatment response in trials
6. MANAGEMENT
A. NON-PHARMACOLOGICAL MANAGEMENT
1. Weight Loss and Caloric Restriction
| Intervention | Target | Evidence |
|---|---|---|
| Caloric restriction | Deficit of 500-750 kcal/day | Most effective approach for histological improvement |
| Weight loss 5% | Improves hepatic steatosis and NAS | Meta-analysis of 8 RCTs: ≥5% weight loss improves steatosis; ≥7% improves NAS |
| Weight loss 7-10% | Improves all features of NASH | Large prospective trial (n=261): all NASH features improved with ≥10% weight loss |
| Weight loss >10% | Fibrosis improvement / resolution | Greatest anti-fibrotic benefit |
2. Dietary Modification
| Dietary Measure | Effect | Comment |
|---|---|---|
| Mediterranean diet | Reduces hepatic steatosis | Best-studied specific diet for NASH; high in monounsaturated fats, fiber, omega-3 |
| Low refined carbohydrate / low-fructose diet | Reduces de novo lipogenesis | Eliminate high-fructose corn syrup and sugary drinks |
| Reduce saturated fats (SFAs) | ↓ Hepatic fat and inflammation | Replace with unsaturated fats |
| Omega-3 PUFA supplementation | Reduces hepatic steatosis and triglycerides | Limited histologic benefit alone |
| Coffee consumption 2-3 cups/day | Associated with decreased risk of fibrosis | Mechanism: anti-inflammatory and antifibrotic effects of chlorogenic acid |
| Complete alcohol abstinence | Prevents additive hepatotoxicity | Even moderate drinking worsens outcomes |
3. Physical Activity / Exercise
| Type | Prescription | Effect |
|---|---|---|
| Aerobic exercise | 3-4 times/week; goal 400 kcal expended per session | ↓ Hepatic fat, ↑ insulin sensitivity |
| Resistance training | 2-3 times/week | Independent benefit on insulin resistance and hepatic steatosis |
| Combined aerobic + resistance | Most effective combination | Best when paired with dietary modification |
| Target | 150-200 min/week moderate-intensity activity | Benefits observed even without significant weight loss |
4. Behavioral and Multidisciplinary Approach
| Component | Detail |
|---|---|
| Behavioral therapy / CBT | Addresses eating behaviors, sedentary habits |
| Dietitian | Structured nutritional counseling superior to prescriptive advice alone |
| Exercise physiologist | Supervised exercise program; improves adherence |
| Psychologist | Addresses depression, stress eating (common comorbidities) |
| Regular monitoring | BMI, LFTs, FIB-4 every 1-2 years; FibroScan as appropriate |
5. Bariatric / Metabolic Surgery
| Procedure | Indication | Outcome |
|---|---|---|
| Roux-en-Y Gastric Bypass (RYGB) | BMI ≥40, or ≥35 with metabolic comorbidities, failed lifestyle modification | Resolves/improves NASH in 60-80% of cases; improves fibrosis |
| Sleeve gastrectomy | Same as above | Comparable NASH resolution |
| Laparoscopic adjustable gastric band (LAGB) | Same as above | Less dramatic metabolic benefit |
| Duodenal mucosal resurfacing | Emerging endoscopic procedure | Targets proximal duodenal enterohormone signaling; promising early data |
| Pre-requisite | Exclude portal hypertension before surgery | Risk of decompensation if cirrhosis present |
6. Cardiovascular Risk Management
- Treat dyslipidemia - statins are safe in NAFLD/NASH
- Manage hypertension (ACE inhibitors / ARBs preferred - additional hepatoprotective effect)
- Screen and treat T2DM
- Coronary artery disease is the most common cause of death in NAFLD/NASH patients
B. PHARMACOLOGICAL MANAGEMENT (Table Form)
| Drug Name | Drug Class | Dosage | Indication & Notes |
|---|---|---|---|
| Vitamin E (α-tocopherol) | Antioxidant | 800 IU/day orally for ≥2 years | First-line in non-diabetic, non-cirrhotic NASH (AASLD/PIVENS trial). Improves NAS, reduces ballooning and inflammation; minimal fibrosis benefit. Caution: potential ↑ risk of prostate cancer in men |
| Pioglitazone | Thiazolidinedione - PPARγ agonist (Insulin sensitizer) | 30-45 mg/day orally for 18+ months | Effective in NASH with and without T2DM (PIVENS trial: 47% vs 21% NASH resolution). Improves steatosis, ballooning, inflammation, and possible fibrosis. Side effects: weight gain (~4 kg), fluid retention, osteoporosis (postmenopausal women), ↑ risk of HF exacerbation, debated bladder cancer risk |
| Semaglutide | GLP-1 Receptor Agonist (Incretin mimetic) | 0.4 mg/day subcutaneous injection for 72 weeks | 59% NASH resolution vs 17% placebo (Phase 2 RCT, 320 patients). Dose-dependent benefit. Approved for obesity and T2DM. No significant fibrosis improvement in Phase 2, but Phase 3 (NASH fibrosis) ongoing. Well-tolerated; GI side effects (nausea, vomiting) |
| Liraglutide | GLP-1 Receptor Agonist (Incretin mimetic) | 1.8 mg/day subcutaneous injection | Resolves NASH histology; improves steatosis and reduces fibrosis progression vs placebo. Approved for T2DM and obesity. GI side effects common |
| Tirzepatide | Dual GLP-1 / GIP Receptor Agonist | 5-15 mg/week subcutaneous | Significant weight loss (up to 20.9% body weight). Promising data for MASH/NASH; Phase 3 trials underway. FDA approved for T2DM and obesity |
| Resmetirom (Rezdiffra) | Thyroid Hormone Receptor-β (THR-β) Selective Agonist | 80-100 mg orally once daily | First FDA-approved drug specifically for NASH with fibrosis (F2-F3) - approved March 2024. MAESTRO-NASH Phase 3 trial: significant NASH resolution and fibrosis improvement vs placebo. Liver-directed; metabolic benefits on lipids. (PMID: 38697306, 39187533) |
| Obeticholic Acid (OCA) | FXR (Farnesoid X Receptor) agonist | 10-25 mg/day orally | Histological improvement in NASH (REGENERATE trial). Not yet fully FDA-approved for NASH (application under review). Side effects: worsening pruritus, dose-dependent worsening of dyslipidemia (↓ HDL) |
| Lanifibranor | Pan-PPAR agonist (PPARα/γ/δ) | 1200 mg/day orally | Improves all NASH histological features including fibrosis (NATIVE trial Phase 2b). Favorable metabolic profile. Phase 3 trials ongoing |
| Atorvastatin | HMG-CoA reductase inhibitor (Statin) | 20-40 mg/day orally | Treats dyslipidemia; reduces cardiovascular risk (leading cause of death in NAFLD). Safe in NASH/NAFLD. Modest improvement in liver enzyme levels |
| Pentoxifylline | Phosphodiesterase inhibitor / TNF-α antagonist | 400 mg three times daily (1200 mg/day) orally | Anti-inflammatory via TNF-α inhibition. Improves liver enzymes and histology in NASH. Considered in patients intolerant to first-line therapy |
| Omega-3 PUFAs (Fish Oil) | Lipid-modifying agent (n-3 fatty acids) | 2-4 g/day orally | Reduces hepatic steatosis and serum triglycerides. Limited histological benefit for NASH specifically; adjunct for hypertriglyceridemia |
| Empagliflozin / Dapagliflozin | SGLT-2 Inhibitor | 10-25 mg/day orally | Reduces hepatic fat, body weight, and insulin resistance. Growing evidence for NASH benefit; combined cardiorenal-metabolic benefit makes these attractive for NASH-T2DM patients. Phase 3 trials underway |
| Metformin | Biguanide (insulin sensitizer) | 500-2000 mg/day orally | NOT recommended as a specific NASH treatment (TONIC trial: no histological improvement in children). Useful for concurrent T2DM management; meta-analyses suggest it may reduce HCC risk in T2DM |
Drug Summary by Stage/Population
| Patient Profile | Preferred Agent(s) |
|---|---|
| Non-diabetic NASH (biopsy-proven) | Vitamin E 800 IU/day |
| Diabetic NASH | Pioglitazone 30-45 mg/day OR GLP-1RA |
| NASH + Obesity | Semaglutide / Liraglutide / Tirzepatide |
| NASH + Fibrosis F2-F3 | Resmetirom 80-100 mg/day (FDA approved 2024) |
| NASH + Dyslipidemia | Statin (atorvastatin) |
| NASH + T2DM | GLP-1RA or SGLT-2i + pioglitazone |
| NASH refractory/morbidly obese | Bariatric surgery |
7. PROGNOSIS
| Feature | Outcome |
|---|---|
| Simple steatosis (NAFL) | Benign; only 1-4% progress to advanced fibrosis |
| NASH | 25-50% develop progressive fibrosis; 15-25% progress to cirrhosis over 10-15 years |
| 20% of NASH patients | Rapid progressors to advanced fibrosis within 5-7 years |
| NASH cirrhosis | HCC risk 10.9/1000 person-years; leading indication for liver transplant |
| Most common cause of death | Cardiovascular disease (in NAFLD overall); liver-related mortality exceeds CVD in NASH with cirrhosis |
| Fibrosis regression | Possible with weight loss >10%, bariatric surgery, and resmetirom |
Quick Summary Box
| Domain | Key Point |
|---|---|
| Definition | Steatosis + ballooning + lobular inflammation ± fibrosis, without alcohol or other cause |
| Pathogenesis | Multiple hits: insulin resistance → lipotoxicity → oxidative stress → inflammation → fibrosis |
| Histological Triad | Macrovesicular steatosis + Hepatocyte ballooning + Lobular inflammation |
| Gold Standard | Percutaneous Liver Biopsy (NAS ≥5 = NASH) |
| Non-pharm cornerstone | Weight loss ≥7-10% + Mediterranean diet + exercise |
| 1st-line drug (non-diabetic) | Vitamin E 800 IU/day |
| 1st-line drug (diabetic) | Pioglitazone 30-45 mg/day |
| Newest FDA-approved | Resmetirom (Rezdiffra) - March 2024 - for NASH with F2/F3 fibrosis |
| Fibrosis marker | FIB-4 index + FibroScan (VCTE); biopsy for confirmation |
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), pp. 2747-2751
- Goldman-Cecil Medicine International Edition, pp. 1610-1612
- Yamada's Textbook of Gastroenterology, 7th ed., pp. 2053-2060
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, pp. 1647-1648 (Table 87.3)
- Robbins & Kumar Basic Pathology, p. 635
- Washington Manual of Medical Therapeutics
- Suvarna R et al. (Resmetirom systematic review), Sci Rep 2024 (PMID: 39187533)
- Dutta D et al. (Resmetirom meta-analysis), Endocr Pract 2024 (PMID: 38697306)
- AASLD Practice Guidance (Chalasani N et al., Hepatology 2018; Rinella ME et al., Hepatology 2023)
- EASL-EASD-EASO Clinical Practice Guidelines, J Hepatol 2016
definition , etiopathogenesis ( chart form ) , clinical features / triads , diagnosis ( gold standard investigation , MANAGEMENT ( NON PHARMACOLOGICAL ) , PHARMACOLOGICAL (TABLE FORM ) WITH DRUG NAME , DRUG CLASS , ITS DOSAGE OF DIABETES MELLITUS
"diabetes mellitus type 2" AND management
Diabetes Mellitus (DM)
1. DEFINITION
- Insulin secretion (Type 1: absolute deficiency; Type 2: relative deficiency)
- Insulin action (insulin resistance)
- Or both
Classification
| Type | Description |
|---|---|
| Type 1 DM | Autoimmune destruction of pancreatic β-cells → absolute insulin deficiency; typically young onset |
| Type 2 DM | Insulin resistance + progressive β-cell failure; strongly associated with obesity and metabolic syndrome |
| Gestational DM (GDM) | Abnormal OGTT during pregnancy; pathogenesis similar to Type 2; reverts postpartum or persists |
| MODY (Maturity-Onset Diabetes of the Young) | Monogenic defects in β-cell function; autosomal dominant; multiple subtypes |
| Secondary DM | Due to pancreatic disease, endocrinopathies (Cushing's, acromegaly), drugs (steroids), etc. |
Diagnostic Criteria (ADA)
| Test | Diabetes | Prediabetes |
|---|---|---|
| FPG (Fasting Plasma Glucose) | ≥126 mg/dL (7.0 mmol/L) | 100-125 mg/dL |
| 2-hr OGTT (75 g) | ≥200 mg/dL (11.1 mmol/L) | 140-199 mg/dL |
| HbA1c | ≥6.5% (48 mmol/mol) | 5.7-6.4% |
| Random PG + symptoms | ≥200 mg/dL | - |
2. ETIOPATHOGENESIS (Chart Form)
TYPE 1 DIABETES MELLITUS
GENETIC SUSCEPTIBILITY
(HLA-DR3, HLA-DR4, HLA-DQ alleles)
│
▼
ENVIRONMENTAL TRIGGER
(Viral: Enterovirus, Coxsackievirus B;
Dietary antigens; Gut microbiome changes)
│
▼
AUTOIMMUNE ACTIVATION
Anti-GAD antibodies (Anti-Glutamic Acid Decarboxylase)
Anti-Islet Cell Antibodies (ICA)
Anti-IA-2 / Anti-Zinc Transporter 8 (ZnT8)
Anti-Insulin Antibodies (IAA)
│
▼
T-CELL MEDIATED DESTRUCTION OF β-CELLS
(CD4+ & CD8+ T lymphocytes infiltrate islets → "Insulitis")
│
▼
PROGRESSIVE β-CELL LOSS
(~80-90% β-cell destruction before clinical onset)
│
▼
ABSOLUTE INSULIN DEFICIENCY
│
┌─────┴──────┐
▼ ▼
↑ Glucagon No glucose uptake
↑ Hepatic by peripheral tissues
glucose (muscle, adipose)
output
│ │
└─────┬──────┘
▼
HYPERGLYCEMIA
Glycosuria → Osmotic diuresis
Polyuria → Polydipsia
│
▼ (if no insulin)
DIABETIC KETOACIDOSIS (DKA)
(Unregulated lipolysis → FFA → Ketogenesis)
TYPE 2 DIABETES MELLITUS - "Ominous Octet" (DeFronzo)
════════════════════════════════════════════
GENETIC + ENVIRONMENTAL RISK FACTORS
Obesity, sedentary lifestyle, family history
High-fat/high-carb diet, aging, ethnicity
════════════════════════════════════════════
│
▼
┌───────────────────────┐
│ INSULIN RESISTANCE │
│ (Muscle, Liver, Fat) │
└───────────────────────┘
│
┌──────────┴──────────┐
▼ ▼
β-cell COMPENSATION Adipose tissue
(Hyperinsulinemia) ↑ Lipolysis → ↑ FFA
│
│ (over time)
▼
β-cell EXHAUSTION + GLUCOTOXICITY + LIPOTOXICITY
│
▼
RELATIVE INSULIN DEFICIENCY
════════════════════════════════════════════
TARGET ORGAN PATHOPHYSIOLOGICAL DEFECTS
(The "Ominous Octet" / DeFronzo model)
════════════════════════════════════════════
┌────────────────────────────────────────────────────────────┐
│ 1. Pancreatic β-cells │ ↓ Insulin secretion (1st phase loss)│
│ 2. Pancreatic α-cells │ ↑ Glucagon → ↑ hepatic glucose │
│ 3. Liver │ ↑ Gluconeogenesis, ↑ glycogenolysis │
│ 4. Muscle (Myocytes) │ ↓ GLUT4, ↓ glucose uptake │
│ 5. Adipose tissue │ ↑ Lipolysis → ↑ FFA → ↑ IR │
│ 6. Gut (Incretins) │ ↓ GLP-1 / GIP secretion │
│ 7. Kidney │ ↑ SGLT2 → ↑ glucose reabsorption │
│ 8. Brain │ ↑ Appetite, ↑ oxidative stress │
└────────────────────────────────────────────────────────────┘
│
▼
CHRONIC HYPERGLYCEMIA
│
┌───────────────┼───────────────┐
▼ ▼ ▼
Non-enzymatic Polyol pathway Protein
glycation of activation kinase C
proteins (Sorbitol ↑) activation
│ │ │
└───────────────┴───────────────┘
│
▼
MICROVASCULAR COMPLICATIONS
Retinopathy, Nephropathy, Neuropathy
MACROVASCULAR COMPLICATIONS
CAD, Stroke, Peripheral Vascular Disease
Mechanisms of Hyperglycemic Tissue Damage
| Pathway | Mechanism | Complication |
|---|---|---|
| Non-enzymatic glycation | AGE (Advanced Glycation End-products) formation → cross-linking of proteins | Nephropathy, retinopathy, atherosclerosis |
| Polyol pathway | Excess glucose → sorbitol (via aldose reductase) → osmotic damage | Neuropathy, cataracts, retinopathy |
| Protein Kinase C activation | DAG accumulation → PKC activation → vascular dysfunction | Retinopathy, nephropathy |
| Hexosamine pathway | Excess fructose-6-phosphate → impairs insulin signaling | Insulin resistance, vascular dysfunction |
| Oxidative stress | ↑ ROS → endothelial dysfunction, lipid peroxidation | Atherosclerosis, neuropathy |
3. CLINICAL FEATURES / TRIADS
Classic Triad of Diabetes
"Three Polys" = Polyuria + Polydipsia + Polyphagia
| Classic Symptom | Mechanism |
|---|---|
| Polyuria | Osmotic diuresis from glycosuria (glucose >180 mg/dL exceeds renal threshold) |
| Polydipsia | Dehydration from polyuria → stimulates thirst center |
| Polyphagia | Cellular glucose starvation (glucose can't enter cells) → hunger signals |
Additional Clinical Features
| Feature | Type 1 DM | Type 2 DM |
|---|---|---|
| Age of onset | Usually <30 years (childhood/adolescence) | Usually >40 years (but increasing in youth) |
| Body habitus | Usually lean/normal weight | Usually obese (>80%) |
| Onset | Acute / abrupt | Insidious (often asymptomatic for years) |
| Weight loss | Common (muscle wasting, fat breakdown) | Uncommon initially |
| Fatigue | Present | Present |
| Blurred vision | Present (lens osmotic swelling) | Present |
| Recurrent infections | Furunculosis, candidiasis, UTI | Candidiasis, UTI, wound infections |
| Acanthosis nigricans | Absent | Present (insulin resistance marker) |
| DKA | Common, life-threatening | Rare (HONK more common) |
| HONK / HHS | Rare | Common (in elderly, very high glucose >600 mg/dL) |
| Neuropathy symptoms | Less common early | Burning/tingling feet, numbness |
| Family history | Less strong | Strong (50% concordance in twins) |
| β-cell antibodies | Positive (GAD, ICA, IA-2, ZnT8) | Negative |
| C-peptide | Low / undetectable | Normal or elevated initially |
Chronic Complications (Clinical Features at Presentation)
| System | Complication | Features |
|---|---|---|
| Eye | Diabetic retinopathy | Blurred vision, floaters, visual loss (microaneurysms, neovascularization) |
| Kidney | Diabetic nephropathy | Proteinuria → CKD → ESRD (Kimmelstiel-Wilson nodules on biopsy) |
| Nerve | Peripheral neuropathy | Symmetric stocking-glove sensory loss, burning pain, loss of vibration/proprioception |
| Autonomic | Autonomic neuropathy | Gastroparesis, orthostatic hypotension, ED, bladder dysfunction |
| Heart | Coronary artery disease | Angina, MI (often silent); leading cause of death in T2DM |
| Vessels | Peripheral arterial disease | Claudication, non-healing ulcers, gangrene, Charcot foot |
| Skin | Necrobiosis lipoidica, diabetic dermopathy | Skin changes on legs |
| Foot | Diabetic foot | Neuropathic + ischemic ulcers; risk of amputation |
4. DIAGNOSIS
Gold Standard Investigation
Oral Glucose Tolerance Test (OGTT) with 75g glucose - most sensitive and definitive test, especially for gestational DM and borderline cases. HbA1c is the gold standard for monitoring long-term glycemic control.
Diagnostic Tests Summary
| Test | Method | Diagnostic Cut-off |
|---|---|---|
| Fasting Plasma Glucose (FPG) | Fasting ≥8 hours | ≥126 mg/dL (7.0 mmol/L) |
| 75g OGTT (2-hr PG) | Gold Standard for diagnosis | ≥200 mg/dL (11.1 mmol/L) |
| Random Plasma Glucose | Any time + symptoms | ≥200 mg/dL |
| HbA1c | Reflects 3-month avg glucose | ≥6.5% (48 mmol/mol) |
| C-peptide | Measure of endogenous insulin | Low in T1DM, Normal/High in T2DM |
| Anti-GAD antibodies | Autoimmune T1DM marker | Positive in T1DM |
| Islet Cell Antibodies (ICA) | Autoimmune marker | Positive in T1DM |
| Urine glucose / ketones | Screening | Positive in DKA/DM |
| Microalbuminuria | Nephropathy screening | 30-300 mg/day = early nephropathy |
Monitoring Tests
| Test | Frequency | Target |
|---|---|---|
| HbA1c | Every 3 months (uncontrolled); 6 months (controlled) | <7% (most adults); individualized |
| Self-Monitoring of Blood Glucose (SMBG) | Daily | Pre-meal: 80-130 mg/dL; Post-meal: <180 mg/dL |
| Lipid profile | Annually | LDL <70-100 mg/dL in DM + CVD |
| Urine albumin:creatinine ratio | Annually | <30 mg/g |
| eGFR | Annually | Monitor for nephropathy |
| Fundoscopy | Annually | Screen retinopathy |
| Foot examination | Annually (at minimum) | Monofilament testing |
5. MANAGEMENT
A. NON-PHARMACOLOGICAL MANAGEMENT
1. Medical Nutrition Therapy (Diet)
| Recommendation | Detail |
|---|---|
| Caloric restriction | 1100-1600 kcal/day (deficit 500-750 kcal/day for obese T2DM) |
| Carbohydrate control | 45-60% of total calories; emphasize low glycemic index foods; limit refined sugars and high-fructose corn syrup |
| Protein | 15-20% of calories; reduce to 0.8 g/kg/day if nephropathy |
| Fat | <30% calories; <7% saturated fat; increase monounsaturated fats |
| Fiber | High-fiber diet (>25-30 g/day): vegetables, legumes, whole grains |
| Mediterranean diet | Preferred dietary pattern - reduces HbA1c and CVD risk |
| Alcohol | Limit to 1 drink/day (women), 2 (men); never on empty stomach (hypoglycemia risk) |
| Timing of meals | Regular meal spacing; avoid prolonged fasting; carbohydrate counting for T1DM |
2. Physical Activity / Exercise
| Type | Prescription | Benefit |
|---|---|---|
| Aerobic exercise | 150 min/week moderate intensity (brisk walking, cycling, swimming); 3-5 days/week | ↓ HbA1c by 0.5-0.7%; ↑ insulin sensitivity; ↓ CVD risk |
| Resistance training | 2-3 times/week | ↑ Muscle glucose uptake; ↑ insulin sensitivity |
| Combined training | Most effective combination | Greater glycemic benefit than either alone |
| Caution | Check glucose pre-exercise; avoid if BG <100 or >300 mg/dL; carry fast-acting carbohydrate |
3. Diabetes Self-Management Education and Support (DSMES)
| Component | Detail |
|---|---|
| SMBG training | Proper glucose monitoring technique and log keeping |
| Insulin technique | Injection sites, rotation, storage, pen use |
| Hypoglycemia recognition | Rule of 15: 15g fast-acting carbs if BG <70 mg/dL; recheck in 15 min |
| Sick-day rules | Continue medications; check glucose/ketones more frequently |
| Foot care | Daily inspection, proper footwear, early wound care |
| Eye care / dental care | Annual dilated eye exam; regular dental hygiene |
4. Weight Management
| Intervention | Target | Outcome |
|---|---|---|
| Caloric restriction + exercise | 5-10% body weight loss | Significant HbA1c reduction; may achieve remission of T2DM |
| Intensive lifestyle program | >10% weight loss | HbA1c can normalize without medication |
| Bariatric surgery | BMI >35 with T2DM (or >30 with uncontrolled DM) | 60-80% T2DM remission; Roux-en-Y most effective |
5. Cardiovascular Risk Factor Management
| Factor | Target |
|---|---|
| Blood pressure | <130/80 mmHg |
| LDL cholesterol | <70 mg/dL (with CVD); <100 mg/dL (without) |
| Smoking cessation | Mandatory |
| Aspirin | 75-100 mg/day in DM with established CVD |
6. Monitoring and Screening
- Annual: HbA1c, lipids, urine albumin, eGFR, fundoscopy, foot exam
- Vaccinations: influenza, pneumococcal, hepatitis B
- Blood pressure monitoring at every visit
B. PHARMACOLOGICAL MANAGEMENT (Table Form)
ORAL ANTIDIABETIC AGENTS
| Drug Name | Drug Class | Mechanism | Dosage | Key Notes |
|---|---|---|---|---|
| Metformin | Biguanide | ↓ Hepatic gluconeogenesis; ↑ peripheral insulin sensitivity; ↓ GI glucose absorption | 500 mg OD → titrate to 1000 mg BD (max 2550 mg/day; optimal effect at 2000 mg/day) | First-line for T2DM (unless contraindicated). Weight neutral; ↓ CVD. CI: eGFR <30, liver failure, iodinated contrast (hold day of) |
| Glibenclamide (Glyburide) | Sulfonylurea (2nd gen) | Closes K-ATP channels on β-cell → ↑ insulin secretion | 2.5-5 mg OD (start); maintenance 5-10 mg OD; max 20 mg/day | Risk of hypoglycemia; weight gain. Avoid in elderly, renal failure, liver failure |
| Glipizide | Sulfonylurea (2nd gen) | Same as above | 5 mg OD (start); max 40 mg/day (>15 mg/day split doses); XL form: 5-20 mg OD | Take 30 min before meals. Preferred in elderly (short half-life, inactive metabolites) |
| Glimepiride | Sulfonylurea (2nd gen) | Same as above | 1-2 mg OD (start); max 8 mg OD | Lowest dose of all SUs; once daily; hepatic metabolism |
| Gliclazide | Sulfonylurea (2nd gen) | Same as above | 40-80 mg OD (start); max 320 mg/day (split if >160 mg) | Not available in USA; inactive metabolites; safer in elderly |
| Pioglitazone | Thiazolidinedione (TZD) - PPARγ agonist | ↑ Peripheral insulin sensitivity (muscle and fat); ↓ hepatic glucose output | 15-30 mg OD (start); max 45 mg OD | Cardiovascular benefit; weight gain ~4 kg; fluid retention; avoid in HF (NYHA III/IV); possible bladder cancer risk |
| Sitagliptin | DPP-4 Inhibitor (Gliptin) | Inhibits DPP-4 → ↑ GLP-1 and GIP → glucose-dependent ↑ insulin + ↓ glucagon | 100 mg OD (reduce to 50 mg if eGFR 30-49; 25 mg if eGFR <30) | Weight neutral; low hypoglycemia risk; nasopharyngitis; rare pancreatitis |
| Saxagliptin | DPP-4 Inhibitor | Same as above | 2.5-5 mg OD | Caution in HF (↑ risk of HF hospitalization) |
| Vildagliptin | DPP-4 Inhibitor | Same as above | 50 mg OD or BD | Quarterly LFTs in first year; hepatic monitoring |
| Linagliptin | DPP-4 Inhibitor | Same as above | 5 mg OD | Only DPP-4i primarily excreted via bile - no dose adjustment in renal failure |
| Alogliptin | DPP-4 Inhibitor | Same as above | 25 mg OD (12.5 mg if CrCl 30-60; 6.25 mg if <30) | Possible ↑ LFTs; caution in liver disease |
| Empagliflozin | SGLT-2 Inhibitor (Gliflozin) | Inhibits SGLT2 in proximal tubule → glycosuria → ↓ glucose, ↓ weight, ↓ BP | 10 mg OD (can increase to 25 mg OD) | CV and renal benefit (EMPA-REG OUTCOME trial). ↓ HF hospitalization, ↓ CKD progression. Risk: genital mycosis, UTI, DKA, Fournier's gangrene |
| Dapagliflozin | SGLT-2 Inhibitor | Same as above | 5-10 mg OD (5 mg initial in hepatic failure) | Also approved for HFrEF and CKD independent of T2DM; CI if eGFR <30 |
| Canagliflozin | SGLT-2 Inhibitor | Same as above | 100 mg OD (increase to 300 mg OD if eGFR normal) | ↑ Risk of lower limb amputation and fractures (CANVAS trial); CI if eGFR <30 |
| Ertugliflozin | SGLT-2 Inhibitor | Same as above | 5 mg OD (increase to 15 mg OD) | CI if eGFR <30 |
| Acarbose | Alpha-glucosidase inhibitor | Delays intestinal absorption of carbohydrates → ↓ post-meal glucose | 25 mg TDS (with meals); max 100 mg TDS | No hypoglycemia; GI side effects (bloating, flatulence, diarrhea); treat hypoglycemia with glucose (not sucrose) |
| Repaglinide | Meglitinide (non-SU secretagogue) | Closes K-ATP channels on β-cell → rapid ↑ insulin (shorter-acting than SUs) | 0.5-2 mg before each meal (TDS); max 16 mg/day | Take only if eating; flexible dosing; risk of hypoglycemia; useful if irregular meal patterns |
| Nateglinide | Meglitinide | Same as above | 60-120 mg before each main meal (TDS) | Short-acting; mainly reduces post-meal hyperglycemia |
INJECTABLE NON-INSULIN AGENTS
| Drug Name | Drug Class | Mechanism | Dosage | Key Notes |
|---|---|---|---|---|
| Liraglutide | GLP-1 Receptor Agonist | Mimics GLP-1: glucose-dependent ↑ insulin, ↓ glucagon, ↓ gastric emptying, ↑ satiety → weight loss | 0.6 mg SC OD (initial); titrate to 1.2-1.8 mg SC OD | CV benefit (LEADER trial); weight loss ~3 kg; also approved for obesity (Saxenda: 3 mg). GI side effects; rare pancreatitis; not for T1DM (except specific indications) |
| Semaglutide | GLP-1 Receptor Agonist | Same as above | SC: 0.25 mg SC weekly → 0.5-1 mg weekly; Oral: 3-14 mg OD | Once-weekly SC or daily oral (Rybelsus). CV and weight loss benefit (SUSTAIN, PIONEER trials). Most potent GLP-1RA for weight loss |
| Exenatide | GLP-1 Receptor Agonist | Same as above | 5 mcg SC BD → 10 mcg SC BD after 1 month; XR: 2 mg SC weekly | First approved GLP-1RA; twice-daily or once-weekly (Bydureon) |
| Dulaglutide | GLP-1 Receptor Agonist | Same as above | 0.75-1.5 mg SC weekly | Once weekly; CV benefit (REWIND trial) |
| Tirzepatide | Dual GIP / GLP-1 Receptor Agonist | Activates both GIP and GLP-1 receptors → superior weight loss and glycemic control | 2.5 mg SC weekly → titrate to 5-15 mg SC weekly | Newest; most potent for weight loss (up to ~20%); approved for T2DM (Mounjaro) and obesity (Zepbound) |
| Pramlintide | Amylin analogue | ↓ Post-meal glucagon; slows gastric emptying; ↑ satiety | T1DM: 15-60 mcg SC before meals; T2DM: 60-120 mcg SC before meals | Adjunct to insulin; reduces post-meal glucose; nausea common |
INSULIN PREPARATIONS (Table Form)
| Insulin Type | Drug Name (Examples) | Onset | Peak | Duration | Dosage / Regimen |
|---|---|---|---|---|---|
| Rapid-acting analogs | Insulin Lispro (Humalog), Insulin Aspart (NovoLog), Insulin Glulisine (Apidra) | 10-15 min | 1-2 hr | 3-5 hr | Given immediately before meals; 1 unit per 10-15g carbohydrate (T1DM); correction factor calculated individually |
| Short-acting (Regular) | Human Regular Insulin (Humulin R, Novolin R) | 30-60 min | 2-4 hr | 5-8 hr | Give 30 min before meals; also used IV in DKA/HHS; U-500 for insulin-resistant patients |
| Intermediate-acting | NPH Insulin (Humulin N, Novolin N) | 1-3 hr | 4-10 hr | 10-18 hr | Given BD; often with short-acting at breakfast and bedtime |
| Long-acting basal | Insulin Glargine (Lantus U-100; Toujeo U-300), Insulin Detemir (Levemir), Insulin Degludec (Tresiba U-100/U-200) | 1-2 hr | Peakless | 20-24+ hr | Once daily (Glargine/Degludec) or BD (Detemir); T1DM basal needs: 0.25-0.4 U/kg/day |
| Premixed | 70/30 NPH/Regular, 75/25 NPL/Lispro, 70/30 NPA/Aspart | Biphasic | Biphasic | ~18-24 hr | Given BD before breakfast and dinner; convenient but less flexible |
- Start basal insulin (glargine/detemir) at 10 units OD or 0.1-0.2 U/kg/day
- Titrate by 2 units every 3 days until fasting BG 80-130 mg/dL
- If HbA1c still >7% despite basal optimization → add prandial (bolus) insulin
Step-Wise Pharmacological Algorithm for Type 2 DM
STEP 1: Lifestyle modification + Metformin
(unless eGFR <30 or intolerant)
│
▼ (if HbA1c target not met)
STEP 2: Add 2nd agent based on patient profile:
┌────────────────────────────────────────────────────────┐
│ CVD / HF / CKD present → SGLT-2i or GLP-1RA first │
│ Obesity → GLP-1RA or SGLT-2i │
│ Cost concern → Sulfonylurea or TZD │
│ Hypoglycemia risk → DPP-4i, GLP-1RA, SGLT-2i │
└────────────────────────────────────────────────────────┘
│
▼ (if still not at target)
STEP 3: Triple combination therapy
│
▼
STEP 4: Add basal insulin (Glargine / Degludec)
│
▼
STEP 5: Intensify to basal-bolus insulin regimen
Glycemic Targets Summary (ADA 2024)
| Target | Value |
|---|---|
| HbA1c | <7.0% (most non-pregnant adults) |
| Pre-meal glucose | 80-130 mg/dL |
| 2-hr post-meal glucose | <180 mg/dL |
| Bedtime glucose | 100-140 mg/dL |
| BP | <130/80 mmHg |
| LDL | <70 mg/dL (with CVD); <100 mg/dL (without) |
Quick Summary Box
| Domain | Key Point |
|---|---|
| Definition | Chronic hyperglycemia from insulin deficiency and/or resistance |
| Classic Triad | Polyuria + Polydipsia + Polyphagia |
| Gold Standard Dx | 75g OGTT (2-hr PG ≥200 mg/dL); HbA1c for monitoring |
| T1DM pathogenesis | Autoimmune β-cell destruction (HLA-DR3/DR4 associated) |
| T2DM pathogenesis | Insulin resistance + β-cell failure; Ominous Octet of defects |
| Non-pharm cornerstone | Diet (Mediterranean), exercise (150 min/wk), weight loss |
| T2DM first-line drug | Metformin 500-2000 mg/day |
| Best CV + renal protection | SGLT-2 inhibitors (empagliflozin/dapagliflozin) + GLP-1RA |
| T1DM treatment | Basal-bolus insulin regimen (mandatory) |
| Monitoring gold standard | HbA1c every 3-6 months; target <7% |
| Most common cause of death | Cardiovascular disease (CAD, MI) |
- Katzung's Basic and Clinical Pharmacology, 16th Edition (DM pharmacology, insulin tables, drug dosages)
- Textbook of Family Medicine, 9th Edition (Pathogenesis - Ominous Octet, Table 34-6)
- Goldman-Cecil Medicine International Edition (Glycemic control, SGLT-2 algorithm)
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
- Goodman & Gilman's Pharmacological Basis of Therapeutics (Metformin, SGLT-2, GLP-1)
- AACE Consensus Statement: Algorithm for Management of Adults With Type 2 Diabetes - 2026 Update (PMID: 41842862)
- ADA Standards of Medical Care in Diabetes 2024
definition , etiopathogenesis ( chart form ) , clinical features / triads , diagnosis ( gold standard investigation , MANAGEMENT ( NON PHARMACOLOGICAL ) , PHARMACOLOGICAL (TABLE FORM ) WITH DRUG NAME , DRUG CLASS , ITS DOSAGE OF GENERAL ANXIETY DISORDER ( IN A VERY SIMPLIFIED LANGUAGE )
"generalized anxiety disorder" AND treatment
Generalized Anxiety Disorder (GAD)
Written in simple, easy-to-understand language as requested.
1. DEFINITION - "What is GAD?"
- Hard to control or stop
- Out of proportion to the actual problem
- So intense it interferes with daily life (work, relationships, sleep)
"Patients with GAD worry about them to the point where catastrophe seems possible, likely, and imminent. They cannot prioritize or put worries aside." - Kaplan & Sadock's Synopsis of Psychiatry
- Lifetime prevalence: 5-6% of the population
- Onset: Usually before age 20
- More common in women (2:1)
- Over 80% of patients also have depression, dysthymia, or social phobia
2. ETIOPATHOGENESIS (Chart Form)
What causes GAD? (Simple Version)
══════════════════════════════════════════════
WHY DOES GAD HAPPEN?
══════════════════════════════════════════════
BIOLOGICAL FACTORS
┌─────────────────────┐
│ 1. Brain Chemistry │
│ Problems │
└────────┬────────────┘
│
┌─────────────┼──────────────┐
▼ ▼ ▼
GABA SEROTONIN NOREPINEPHRINE
Too little Too little Too much
(brain's (mood (stress
"calm" regulator) hormone)
chemical)
│ │ │
└─────────────┴──────────────┘
│
▼
BRAIN BECOMES TOO
"SWITCHED ON" FOR DANGER
(Overactive: Amygdala, HPA axis)
══════════════════════════════════════════════
PSYCHOLOGICAL FACTORS
══════════════════════════════════════════════
Past trauma or bad experiences
Learned worry patterns from childhood
Perfectionism / High need for control
Low tolerance for uncertainty
Negative thinking style ("What if?")
══════════════════════════════════════════════
GENETIC FACTORS
══════════════════════════════════════════════
Family history of anxiety / depression
First-degree relatives at higher risk
Genes affecting serotonin transporters
(Heritability ~30%)
══════════════════════════════════════════════
ENVIRONMENTAL / SOCIAL FACTORS
══════════════════════════════════════════════
Stressful life events (job loss, divorce)
Childhood adversity or abuse
Chronic illness / pain
Substance abuse (alcohol, caffeine, drugs)
══════════════════════════════════════════════
ALL THREE COMBINE
│
▼
══════════════════════════════════════════════
BRAIN STUCK IN "WORRY MODE"
GABA system can't calm things down
Amygdala fires "danger signals" constantly
Prefrontal cortex (rational thinking) overwhelmed
│
▼
GENERALIZED ANXIETY DISORDER (GAD)
══════════════════════════════════════════════
Brain Chemistry Summary (Simple)
| Brain Chemical | Normal Role | In GAD |
|---|---|---|
| GABA | Brain's "calm down" signal | Too little → brain stays anxious |
| Serotonin (5-HT) | Mood stabilizer, happiness | Too little → low mood + anxiety |
| Norepinephrine | "Fight or flight" response | Too much → always feels alert/tense |
| CRF / Cortisol | Stress hormone | Chronically elevated → always "stressed" |
3. CLINICAL FEATURES / TRIADS
The GAD Triad (Core 3 Features)
Excessive Worry + Physical Tension + Inability to Control the Worry
DSM-5 Diagnostic Criteria (Simplified)
| # | Symptom | What it Feels Like (Simple) |
|---|---|---|
| 1 | Restlessness / Feeling "on edge" | Can't sit still; always feels wired or keyed up |
| 2 | Easy fatigue | Tired all the time even without doing much |
| 3 | Difficulty concentrating / "Mind going blank" | Can't focus; mind wanders or freezes |
| 4 | Irritability | Gets frustrated easily over small things |
| 5 | Muscle tension | Tight neck, shoulders, jaw; headaches |
| 6 | Sleep problems | Trouble falling asleep or staying asleep due to worrying |
Physical Symptoms of GAD
| System | Symptom |
|---|---|
| Muscles | Tension headaches, neck/back stiffness, trembling |
| Heart | Mild palpitations (unlike panic disorder - no major racing heart) |
| Gut | Nausea, irritable bowel, stomach discomfort |
| Breathing | Slight tightness in chest (mild) |
| Sleep | Insomnia, unrefreshing sleep, nightmares |
| Nerves | Sweating, shakiness, dry mouth |
Important: In GAD, complaints of shortness of breath and palpitations are less prominent than in panic disorder.
GAD vs Normal Worry - Simple Comparison
| Normal Worry | GAD Worry |
|---|---|
| About real problems | About everything, even small things |
| Comes and goes | Almost every day, for 6+ months |
| Can be set aside | Hard or impossible to stop |
| Doesn't affect daily life | Interferes with work, relationships, sleep |
| Proportionate | Out of proportion to actual risk |
4. DIAGNOSIS
Gold Standard Investigation
Clinical Interview using DSM-5 Criteria - there is no blood test or scan for GAD. Diagnosis is made by a trained doctor/psychiatrist through careful questioning.
Diagnostic Tools (Simple)
| Tool | What It Does |
|---|---|
| DSM-5 Clinical Interview | Gold Standard - psychiatrist/doctor checks if patient meets all criteria |
| GAD-7 Scale | 7-question questionnaire; scores anxiety severity (0-21; ≥10 = moderate-severe GAD) |
| Beck Anxiety Inventory (BAI) | Measures anxiety symptoms; helps monitor treatment |
| Hamilton Anxiety Rating Scale (HAM-A) | Rates 14 anxiety items; used in research and clinics |
| Hospital Anxiety & Depression Scale (HADS) | Screens for both anxiety AND depression together |
GAD-7 Scoring (Quick Guide)
| GAD-7 Score | Severity |
|---|---|
| 0-4 | Minimal anxiety |
| 5-9 | Mild anxiety |
| 10-14 | Moderate anxiety |
| 15-21 | Severe anxiety |
Ruling Out Other Causes First
| Must Exclude | How |
|---|---|
| Hyperthyroidism | Thyroid function tests (TFTs) |
| Cardiac arrhythmia | ECG |
| Substance use (caffeine, alcohol, stimulants) | History + urine drug screen |
| Panic disorder | Assess for episodic, sudden attacks |
| Depression | PHQ-9 or clinical interview |
| Medical illness (COPD, cardiac disease) | Full physical exam + investigations |
5. MANAGEMENT
A. NON-PHARMACOLOGICAL MANAGEMENT
Think of non-drug treatment as "retraining the brain" to stop the worry spiral.
1. Psychotherapy (Talking Therapies)
| Therapy | What it Does (Simple Explanation) | Evidence |
|---|---|---|
| Cognitive Behavioral Therapy (CBT) | Best psychological treatment for GAD. Teaches patient to identify and challenge negative "what if?" thoughts; replaces worry with realistic thinking; breaks the worry cycle | Strongest evidence; as effective as medication in many patients |
| Relaxation Training | Deep breathing, progressive muscle relaxation (tensing and releasing muscles) to reduce physical tension | Effective especially for muscle symptoms; good for long-term practice |
| Mindfulness-Based Therapy (MBSR) | Teaches patient to notice worry thoughts without reacting to them; "observing without judging" | Growing evidence; helpful combined with CBT |
| Acceptance and Commitment Therapy (ACT) | Helps patient accept uncertainty instead of fighting it; focuses on living life despite anxiety | Good alternative to CBT |
| Worry Time Technique | Set aside 20-30 min/day specifically for worrying; outside this time, postpone worries | Simple technique; reduces constant background worry |
| Short-Term Dynamic Psychotherapy (STDP) | Explores past emotional conflicts linked to anxiety; equally effective to CBT in some studies | Good for patients with insight |
2. Lifestyle Modifications
| Change | Why It Helps |
|---|---|
| Regular aerobic exercise (30 min, 5 days/week) | Releases endorphins; reduces cortisol; improves sleep and mood |
| Sleep hygiene | Regular sleep time; no screens before bed; cool dark room; reduces anxiety-insomnia cycle |
| Limit caffeine | Caffeine worsens anxiety, trembling, and palpitations - cut coffee, energy drinks, tea |
| Reduce/stop alcohol | Alcohol temporarily relieves anxiety but worsens it long-term (rebound anxiety); risk of dependence |
| Stress management | Time management, saying "no" to overcommitment, taking breaks |
| Social support | Talking to trusted friends/family; join support groups |
| Yoga / meditation | Reduces muscle tension, lowers cortisol, improves sleep |
| Reduce news/social media | Reduces "anxiety triggers" from constant negative information |
3. Psychoeducation
- Explain to the patient what GAD is - "Your brain's alarm is too sensitive"
- Reassure that GAD is treatable and that their worry is a symptom, not reality
- Teach that anxiety cannot cause physical harm (heart attack, death) - this reduces health anxiety spiral
- Encourage patient participation in treatment decisions
B. PHARMACOLOGICAL MANAGEMENT (Table Form)
FIRST-LINE DRUGS
| Drug Name | Drug Class | How it Works (Simple) | Dosage | Key Notes |
|---|---|---|---|---|
| Escitalopram | SSRI (Selective Serotonin Reuptake Inhibitor) | Increases serotonin ("happiness chemical") in the brain | Start 5 mg OD; increase to 10-20 mg OD | FDA approved for GAD. Very well tolerated. Start at HALF the usual depression dose. Takes 4-6 weeks to work. Side effects: nausea, insomnia initially |
| Paroxetine | SSRI | Same as above | Start 10 mg OD; increase to 20-40 mg OD | FDA approved for GAD. More sedating - useful if sleep problems. More discontinuation symptoms than other SSRIs. Weight gain possible |
| Sertraline | SSRI | Same as above | Start 25 mg OD; increase to 50-200 mg OD | Not FDA approved specifically for GAD but widely used (class effect); very safe; good first choice |
| Venlafaxine XR | SNRI (Serotonin-Norepinephrine Reuptake Inhibitor) | Increases both serotonin AND norepinephrine | Start 37.5 mg OD; increase to 75-225 mg OD | FDA approved for GAD. Good for GAD with depression. Monitor BP (may increase). XR (extended-release) form preferred |
| Duloxetine | SNRI | Same as above | Start 30 mg OD; increase to 60-120 mg OD | FDA approved for GAD. Also helps chronic pain and muscle tension. Good if physical symptoms prominent |
SECOND-LINE DRUGS
| Drug Name | Drug Class | How it Works (Simple) | Dosage | Key Notes |
|---|---|---|---|---|
| Buspirone | Azapirone / 5-HT1A partial agonist | Acts on serotonin receptors; calms worry without causing sedation or addiction | Start 7.5 mg BD; increase to 15-30 mg BD (max 60 mg/day) | FDA approved for GAD. Non-addictive - safe long-term. Slow onset (2-4 weeks). Works best in patients who have never taken benzodiazepines before. No dependence. Good for chronic mild-moderate GAD |
| Hydroxyzine | Antihistamine (H1 blocker) | Blocks histamine receptors → sedation and reduced anxiety | 25-50 mg TDS or QDS (max 400 mg/day); 25-100 mg at bedtime for sleep | FDA approved for GAD. Works quickly (30-60 min). No dependence risk. Useful short-term. Side effects: drowsiness, dry mouth |
| Pregabalin | Alpha-2-delta (α2δ) ligand / Anticonvulsant | Reduces overactive brain signaling (calcium channels) | 75 mg BD; increase to 150-300 mg BD (max 600 mg/day) | Approved for GAD in Europe (not US). Largest effect size of all drugs in meta-analysis. Fast onset (1-2 weeks). Good alternative to benzodiazepines |
| Clonazepam | Benzodiazepine (long-acting) | Enhances GABA ("calm down" signal) - fast anxiety relief | 0.25-0.5 mg BD (start); usual 1-4 mg/day | FDA approved for GAD. Fast-acting; long half-life = stable levels. Use short-term only (2-4 weeks). Risk of dependence; withdrawal if stopped abruptly. Use as bridge while SSRIs kick in |
| Alprazolam XR | Benzodiazepine (extended release) | Same as above | Start 0.5 mg OD; usual 1-4 mg/day | Extended-release form preferred over immediate release for GAD (more steady levels) |
| Lorazepam | Benzodiazepine (short-intermediate) | Same as above | 0.5-1 mg BD-TDS (usual); max 4-6 mg/day | Safer in elderly and liver disease (metabolized by conjugation, no active metabolites); still use short-term only |
| Imipramine | Tricyclic Antidepressant (TCA) | Blocks serotonin + norepinephrine reuptake; also anticholinergic effects | Start 25 mg OD; increase to 150-300 mg/day | Effective (strongest TCA evidence for GAD); relegated to 2nd/3rd line due to side effects (sedation, dry mouth, constipation, heart effects, lethal in overdose) |
AUGMENTATION / ADD-ON OPTIONS (If First-Line Fails)
| Drug Name | Drug Class | Dosage | Notes |
|---|---|---|---|
| Mirtazapine | Noradrenergic & Specific Serotonergic Antidepressant (NaSSA) | 15-45 mg at bedtime | Off-label; useful if sleep problems + anxiety + poor appetite; sedating |
| Quetiapine | Atypical antipsychotic | 50-150 mg at bedtime | Evidence for GAD as monotherapy; FDA denied approval (side effects: weight gain, metabolic effects, sedation); use only in refractory cases |
| Propranolol | Beta-blocker | 10-40 mg BD-TDS (as needed for physical symptoms) | Blocks physical symptoms (shaking, palpitations); does NOT treat underlying worry or emotional anxiety; useful for situational/performance anxiety |
| Gabapentin | α2δ ligand | 300-600 mg TDS | Off-label; similar to pregabalin; useful augmentation agent |
| Vortioxetine | Serotonin modulator | 5-20 mg OD | Off-label but effective in some studies; also improves cognition |
Treatment Timeline (Simple Plan)
WEEK 1-2:
Start SSRI/SNRI at LOW dose (half of depression dose)
+ Benzodiazepine SHORT-TERM (bridge while waiting for SSRI to work)
+ Start CBT (refer to therapist)
│
▼
WEEKS 4-6:
SSRI/SNRI starts working → taper benzodiazepine
Continue CBT (8-20 sessions typical)
│
▼
WEEKS 8-12:
Assess response (use GAD-7)
If partial response → increase SSRI/SNRI dose
Or add buspirone / pregabalin
│
▼
MONTHS 6-12:
Continue treatment (most patients need 12+ months)
Maintain lifestyle changes
│
▼
Consider tapering medication SLOWLY
after sustained remission (≥12 months symptom-free)
Quick Summary
| Topic | Simple Summary |
|---|---|
| What is GAD? | Excessive, uncontrollable worry about many things for 6+ months |
| Core Triad | Excessive worry + Physical tension + Inability to stop worrying |
| Brain cause | Low GABA + Low serotonin = brain stuck in "worry mode" |
| Gold Standard Dx | Clinical interview using DSM-5 criteria + GAD-7 questionnaire |
| Best non-drug treatment | CBT (Cognitive Behavioral Therapy) |
| Best drug (1st line) | SSRI (escitalopram/paroxetine) or SNRI (venlafaxine/duloxetine) |
| Non-addictive alternative | Buspirone (needs 2-4 weeks to work) |
| Quick relief (short-term only) | Benzodiazepines (clonazepam/lorazepam) - bridge therapy only |
| Drug with biggest effect size | Pregabalin (best evidence in meta-analysis) |
| Key lifestyle change | Exercise + cut caffeine + CBT |
| Prognosis | Treatable but often chronic; combination treatment is best |
- Kaplan & Sadock's Synopsis of Psychiatry, 12th Edition, pp. 1252-1253
- Textbook of Family Medicine, 9th Edition, pp. 1325-1327
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), pp. 3701-3702
- Stahl's Essential Psychopharmacology, pp. 393
- Lippincott Illustrated Reviews: Pharmacology, pp. 556-557
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
definition , etiopathogenesis ( chart form ) , clinical features / triads , diagnosis ( gold standard investigation , MANAGEMENT ( NON PHARMACOLOGICAL ) , PHARMACOLOGICAL (TABLE FORM ) WITH DRUG NAME , DRUG CLASS , ITS DOSAGE OF SOMATOFORM AND MOOD DISORDER( IN A VERY SIMPLIFIED LANGUAGE )
"somatic symptom disorder" AND management
PART 1: SOMATOFORM DISORDER
1. DEFINITION - "What is Somatoform Disorder?"
Key point: The patient is NOT lying or pretending. The symptoms are REAL to them. The problem is how the brain processes and amplifies body sensations.
DSM-5 Classification (Updated Names)
| Old Name (DSM-IV) | New Name (DSM-5) | Simple Meaning |
|---|---|---|
| Somatization Disorder | Somatic Symptom Disorder (SSD) | Many unexplained physical symptoms with excessive worry |
| Hypochondriasis | Illness Anxiety Disorder | Excessive fear of having a serious illness |
| Conversion Disorder | Functional Neurological Symptom Disorder | Neurological symptoms (paralysis, blindness) without nerve damage |
| Pain Disorder | Included in SSD | Persistent pain not explained by physical cause |
| Body Dysmorphic Disorder | Moved to OCD Spectrum | Obsessive focus on perceived physical "defects" |
2. ETIOPATHOGENESIS (Chart Form)
══════════════════════════════════════════════
WHY DOES SOMATOFORM DISORDER HAPPEN?
══════════════════════════════════════════════
BIOLOGICAL FACTORS
┌─────────────────────────────────────────┐
│ • Altered brain pain processing │
│ • Overactive stress system (HPA axis) │
│ • ↑ Cortisol + adrenaline chronically │
│ • Brain amplifies normal body signals │
│ (central sensitization) │
│ • Low serotonin + norepinephrine │
└──────────────────┬──────────────────────┘
│
══════════════════════════════════════════════
PSYCHOLOGICAL FACTORS
┌─────────────────────────────────────────┐
│ • History of childhood trauma / abuse │
│ • Learned helplessness from illness │
│ in family │
│ • Cannot express emotions verbally │
│ ("alexithymia") → body speaks instead │
│ • Anxiety/depression expressed as │
│ physical symptoms │
│ • Catastrophic thinking about │
│ body sensations │
└──────────────────┬──────────────────────┘
│
══════════════════════════════════════════════
SOCIAL / CULTURAL FACTORS
┌─────────────────────────────────────────┐
│ • "Sick role" brings attention + care │
│ • Some cultures express distress │
│ physically, not emotionally │
│ • Reinforcement from caregivers │
│ • Secondary gain (avoiding work/duties) │
└──────────────────┬──────────────────────┘
│
▼
══════════════════════════════════════════════
BRAIN MISINTERPRETS NORMAL SIGNALS
↓ Pain threshold
↑ Body awareness / scanning
↑ Focus on physical symptoms
↑ Medical help-seeking
│
▼
SOMATOFORM DISORDER
Real suffering without physical cause
══════════════════════════════════════════════
3. CLINICAL FEATURES / TRIADS
Core Triad of Somatic Symptom Disorder (DSM-5)
1. Physical Symptoms + 2. Excessive Thoughts/Feelings About Them + 3. Abnormal Behavior Because of Them
| Core Feature | Simple Explanation |
|---|---|
| 1. One or more distressing physical symptoms | Pain, fatigue, nausea, shortness of breath, weakness, etc. - real and distressing |
| 2. Excessive worry/thoughts about the symptoms | Constantly thinking the worst; convinced something is seriously wrong |
| 3. Excessive time/energy devoted to symptoms | Repeatedly seeing doctors, Googling symptoms, avoiding activities |
Symptoms by Subtype
| Type | Main Symptom | Unique Feature |
|---|---|---|
| Somatic Symptom Disorder | Many symptoms across multiple body systems | Excessive health anxiety + repeated medical visits |
| Illness Anxiety Disorder | Few or no physical symptoms | Fear of having a serious illness (e.g., cancer, HIV) despite negative tests |
| Conversion Disorder | Neurological symptoms (paralysis, blindness, seizures, loss of speech) | Triggered by psychological stress; "La belle indifférence" (calm acceptance of severe symptom) |
| Pain Disorder | Chronic pain anywhere | Pain disproportionate to findings; mood and stress worsen it |
Common Physical Symptoms Reported
| System | Symptoms |
|---|---|
| Pain | Headache, back pain, joint pain, chest pain, pelvic pain |
| Gut | Nausea, bloating, vomiting, diarrhea, difficulty swallowing |
| Nervous system | Dizziness, weakness, paralysis, numbness, fainting, "pseudoseizures" |
| Heart/Lungs | Palpitations, shortness of breath (no cardiac/pulmonary cause) |
| Reproductive | Menstrual irregularities, sexual dysfunction |
| General | Fatigue, weakness, weight loss |
Behavioral Features
- Doctor-shopping (seeing multiple doctors for same complaints)
- Over-use of healthcare (frequent ER visits, tests)
- Resistance to psychological explanations
- Symptoms worsen with stress
- Relief when attention/care is given
4. DIAGNOSIS
Gold Standard Investigation
Clinical diagnosis using DSM-5 criteria + thorough medical evaluation to rule out organic causes first.
Diagnostic Approach
| Step | Action | Why |
|---|---|---|
| Step 1: Full medical workup | Blood tests, imaging, physical exam | Rule out real diseases (MS, lupus, thyroid, cancer, AIDS, etc.) |
| Step 2: Apply DSM-5 criteria | Check for the core triad for ≥6 months | Confirms somatic symptom disorder |
| Step 3: Psychiatric interview | Explore stress, trauma, emotional history | Uncovers psychological contributors |
| Step 4: Rule out other psychiatric disorders | Depression, anxiety, psychosis, malingering | These can mimic or co-exist with SSD |
| Step 5: Severity rating | PHQ-15 (somatic symptom checklist) | Measures symptom burden |
Key Differences from Related Conditions
| Condition | Key Difference |
|---|---|
| Factitious disorder | Patient deliberately FAKES or CREATES symptoms |
| Malingering | Patient PRETENDS for clear external gain (money, avoiding prison) |
| Illness anxiety disorder | Fear of HAVING disease; fewer actual symptoms |
| Depression | Physical symptoms due to underlying depressed mood |
5. MANAGEMENT
A. NON-PHARMACOLOGICAL MANAGEMENT
1. The Most Important First Step - The Doctor-Patient Relationship
| Approach | What to Do (Simple) |
|---|---|
| Acknowledge the suffering | "I believe your pain is real" - validate symptoms, don't dismiss |
| Regular scheduled visits | Don't wait for crises; see patient regularly to prevent ER overuse |
| Brief physical check | Examine the area of complaint at each visit to reassure |
| Avoid unnecessary tests | Repeated testing reinforces belief in physical disease |
| Never say "It's all in your head" | This destroys trust and worsens symptoms |
| Gently link stress and symptoms | "Stress can cause real physical symptoms in the body" |
2. Cognitive Behavioral Therapy (CBT) - Best Treatment
| What CBT Does | Simple Explanation |
|---|---|
| Identifies catastrophic thinking | "This pain means I have cancer" → challenge this thought |
| Relaxation training | Reduces physical tension and pain |
| Graded activity increase | Gradually do more despite symptoms |
| Reduces health anxiety | Helps patient stop Googling and over-checking body |
| Improves coping skills | Better emotional regulation = fewer somatic symptoms |
3. Other Psychological Approaches
| Therapy | Best For |
|---|---|
| Mindfulness-Based Therapy | Teaches acceptance of discomfort without catastrophizing |
| Psychodynamic Therapy | Explores unconscious emotional conflicts driving symptoms |
| Group Therapy | Support from others with similar experiences; reduces isolation |
| Family Therapy | Corrects family reinforcement of sick role |
4. Lifestyle Changes
| Change | Effect |
|---|---|
| Gentle regular exercise | ↓ Pain perception; ↑ endorphins |
| Regular sleep schedule | Poor sleep worsens somatic symptoms |
| Stress management | Reduces symptom flares |
| Reduce alcohol / caffeine | Both worsen anxiety and pain perception |
B. PHARMACOLOGICAL MANAGEMENT - Somatoform Disorder
Key principle: Medications are NOT the main treatment. They are used only when there is a clear comorbid depression, anxiety, or pain disorder.
| Drug Name | Drug Class | What It Treats | Dosage | Notes |
|---|---|---|---|---|
| Amitriptyline | Tricyclic Antidepressant (TCA) | Chronic pain + depression + sleep | 25 mg at night; increase to 75-150 mg/day | Low dose works for pain (different mechanism than antidepressant effect); sedating - good for sleep |
| Duloxetine | SNRI (Serotonin-Norepinephrine Reuptake Inhibitor) | Pain + depression + anxiety | 30 mg OD; increase to 60-120 mg/day | Best evidence for somatic pain syndromes; FDA approved for chronic pain (fibromyalgia, neuropathic pain) |
| Escitalopram | SSRI | Comorbid anxiety / depression driving somatic symptoms | Start 5 mg OD; increase to 10-20 mg OD | First-line if depression or anxiety is clearly co-existing |
| Sertraline | SSRI | Same as above | Start 25 mg OD; increase to 50-200 mg OD | Well tolerated; good for health anxiety |
| Pregabalin | Alpha-2-delta ligand | Fibromyalgia, neuropathic pain, anxiety | 75 mg BD; increase to 150-300 mg BD | Good for pain-predominant somatic disorders; also reduces anxiety |
| Gabapentin | Anticonvulsant / Alpha-2-delta ligand | Chronic pain, somatic pain syndromes | 300 mg TDS; increase as needed | Adjunct for pain management |
| Buspirone | Azapirone (5-HT1A agonist) | Illness anxiety with chronic worrying | 7.5-15 mg BD (max 60 mg/day) | Non-addictive; good for health anxiety component; slow onset |
| Low-dose antipsychotics (e.g., Quetiapine) | Atypical antipsychotic | Severe health anxiety / somatic delusions | 25-50 mg at night | Only if symptoms are near-delusional intensity; use cautiously |
Avoid: Benzodiazepines for long-term use (addiction risk, doesn't address core problem), opioids (worsen somatic focus and risk addiction)
PART 2: MOOD DISORDER
1. DEFINITION - "What is a Mood Disorder?"
- Normal thermostat = normal mood swings
- Major Depression = thermostat stuck on "too cold" (always down)
- Bipolar Disorder = thermostat swings wildly between "freezing" and "overheated"
Types of Mood Disorders
| Type | Simple Description |
|---|---|
| Major Depressive Disorder (MDD) | Severe persistent low mood + loss of interest for ≥2 weeks; no manic episodes |
| Persistent Depressive Disorder (Dysthymia) | Milder but longer-lasting depression (≥2 years) |
| Bipolar I Disorder | Full manic episodes + depressive episodes |
| Bipolar II Disorder | Hypomania (milder mania) + depressive episodes |
| Cyclothymic Disorder | Milder, shorter mood swings for ≥2 years |
| Premenstrual Dysphoric Disorder (PMDD) | Severe mood symptoms in the week before menstruation |
2. ETIOPATHOGENESIS (Chart Form)
MAJOR DEPRESSIVE DISORDER
══════════════════════════════════════════════
WHY DOES DEPRESSION HAPPEN?
══════════════════════════════════════════════
BIOLOGICAL: Brain Chemistry Imbalance
┌────────────────────────────────────────────┐
│ ↓ Serotonin (mood, sleep, appetite) │
│ ↓ Norepinephrine (energy, motivation) │
│ ↓ Dopamine (pleasure, reward) │
│ ↑ Cortisol (stress hormone - chronically) │
│ Overactive HPA axis │
│ Reduced hippocampus volume │
│ (stress kills brain cells here) │
└─────────────────┬──────────────────────────┘
│
══════════════════════════════════════════════
GENETIC FACTORS
┌────────────────────────────────────────────┐
│ Family history of depression (2-3x risk) │
│ Monozygotic twin concordance ~50% │
│ Serotonin transporter gene (5-HTTLPR) │
│ short allele → more stress-sensitive │
└─────────────────┬──────────────────────────┘
│
══════════════════════════════════════════════
PSYCHOLOGICAL FACTORS
┌────────────────────────────────────────────┐
│ Learned helplessness (feeling no control) │
│ Negative cognitive triad (Beck): │
│ → Negative view of self │
│ → Negative view of the world │
│ → Negative view of the future │
│ Loss, grief, trauma │
│ Low self-esteem │
└─────────────────┬──────────────────────────┘
│
══════════════════════════════════════════════
SOCIAL / ENVIRONMENTAL
┌────────────────────────────────────────────┐
│ Stressful life events (death, divorce, │
│ job loss, isolation) │
│ Chronic illness │
│ Substance abuse │
│ Lack of social support │
└─────────────────┬──────────────────────────┘
│
▼
══════════════════════════════════════════════
BRAIN GETS "STUCK" IN NEGATIVE STATE
Prefrontal cortex (thinking) slows down
Amygdala (emotion center) overactivates
Limbic system dysregulation
│
▼
MAJOR DEPRESSIVE DISORDER
══════════════════════════════════════════════
BIPOLAR DISORDER
══════════════════════════════════════════════
WHY DOES BIPOLAR DISORDER HAPPEN?
══════════════════════════════════════════════
STRONG GENETIC BASIS
(Heritability ~80%; strongest genetic link
of any psychiatric disorder)
│
DYSREGULATION of MULTIPLE neurotransmitters:
Serotonin ↓, Dopamine ↑ (mania) / ↓ (depression)
Norepinephrine fluctuates
Circadian rhythm genes disrupted
│
KINDLING THEORY:
Each mood episode makes the next one easier to trigger
(like a fire starting easier with each attempt)
│
▼
MOOD EPISODES SWING BETWEEN:
DEPRESSION ←──────────────→ MANIA/HYPOMANIA
══════════════════════════════════════════════
3. CLINICAL FEATURES / TRIADS
MAJOR DEPRESSIVE DISORDER - The SIG E CAPS Mnemonic
Diagnosis = 5 or more of these 9 symptoms for ≥2 weeks; must include #1 or #2
| Letter | Symptom | Simple Explanation |
|---|---|---|
| S | Sleep disturbance | Sleeping too much or too little; early morning waking |
| I | Interest loss (Anhedonia) | Can't enjoy things that used to bring happiness |
| G | Guilt / Worthlessness | Feels like a burden; blames self for everything |
| E | Energy loss | Exhausted all the time; even small tasks feel huge |
| C | Concentration problems | Can't focus, make decisions, or remember things |
| A | Appetite change | Eating too much or too little; significant weight change |
| P | Psychomotor changes | Moving/thinking slower (retardation) or more agitated |
| S | Suicidal thoughts | Thoughts of death, self-harm, or suicide |
- Depressed mood (feels sad, empty, hopeless most of the day, nearly every day), AND/OR
- Anhedonia (loss of interest/pleasure in almost all activities)
BIPOLAR DISORDER - Manic Episode (DIG FAST)
Mania = 3 or more of these (or 4 if mood is irritable only) for ≥1 week
| Letter | Symptom | Simple Explanation |
|---|---|---|
| D | Distractibility | Can't stay focused; jumps from thing to thing |
| I | Impulsivity / Irresponsibility | Risky behaviors: gambling, sex, spending sprees |
| G | Grandiosity | Feels special, powerful, chosen; may have delusions |
| F | Flight of ideas / Racing thoughts | Thoughts come too fast; hard to keep up |
| A | Activity increase / Agitation | Working on many projects; never sits still |
| S | Sleep decreased | Needs only 3-4 hours; feels fully rested |
| T | Talkativeness | Can't stop talking; pressured, loud speech |
Mood Episodes at a Glance
| Episode | Duration | Mood | Function |
|---|---|---|---|
| Major Depression | ≥2 weeks | Low, sad, empty | Impaired |
| Mania (Bipolar I) | ≥1 week | Elevated/euphoric OR irritable | Severely impaired; may need hospitalization |
| Hypomania (Bipolar II) | ≥4 days | Elevated/euphoric | Less impaired; no hospitalization needed |
| Mixed episode | ≥1 week | Both depressed AND manic symptoms simultaneously | Highly distressing and dangerous |
4. DIAGNOSIS
Gold Standard Investigation
Clinical interview using DSM-5 criteria - there is no blood test for mood disorders. Diagnosis is clinical, but tests help rule out medical causes.
Diagnostic Steps
| Step | Tool | Purpose |
|---|---|---|
| 1. Clinical Interview (DSM-5) | Gold Standard | Identify type and severity of mood episode |
| 2. PHQ-9 | Patient questionnaire (9 questions) | Screens and measures depression severity (score 0-27; ≥10 = moderate) |
| 3. MDQ (Mood Disorder Questionnaire) | 13-question screening tool | Screens specifically for bipolar disorder |
| 4. HDRS (Hamilton Depression Rating Scale) | Clinician-rated scale | Measures depression severity in detail |
| 5. Young Mania Rating Scale (YMRS) | Clinician-rated scale | Measures mania severity |
| 6. Rule out medical causes | TFTs (thyroid), FBC, metabolic panel, B12, folate, drug screen | Hypothyroidism, anemia, drug use all mimic depression |
| 7. MSE (Mental Status Exam) | Clinical assessment | Appearance, behavior, mood, affect, thought, perception, cognition, insight |
PHQ-9 Depression Severity
| Score | Severity |
|---|---|
| 0-4 | Minimal |
| 5-9 | Mild |
| 10-14 | Moderate |
| 15-19 | Moderately severe |
| 20-27 | Severe |
5. MANAGEMENT
A. NON-PHARMACOLOGICAL MANAGEMENT
1. Psychotherapy (Talking Therapies)
| Therapy | Best For | What It Does |
|---|---|---|
| CBT (Cognitive Behavioral Therapy) | Depression + Bipolar | Identifies negative thought patterns; replaces with realistic ones; prevents relapse |
| Interpersonal Therapy (IPT) | Depression | Focuses on relationships and life transitions that triggered depression |
| Behavioral Activation | Depression | Gets patient doing enjoyable activities again to break the "depression-inactivity-worsening" cycle |
| Mindfulness-Based CBT (MBCT) | Recurrent depression prevention | Teaches awareness to catch early warning signs of relapse |
| Psychoeducation | Bipolar | Teaching patient/family about the disorder, early warning signs, when to seek help |
| Family-Focused Therapy (FFT) | Bipolar | Involves family in treatment; reduces expressed emotion and conflict |
| IPSRT (Interpersonal & Social Rhythm Therapy) | Bipolar | Regularizes daily routines and sleep schedules → prevents mood episodes |
2. Lifestyle Modifications
| Change | Why It Helps |
|---|---|
| Regular sleep schedule | Critical in bipolar - irregular sleep triggers mood episodes |
| Regular aerobic exercise | As effective as antidepressants for mild-moderate depression; ↑ BDNF, ↓ cortisol |
| Avoid alcohol and recreational drugs | Both trigger and worsen depression and mania; interact with medications |
| Social connection and support | Isolation worsens depression; support groups are very helpful |
| Stress reduction | Stress triggers both depressive and manic episodes |
| Light therapy | For Seasonal Affective Disorder (SAD) - 10,000 lux lamp for 30 min each morning |
| Regular routine | Especially for bipolar - structured days stabilize mood |
3. For Severe/Suicidal Cases
| Intervention | When Used |
|---|---|
| Hospitalization | Active suicidal risk; severe mania; psychosis; inability to care for self |
| ECT (Electroconvulsive Therapy) | Severe treatment-resistant depression; suicidal emergency; works quickly |
| Crisis plan | Written safety plan with patient; emergency contacts; what to do if suicidal thoughts occur |
B. PHARMACOLOGICAL MANAGEMENT - MOOD DISORDERS (Table Form)
FOR MAJOR DEPRESSIVE DISORDER (MDD)
| Drug Name | Drug Class | Dosage | Key Notes |
|---|---|---|---|
| Fluoxetine (Prozac) | SSRI | 10 mg OD (start); 20-80 mg OD (therapeutic) | Longest half-life (4-6 days) - safest in overdose; least withdrawal; FDA-approved for MDD, OCD, bulimia |
| Sertraline (Zoloft) | SSRI | 25 mg OD (start); 50-200 mg OD | Most commonly prescribed; good safety profile; fewest drug interactions |
| Escitalopram (Lexapro) | SSRI | 5-10 mg OD (start); 10-20 mg OD | Most selective SSRI; very well tolerated; approved for MDD + GAD |
| Citalopram (Celexa) | SSRI | 10-20 mg OD (start); 20-40 mg OD (max 40 mg) | Well tolerated; avoid >40 mg (QT prolongation) |
| Paroxetine (Paxil) | SSRI | 10 mg OD (start); 20-50 mg OD | Most sedating SSRI; good for anxious depression; most discontinuation symptoms; weight gain |
| Venlafaxine XR (Effexor) | SNRI | 37.5-75 mg OD (start); 75-225 mg OD | Good for depression with chronic pain; monitor BP; useful in treatment-resistant depression |
| Duloxetine (Cymbalta) | SNRI | 30 mg OD (start); 60-120 mg OD | Good for MDD + pain + anxiety; FDA approved for multiple indications |
| Mirtazapine (Remeron) | NaSSA (noradrenergic) | 7.5-15 mg at night (start); 15-45 mg at night | Very sedating - good for insomnia + poor appetite; weight gain; works quickly |
| Bupropion (Wellbutrin) | NDRI (Norepinephrine-Dopamine) | 150 mg OD (start); 150 mg BD or 300 mg XL OD | No sexual side effects; weight neutral/loss; good for fatigue + concentration; avoid in seizure history/eating disorders |
| Amitriptyline | TCA | 25 mg at night (start); 100-200 mg/day | Effective but sedating; anticholinergic side effects; dangerous in overdose - second line |
| Imipramine | TCA | 25 mg TDS (start); 150-300 mg/day | Second-line; also used for panic disorder and bedwetting |
| Vortioxetine (Trintellix) | Serotonin modulator & stimulator | 5-10 mg OD (start); 10-20 mg OD | Newer; improves cognitive symptoms of depression; fewer sexual side effects |
FOR BIPOLAR DISORDER
| Drug Name | Drug Class | What It Treats | Dosage | Key Notes |
|---|---|---|---|---|
| Lithium | Mood Stabilizer (alkali metal) | Bipolar I & II - mania + depression prevention | 300 mg TDS (start); titrate to serum level 0.6-1.2 mEq/L for maintenance; 0.8-1.2 for acute mania | Gold standard mood stabilizer. Monitor: thyroid, kidneys, serum levels. Toxic level >1.5 mEq/L. Side effects: tremor, polyuria, weight gain, hypothyroidism. Works better in family history-positive patients |
| Valproate / Valproic Acid (Depakote) | Anticonvulsant / Mood Stabilizer | Acute mania; mixed states; rapid cycling | Start 250 mg BD-TDS; titrate to serum level 50-125 mcg/mL; usual 750-2500 mg/day | Better than lithium for mixed states and rapid cycling. Side effects: weight gain, hair loss, tremor, liver toxicity. Teratogenic - avoid in pregnancy (neural tube defects) |
| Carbamazepine (Tegretol) | Anticonvulsant / Mood Stabilizer | Acute mania; maintenance | 200 mg BD (start); increase to 400-1600 mg/day in divided doses | Better for bipolar patients with dysphoric mania or negative family history. Induces own metabolism. Blood count monitoring needed (agranulocytosis risk) |
| Lamotrigine (Lamictal) | Anticonvulsant / Mood Stabilizer | Bipolar depression + maintenance | 25 mg OD (start SLOWLY); increase over 6+ weeks to 100-400 mg/day | Best for bipolar depression. Must titrate slowly (Steven-Johnson syndrome risk if titrated fast). Little weight gain. Not good for acute mania |
| Quetiapine (Seroquel) | Atypical Antipsychotic | Acute mania + bipolar depression + maintenance | 50-100 mg at night (start); 300-800 mg/day (mania); 50-300 mg/day (depression) | Only atypical approved for BOTH poles of bipolar. Sedating - good for sleep. Weight gain, metabolic effects |
| Olanzapine (Zyprexa) | Atypical Antipsychotic | Acute mania; maintenance | 5-10 mg OD (start); 10-20 mg OD | Fast for acute mania; significant weight gain and metabolic syndrome risk |
| Aripiprazole (Abilify) | Atypical Antipsychotic (partial dopamine agonist) | Acute mania; maintenance; adjunct for MDD | 10-15 mg OD (start); 15-30 mg OD | Weight neutral; akathisia (restlessness) common; also FDA approved as adjunct antidepressant in MDD |
| Risperidone (Risperdal) | Atypical Antipsychotic | Acute mania with psychosis | 1-2 mg OD-BD (start); 2-6 mg/day | Good for mania with psychotic features; extrapyramidal side effects possible |
ANTIDEPRESSANT CAUTION IN BIPOLAR
Important: Standard antidepressants (SSRIs, SNRIs) used alone in bipolar disorder can trigger a manic switch or rapid cycling. Always combine with a mood stabilizer first.
Quick Summary Box - BOTH DISORDERS
| Topic | Somatoform Disorder | Mood Disorder |
|---|---|---|
| What is it? | Real physical symptoms from the mind, not body disease | Severe disturbance in mood (too low = depression; cycling = bipolar) |
| Core feature | Unexplained physical symptoms + excessive worry | Depressed mood / mania episodes |
| Gold standard Dx | Clinical interview + DSM-5 + rule out organic causes | Clinical interview + DSM-5 (PHQ-9 / MDQ screening) |
| Best non-drug Rx | CBT + therapeutic doctor-patient relationship | CBT / IPT / Behavioral Activation; Psychoeducation (bipolar) |
| 1st-line drug (depression) | SSRI/SNRI for comorbid anxiety/depression | SSRIs (fluoxetine, sertraline, escitalopram) |
| Pain-specific drug | Duloxetine or Amitriptyline | - |
| Bipolar mood stabilizer | - | Lithium (gold standard); Valproate; Lamotrigine (depression) |
| Avoid | Benzodiazepines long-term; opioids | Antidepressants alone in bipolar (risk of manic switch) |
| Prognosis | Chronic but manageable with CBT | Recurrent; requires long-term management |
- Kaplan & Sadock's Synopsis of Psychiatry, 12th Edition
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- Katzung's Basic and Clinical Pharmacology, 16th Edition
- Goldman-Cecil Medicine International Edition
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
- Stahl's Essential Psychopharmacology
definition , etiopathogenesis ( chart form ) , clinical features / triads , diagnosis ( gold standard investigation , MANAGEMENT ( NON PHARMACOLOGICAL ) , PHARMACOLOGICAL (TABLE FORM ) WITH DRUG NAME , DRUG CLASS , ITS DOSAGE OF HYPO- THYRIODISM ( IN A VERY SIMPLIFIED LANGUAGE )
"hypothyroidism" AND "levothyroxine" AND management
HYPOTHYROIDISM
1. DEFINITION - "What is Hypothyroidism?"
Simple Analogy
Normal thyroid = engine running perfectly Hypothyroidism = engine running too slow → car barely moves
Types by Cause
| Type | Where the Problem Is | Simple Explanation |
|---|---|---|
| Primary (most common) | Thyroid gland itself is damaged | Gland can't make enough hormone |
| Secondary (Central) | Pituitary gland not sending signal | Brain doesn't tell thyroid to work |
| Tertiary | Hypothalamus not sending signal | Even higher brain center is at fault |
| Subclinical | Mildly elevated TSH; normal T4 | Early/borderline; no or minimal symptoms |
| Congenital (Cretinism) | Baby born without functioning thyroid | Most severe; causes intellectual disability if untreated |
Key Facts
- Most common endocrine disorder (after diabetes)
- Affects women 10x more than men
- Most common age: 30-50 years (can occur at any age)
- #1 cause worldwide: Iodine deficiency
- #1 cause in developed countries: Hashimoto's thyroiditis (autoimmune)
2. ETIOPATHOGENESIS (Chart Form)
Simple Overview of Causes
══════════════════════════════════════════════
WHY DOES THE THYROID STOP WORKING?
══════════════════════════════════════════════
PRIMARY HYPOTHYROIDISM (Thyroid itself fails)
┌────────────────────────────────────────────┐
│ 1. AUTOIMMUNE (Hashimoto's Thyroiditis) │
│ Most common in developed countries │
│ Body attacks its own thyroid with │
│ antibodies (TPO-Ab, Tg-Ab) │
│ → Lymphocytes infiltrate thyroid │
│ → Fibrosis and destruction of gland │
│ │
│ 2. IODINE DEFICIENCY │
│ #1 cause worldwide │
│ No iodine → thyroid can't make T3/T4 │
│ → Gland grows big trying to compensate │
│ (GOITRE) │
│ │
│ 3. SURGERY (Thyroidectomy) │
│ Removal of thyroid → no hormone │
│ │
│ 4. RADIOIODINE THERAPY (¹³¹I) │
│ Used to treat hyperthyroidism → │
│ destroys too much thyroid tissue │
│ │
│ 5. DRUGS │
│ Amiodarone, Lithium, Carbimazole, │
│ PTU, Interferon-α → block thyroid │
│ hormone synthesis │
│ │
│ 6. INFILTRATIVE DISEASES │
│ Sarcoidosis, Amyloidosis, Haemochromatosis│
│ → Replace normal thyroid tissue │
│ │
│ 7. RADIATION to neck/head │
│ Damages thyroid cells │
└──────────────────┬─────────────────────────┘
│
══════════════════════════════════════════════
SECONDARY HYPOTHYROIDISM (Pituitary fails)
┌────────────────────────────────────────────┐
│ Pituitary tumour / damage │
│ → ↓ TSH secretion │
│ → Thyroid not stimulated → ↓ T3/T4 │
└──────────────────┬─────────────────────────┘
│
══════════════════════════════════════════════
CONGENITAL HYPOTHYROIDISM (Born with it)
┌────────────────────────────────────────────┐
│ Thyroid agenesis (gland missing) │
│ Thyroid dyshormonogenesis (defective │
│ enzyme can't make hormone) │
│ Iodine deficiency in mother during │
│ pregnancy → severe hypothyroidism │
│ in baby → CRETINISM if untreated │
└──────────────────┬─────────────────────────┘
│
▼
══════════════════════════════════════════════
RESULT: ↓ T3 and T4 in bloodstream
│
▼
Pituitary senses low T3/T4
→ TSH rises (trying to kick-start thyroid)
→ TSH keeps rising as thyroid fails more
│
▼
EVERY ORGAN SYSTEM SLOWS DOWN
(Hypometabolic state = everything runs slow)
══════════════════════════════════════════════
How Hashimoto's Destroys the Thyroid (Step-by-Step)
GENETIC PREDISPOSITION
(HLA-DR3, DR4, DR5; PTPN22, CTLA-4 variants)
+
ENVIRONMENTAL TRIGGER
(High iodine intake, low selenium,
infections, radiation, smoking cessation)
│
▼
AUTOIMMUNE ACTIVATION
• CD8+ Cytotoxic T-cells attack thyroid cells
• CD4+ T-cells produce cytokines
(TNF-α, IL-1, IFN-γ) → more destruction
• B-cells produce:
→ Anti-TPO Antibodies (Anti-Thyroid Peroxidase)
→ Anti-Thyroglobulin Antibodies (Anti-Tg)
→ TSH-Receptor Blocking Antibodies
│
▼
LYMPHOCYTIC INFILTRATION + FIBROSIS of thyroid
Germinal centre formation
Oxyphil (Hurthle cell) metaplasia
Loss of thyroid follicles
│
▼
↓ T4 and T3 production
↑ TSH (pituitary overcompensates)
│
▼
SUBCLINICAL → CLINICAL HYPOTHYROIDISM
3. CLINICAL FEATURES / TRIADS
The Classic Triad of Hypothyroidism
Fatigue + Weight Gain + Cold Intolerance
Complete Clinical Features by System
| Body System | Symptom / Sign | Simple Explanation |
|---|---|---|
| General | Fatigue, weakness, lethargy | Everything runs slow; feels like moving through mud |
| General | Weight gain (despite poor appetite) | Slow metabolism burns fewer calories; mainly fluid retention |
| General | Cold intolerance | ↓ heat production; always feels cold |
| Skin | Dry, rough, pale yellowish skin | ↓ sweating; ↑ glycosaminoglycans in skin; carotene accumulation gives yellow tinge |
| Skin | Non-pitting oedema (Myxoedema) | Fluid + glycosaminoglycans trapped in tissues; face, hands, shins puffed up without pitting |
| Face | Puffy face, periorbital oedema | Classic "moon face" with puffy around eyes |
| Hair/Nails | Dry, brittle hair; hair loss | Slow cell turnover; hair falls easily; outer third of eyebrow thinning |
| Heart | Bradycardia (slow pulse), diastolic hypertension | ↓ cardiac contractility and heart rate |
| Heart | Pericardial effusion | Fluid around heart (up to 30% of patients) |
| Gut | Constipation | Slow bowel movements |
| Muscles | Muscle weakness, cramps, aches | Slow muscle metabolism; may have myopathy |
| Nerves | Slow reflexes (delayed relaxation phase) | Classic sign - ankle jerk with slow relaxation |
| Brain | Slow thinking, poor memory, "brain fog" | Everything in brain runs slower |
| Brain | Depression | Low thyroid hormone directly affects mood |
| Voice | Hoarse, deep voice | Myxedema of vocal cords |
| Female | Menorrhagia, irregular periods | Hormonal imbalance from thyroid deficiency |
| Fertility | Reduced fertility, recurrent miscarriage | ↓ T4 impairs ovulation and fetal development |
| Lipids | ↑ Cholesterol, ↑ triglycerides | ↓ LDL receptor expression → dyslipidaemia |
| Blood | Anaemia (normocytic or macrocytic) | ↓ RBC production; or B12 deficiency (co-existing pernicious anaemia) |
Myxoedema Coma (Most Severe Form - Emergency!)
Untreated, severe hypothyroidism → life-threatening emergency
| Feature | Simple Explanation |
|---|---|
| Progressive stupor / coma | Brain completely slows down |
| Hypothermia (very low body temp) | No heat production |
| Hypoventilation | Breathing slows dangerously |
| Bradycardia, hypotension | Heart slowing to dangerously low rate |
| Hypoglycaemia | Glucose not mobilized |
| Hyponatraemia | Water retention dilutes sodium |
| Mortality up to 60% if untreated | Requires ICU treatment immediately |
Congenital Hypothyroidism (Cretinism) Features
| Feature | Simple Explanation |
|---|---|
| Short stature | Growth hormone-like effects of T4 absent |
| Intellectual disability | Brain development severely impaired without T4 |
| Coarse facial features | Myxoedema deposits |
| Large tongue (macroglossia) | Glycosaminoglycan deposits |
| Umbilical hernia | Low muscle tone |
| Delayed bone age | Slow skeletal development |
4. CLINICAL PHOTO

5. DIAGNOSIS
Gold Standard Investigation
Serum TSH (Thyroid Stimulating Hormone) - the SINGLE BEST test for diagnosing and monitoring hypothyroidism.
- TSH rises FIRST before T4 even falls → detects even early/subclinical hypothyroidism
- Sensitive to tiny changes in thyroid hormone levels
- TSH has a log-linear relationship with T4 → even small drops in T4 cause BIG rises in TSH
Diagnostic Criteria
| Test | Normal | Subclinical Hypothyroidism | Overt Hypothyroidism |
|---|---|---|---|
| TSH | 0.5-4.5 mIU/L | 4.5-10 mIU/L (elevated) | >10 mIU/L (often much higher) |
| Free T4 (FT4) | 0.8-1.8 ng/dL | Normal | Low |
| T3 | Normal | Usually normal | Low (less reliable test) |
| Anti-TPO antibodies | Negative | May be positive | Positive in >95% of Hashimoto's |
| Anti-Tg antibodies | Negative | May be positive | Positive in autoimmune cause |
Step-by-Step Diagnosis
| Step | Test | Interpretation |
|---|---|---|
| Step 1 | Serum TSH (gold standard screening test) | If elevated → go to Step 2 |
| Step 2 | Free T4 (FT4) | Low FT4 + high TSH = OVERT hypothyroidism; Normal FT4 + high TSH = SUBCLINICAL |
| Step 3 | Anti-TPO and Anti-Tg antibodies | Positive = Hashimoto's autoimmune cause |
| Step 4 | Full blood count (FBC) | Anaemia check |
| Step 5 | Lipid profile | ↑ Cholesterol, ↑ TG (reversible with treatment) |
| Step 6 | Creatine Kinase (CK) | Often elevated in hypothyroid myopathy |
| Step 7 | Thyroid ultrasound | Assess gland size, nodules, echogenicity |
| Special cases | MRI pituitary (if TSH low with low T4) | Secondary/central hypothyroidism |
| Newborn screening | TSH at day 5 (heel prick test) | Early detection of congenital hypothyroidism - before symptoms |
Secondary (Central) Hypothyroidism - Different!
Both TSH and FT4 are LOW (pituitary not secreting TSH) Use FT4 to monitor treatment (NOT TSH) in this case
6. MANAGEMENT
A. NON-PHARMACOLOGICAL MANAGEMENT
1. Dietary Changes
| Recommendation | Why | Simple Explanation |
|---|---|---|
| Adequate iodine intake | Iodine is needed to make thyroid hormone | Use iodized salt; eat fish, seafood, dairy |
| Selenium intake | Selenium helps T4 convert to active T3 | Brazil nuts, sunflower seeds, fish |
| Avoid goitrogens in large amounts | These foods block thyroid hormone production | Raw cruciferous vegetables (cabbage, broccoli, cauliflower) - cooking largely destroys goitrogens; soy in large amounts |
| Avoid excessive iodine | Paradoxically, too much iodine can also suppress thyroid (Wolff-Chaikoff effect) | Don't take iodine supplements without medical advice |
2. Medication Timing and Absorption Rules
Very important for patients on levothyroxine:
| Rule | Why |
|---|---|
| Take tablet on empty stomach, 30-60 min before breakfast | Food reduces absorption by up to 40% |
| Do not take with coffee | Coffee reduces absorption significantly |
| Take 4 hours apart from calcium tablets, iron supplements, antacids | These bind levothyroxine and reduce absorption |
| Take 4 hours apart from soy products and bran | Reduce T4 absorption |
| Never miss a dose for long periods | TSH rises, symptoms return |
3. Regular Monitoring
| What to Monitor | How Often |
|---|---|
| Serum TSH | Every 6-12 months once stable |
| After dose change | Recheck TSH in 6-8 weeks (takes this long to reach steady state) |
| Pregnancy | TSH every trimester (dose usually needs ↑ by 25-30%) |
| Lipid profile | Annually (hypothyroidism causes dyslipidaemia) |
| BP and heart rate | Regular check |
4. Lifestyle Modifications
| Change | Benefit |
|---|---|
| Regular gentle exercise | Combats fatigue, weight gain, mood changes |
| Warm clothing / warm environment | Manages cold intolerance until thyroid controlled |
| Manage stress | Stress worsens autoimmune thyroiditis |
| Adequate sleep | Fatigue management |
| Mental health support | Depression is common in hypothyroidism; may need short-term treatment |
5. Special Situations
| Situation | Non-Pharmacological Consideration |
|---|---|
| Pregnancy | Increase levothyroxine dose immediately upon positive test; TSH targets are stricter (0.1-2.5 mIU/L first trimester) |
| Newborns (congenital) | Neonatal screening + IMMEDIATE treatment essential for brain development |
| Surgery for goitre | Only if large compressive goitre; not for hypothyroidism itself |
| Radioiodine as cause | Post-treatment monitoring; start levothyroxine once hypothyroid |
B. PHARMACOLOGICAL MANAGEMENT (Table Form)
| Drug Name | Drug Class | How It Works (Simple) | Dosage | Key Notes |
|---|---|---|---|---|
| Levothyroxine (L-T4) (Synthroid, Eltroxin) | Synthetic thyroid hormone replacement (T4) | Replaces the missing thyroid hormone T4. Body converts T4 to active T3 in tissues as needed. | ADULTS: Start 50 mcg OD (morning, fasting); titrate every 6-8 weeks; maintenance 1.6-1.7 mcg/kg/day (average adult ~100-125 mcg/day). ELDERLY/cardiac patients: Start LOW at 12.5-25 mcg OD; increase by 12.5-25 mcg every 2-4 weeks. POST-THYROIDECTOMY (cancer): 2.2 mcg/kg/day (suppressive dose) | GOLD STANDARD treatment. Once-daily (half-life 7 days). Must take on empty stomach. TSH target: 0.5-2.5 mIU/L for most patients. Steady state takes 6-8 weeks after dose change. Excess: causes angina, AF, osteoporosis |
| Liothyronine (L-T3) (Cytomel) | Synthetic active thyroid hormone (T3) | Directly provides active T3 (no need for conversion). Faster-acting but shorter duration. | 5-25 mcg BD-TDS orally | Used when T4 alone is inadequate (T4-resistant symptoms). Not routine first-line. More cardiac risk (fluctuating T3 levels). Reserved for patients still symptomatic on T4 alone |
| Combined T4/T3 therapy | Thyroid hormone combination | Gives both hormones → some patients feel better with combination | T4 component: levothyroxine; T3 component: liothyronine in ratio approx 14:1 (T4:T3) by weight | For patients who remain symptomatic despite optimal T4 replacement with normal TSH. Genetic variations in deiodinase enzymes may explain why some patients need T3 supplementation. Keep TSH ≥1.0 mIU/L |
| Thyroid Extract (Desiccated Thyroid) (Armour Thyroid) | Natural combined T4 + T3 (porcine/bovine thyroid) | Natural preparation from animal thyroid glands; contains both T3 and T4 | 60-120 mg/day (1 grain = 60 mg); starting at 30 mg/day | Alternative to synthetic hormones; some patients prefer. T3:T4 ratio different from humans; fluctuating T3 levels. Use with caution in cardiac patients |
For MYXOEDEMA COMA (Emergency Treatment)
| Drug | Route | Dosage | Notes |
|---|---|---|---|
| Levothyroxine (IV) | Intravenous | Loading dose: 300-400 mcg IV stat; then 50-100 mcg IV daily | MUST give IV (poor oral absorption in coma) |
| Liothyronine (IV T3) | Intravenous | 5-20 mcg IV initially; then 2.5-10 mcg every 8 hours | Added for faster effect; more cardiotoxic - monitor closely |
| Hydrocortisone | Intravenous | 100 mg IV every 8 hours | Given until adrenal insufficiency is ruled out (secondary hypothyroidism may have coexisting Addison's) |
| Supportive care | - | Ventilation, IV fluids (cautiously), warming, treat infection | Treat the cause (most often infection, cold exposure, medications) |
For SUBCLINICAL HYPOTHYROIDISM
| When to Treat | When NOT to Treat |
|---|---|
| TSH >10 mIU/L (treat all) | TSH 4.5-10 with no symptoms and no antibodies |
| TSH 4.5-10 with positive TPO antibodies | Elderly (>70 yrs) with mild TSH elevation |
| TSH 4.5-10 with symptoms | Pregnancy may be exception - treat |
| Pregnancy (any TSH above trimester reference) | Always weigh individual risks/benefits |
Target TSH Ranges
| Patient | Target TSH |
|---|---|
| Most adults | 0.5-2.5 mIU/L |
| Elderly (>70 yrs) | 1.0-4.0 mIU/L (slightly higher acceptable) |
| Pregnancy (1st trimester) | 0.1-2.5 mIU/L |
| Pregnancy (2nd trimester) | 0.2-3.0 mIU/L |
| Pregnancy (3rd trimester) | 0.3-3.0 mIU/L |
| Thyroid cancer (suppressive) | <0.1 mIU/L |
Drugs That Interfere with Levothyroxine
| Drug | Effect |
|---|---|
| Calcium tablets, iron supplements, antacids (Al/Mg) | ↓ Levothyroxine absorption (give 4 hours apart) |
| Cholestyramine, colestipol | ↓ Absorption |
| Rifampicin, phenytoin, carbamazepine | ↑ Levothyroxine metabolism → need higher dose |
| Amiodarone | Causes hypothyroidism itself; also interferes with T4-T3 conversion |
| Lithium | Blocks thyroid hormone synthesis → hypothyroidism |
| Sertraline, phenobarbitone | ↑ T4 clearance → need dose increase |
Quick Summary Box
| Topic | Key Point |
|---|---|
| What is it? | Thyroid gland makes too little hormone → everything in body slows down |
| #1 cause worldwide | Iodine deficiency |
| #1 cause in developed countries | Hashimoto's autoimmune thyroiditis |
| Classic Triad | Fatigue + Weight gain + Cold intolerance |
| Skin sign | Non-pitting myxoedema (puffy face, pretibial oedema) |
| Gold standard test | Serum TSH (best single test) |
| Confirm with | Free T4 (low); Anti-TPO antibodies (positive in Hashimoto's) |
| Gold standard treatment | Levothyroxine (L-T4) once daily, fasting |
| Usual adult dose | 1.6-1.7 mcg/kg/day (~100-125 mcg/day) |
| Elderly/cardiac patients | Start LOW (12.5-25 mcg) and go SLOW |
| TSH target | 0.5-2.5 mIU/L |
| Recheck TSH after dose change | After 6-8 weeks |
| Myxoedema coma treatment | IV Levothyroxine 300-400 mcg loading + ICU care |
| Congenital - when to treat | IMMEDIATELY after birth (heel prick screen positive) |
| Key absorption rule | Take on EMPTY stomach; 4 hours away from calcium/iron |
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), pp. 3072-3074
- Katzung's Basic and Clinical Pharmacology, 16th Edition, pp. 1088-1090
- Textbook of Family Medicine, 9th Edition, pp. 1022-1023
- Goldman-Cecil Medicine International Edition
- Berek & Novak's Gynecology (thyroid in women/pregnancy)
- Rosen's Emergency Medicine (Myxoedema coma management)
- Goodman & Gilman's Pharmacological Basis of Therapeutics
definition , etiopathogenesis ( chart form ) , clinical features / triads , diagnosis ( gold standard investigation , MANAGEMENT ( NON PHARMACOLOGICAL ) , PHARMACOLOGICAL (TABLE FORM ) WITH DRUG NAME , DRUG CLASS , ITS DOSAGE OF HYPER THYRIODISM ( IN A VERY SIMPLIFIED LANGUAGE )
"hyperthyroidism" AND "Graves disease" AND treatment
definition , etiopathogenesis ( chart form ) , clinical features / triads , diagnosis ( gold standard investigation , MANAGEMENT ( NON PHARMACOLOGICAL ) , PHARMACOLOGICAL (TABLE FORM ) WITH DRUG NAME , DRUG CLASS , ITS DOSAGE OF HYPER THYRIODISM ( IN A VERY SIMPLIFIED LANGUAGE )
HYPERTHYROIDISM (THYROTOXICOSIS)
1. DEFINITION - "What is Hyperthyroidism?"
Simple Analogy
Normal thyroid = car engine running at the right speed Hyperthyroidism = engine running at full throttle, non-stop → overheats, burns out
Key Facts
- Most common cause: Graves' disease (autoimmune) - accounts for 60-80% of all cases
- Women affected 7-10x more than men
- Peak age: 20-40 years
- Can affect every organ system in the body
- Left untreated → can cause heart failure, atrial fibrillation, osteoporosis
- Most severe emergency: Thyroid Storm (life-threatening)
2. ETIOPATHOGENESIS (Chart Form)
Causes of Hyperthyroidism - Overview
═══════════════════════════════════════════════════════
WHY DOES THE THYROID MAKE TOO MUCH HORMONE?
═══════════════════════════════════════════════════════
PRIMARY HYPERTHYROIDISM (Thyroid itself is overactive)
┌─────────────────────────────────────────────────────┐
│ 1. GRAVES' DISEASE (Most Common - 60-80%) │
│ Autoimmune condition │
│ Body makes STIMULATING antibodies (TSI/TRAb) │
│ → These act like TSH and SWITCH ON thyroid │
│ permanently → non-stop hormone production │
│ Triad: Goitre + Eye disease + Skin changes │
│ │
│ 2. TOXIC MULTINODULAR GOITRE (Plummer's Disease) │
│ Multiple lumps in thyroid │
│ Each lump produces its own hormones │
│ autonomously (without TSH control) │
│ Most common in OLDER patients │
│ │
│ 3. TOXIC ADENOMA (Single Hot Nodule) │
│ One lump that works independently │
│ Produces excess hormone without control │
│ │
│ 4. IODINE EXCESS (Jod-Basedow Phenomenon) │
│ Too much iodine → triggers thyroid to │
│ overproduce hormones │
│ Seen with: Amiodarone (high iodine content), │
│ contrast dye, iodine supplements │
│ │
│ 5. THYROIDITIS (Leaked hormones - NOT true │
│ hyperthyroidism - "thyrotoxicosis without │
│ hyperthyroidism") │
│ Subacute (De Quervain's) thyroiditis │
│ Silent/postpartum thyroiditis │
│ → Inflamed gland leaks stored hormones │
│ → TRANSIENT thyrotoxicosis, then hypothyroid │
│ │
│ 6. FACTITIOUS THYROTOXICOSIS │
│ Taking too many thyroid hormone tablets │
└──────────────────┬──────────────────────────────────┘
│
SECONDARY HYPERTHYROIDISM (Pituitary overdrives thyroid)
┌─────────────────────────────────────────────────────┐
│ TSH-secreting pituitary adenoma (rare) │
│ → ↑↑ TSH → overstimulates thyroid → ↑ T3/T4 │
└──────────────────┬──────────────────────────────────┘
│
▼
═══════════════════════════════════════════════════════
GRAVES' DISEASE MECHANISM (MOST IMPORTANT)
═══════════════════════════════════════════════════════
How Graves' Disease Develops (Step-by-Step)
GENETIC PREDISPOSITION
(HLA-DR3, HLA-B8; CTLA-4, PTPN22 gene variants)
+
TRIGGER FACTORS
(Stress, infection, pregnancy, postpartum,
smoking, immune checkpoint inhibitors,
alemtuzumab, HAART therapy)
│
▼
AUTOIMMUNE ACTIVATION
• B-lymphocytes produce
THYROID STIMULATING IMMUNOGLOBULINS (TSI)
also called TSH Receptor Antibodies (TRAb)
│
▼
TRAb BINDS TSH RECEPTOR ON THYROID CELLS
• Mimics TSH → CONTINUOUSLY stimulates thyroid
• TSH receptor never "turns off"
• Thyroid keeps producing T3 and T4 non-stop
│
▼
↑↑↑ T3 and T4 in bloodstream
Pituitary senses excess → shuts down TSH
(TSH becomes very LOW in Graves')
│
▼
EVERY ORGAN SYSTEM SPEEDS UP
(Hypermetabolic state = everything in overdrive)
═══════════════════════════════════════════════════════
OPHTHALMOPATHY IN GRAVES' (Eye Disease)
═══════════════════════════════════════════════════════
CD8+ T-cells infiltrate extraocular muscles
↓
Cytokines released (TNF, IFN-γ, IL-1)
↓
Fibroblasts activated → produce glycosaminoglycans
→ Water trapped → Muscle swelling + Fat increase
→ PROPTOSIS (eyeballs pushed forward)
→ Diplopia, corneal damage, optic nerve compression
3. CLINICAL FEATURES / TRIADS
THE CLASSIC TRIAD OF GRAVES' DISEASE
Goitre + Exophthalmos (bulging eyes) + Pretibial Myxoedema
Clinical Features Image (Harrison's)

Complete Clinical Features by System
| Body System | Symptom / Sign | Simple Explanation |
|---|---|---|
| General | Weight loss despite increased appetite | Metabolic rate in overdrive, burning everything |
| General | Heat intolerance, sweating | Body generating too much heat |
| General | Fatigue and weakness | Muscles depleted from overactivity |
| Heart | Palpitations, tachycardia (fast heart) | Most common cardiac sign; >100 bpm at rest |
| Heart | Atrial fibrillation | Common in elderly; 10-35% of cases |
| Heart | Widened pulse pressure, bounding pulse | High cardiac output |
| Heart | Heart failure | In severe or untreated cases |
| Nervous system | Anxiety, irritability, hyperactivity | Brain running too fast |
| Nervous system | Fine tremor of hands | Best seen when fingers stretched out |
| Nervous system | Insomnia, poor concentration | Can't "switch off" |
| Nervous system | Hyperreflexia (brisk reflexes) | Exaggerated tendon reflexes |
| Muscles | Proximal muscle weakness | Difficulty climbing stairs, rising from chair |
| Skin | Warm, moist, sweaty skin | ↑ blood flow and metabolism |
| Skin | Palmar erythema (red palms) | ↑ blood flow |
| Skin | Onycholysis (nails separate from bed) | Plummer's nails |
| Hair | Diffuse hair thinning (alopecia) | Rapid cell turnover disrupts hair cycle |
| Gut | Increased stool frequency/diarrhoea | ↑ gut motility |
| Female | Oligomenorrhoea/amenorrhoea | Hormonal disruption |
| Male | Impaired sexual function, gynecomastia | Sex hormone imbalance |
| Bones | Osteoporosis, fracture risk | T3/T4 directly resorb bone; ↑ calcium |
| Eyes (Graves' only) | Proptosis (exophthalmos) | Eyeballs pushed forward |
| Eyes (Graves' only) | Lid retraction, lid lag | Sympathetic overactivity + muscle swelling |
| Eyes (Graves' only) | Diplopia, periorbital oedema | Extraocular muscle inflammation |
| Eyes (Graves' only) | Optic nerve compression | Most severe - can cause blindness |
| Skin (Graves' only) | Pretibial myxoedema | Thickened, nodular skin on shins (looks like orange peel) |
| Fingers (Graves' only) | Thyroid acropachy | Clubbing of fingers (rare) |
Graves' Eye Disease - NO SPECS Scoring System
| Class | Meaning |
|---|---|
| N = No signs or symptoms | Normal |
| O = Only lid retraction/lag | Sympathetic overactivity |
| S = Soft tissue involvement | Periorbital oedema, chemosis |
| P = Proptosis (>22 mm) | Eyeball pushed forward |
| E = Extraocular muscle involvement | Diplopia |
| C = Corneal involvement | Corneal exposure/ulceration |
| S = Sight loss | Optic nerve compression → vision loss |
Apathetic Thyrotoxicosis (Elderly patients - Different Presentation!)
Elderly patients may NOT show the "classic" overactive symptoms. Instead they present with: fatigue, weight loss, depression, atrial fibrillation - easily missed! Called "apathetic thyrotoxicosis"
Thyroid Storm (Most Severe Emergency!)
| Feature | Simple Explanation |
|---|---|
| Hyperpyrexia (very high fever >40°C) | Metabolic overdrive generates extreme heat |
| Extreme tachycardia, arrhythmias | Heart racing dangerously fast |
| Agitation, delirium, coma | Brain in crisis |
| Severe vomiting, diarrhoea | GI in overdrive |
| Heart failure | Heart cannot keep up |
| Mortality 20-50% if untreated | ICU emergency |
| Precipitated by: infection, surgery, trauma, iodine load, stopping antithyroid drugs | Sudden "flood" of thyroid hormone |
4. DIAGNOSIS
Gold Standard Investigation
Serum TSH (Thyroid Stimulating Hormone) - SINGLE BEST test for diagnosis and monitoring
- TSH falls FIRST before T4 even rises → earliest and most sensitive indicator
- In primary hyperthyroidism: TSH is very low (suppressed) because the pituitary is "switched off" by excess T3/T4
- A normal TSH virtually rules out primary hyperthyroidism
Step-by-Step Diagnostic Approach
| Step | Test | What You Find in Hyperthyroidism |
|---|---|---|
| Step 1 | Serum TSH (Gold Standard screening) | Suppressed/Undetectable TSH (<0.1 mIU/L) |
| Step 2 | Free T4 (FT4) | High FT4 = overt hyperthyroidism |
| Step 3 | Free T3 (FT3) | Sometimes only T3 is elevated (T3 toxicosis) |
| Step 4 | TSH Receptor Antibodies (TRAb) | Positive = Graves' disease (confirms autoimmune cause) |
| Step 5 | Anti-TPO antibodies | Positive in 80% of Graves' |
| Step 6 | Radioactive Iodine Uptake (RAIU) scan | ↑↑ uptake = Graves'/toxic nodule; ↓ uptake = thyroiditis/factitious |
| Step 7 | Thyroid ultrasound | Goitre size, nodules, vascularity (Graves' shows ↑↑ vascularity) |
| Special | Thyroid scintigraphy (¹²³I scan) | Differentiates Graves' (diffuse uptake) vs toxic nodule (focal uptake) vs thyroiditis (no uptake) |
Diagnostic Values Summary
| Test | Normal | Hyperthyroidism (Primary) | Secondary Hyperthyroidism (Pituitary TSHoma) |
|---|---|---|---|
| TSH | 0.5-4.5 mIU/L | ↓↓ Suppressed (<0.1) | ↑ Elevated |
| Free T4 | 0.8-1.8 ng/dL | ↑ Elevated | ↑ Elevated |
| Free T3 | 2.3-4.2 pg/mL | ↑ Elevated | ↑ Elevated |
| TRAb | Negative | Positive (Graves') | Negative |
Key Rule: Low TSH + High FT4 + High FT3 = Primary Hyperthyroidism until proven otherwise
5. MANAGEMENT
A. NON-PHARMACOLOGICAL MANAGEMENT
1. Lifestyle Modifications
| What to Do | Why | Simple Explanation |
|---|---|---|
| Rest adequately | Body already in overdrive | Reduces adrenergic load on heart |
| Avoid caffeine and stimulants | Makes palpitations, anxiety, tremor worse | Coffee/energy drinks worsen tachycardia |
| High-calorie, high-protein diet | Body is burning calories at very high rate | Prevent weight loss and muscle wasting |
| Calcium and Vitamin D supplements | Hyperthyroidism causes bone loss (osteoporosis) | Protect bones from T3/T4 bone resorption effect |
| Avoid iodine-rich foods (temporarily) | Iodine can worsen hyperthyroidism | Avoid seaweed, iodized supplements, contrast dye if possible |
| Quit smoking (Graves' eye disease) | Smoking STRONGLY worsens Graves' ophthalmopathy | Doubles the risk of severe eye disease |
| Stress management | Stress triggers/worsens autoimmune activity | Relaxation, yoga, counselling |
| Regular gentle exercise (once stable) | Improves cardiovascular fitness | Once thyroid is controlled with medication |
| Cool environment | Heat intolerance is a major symptom | Fans, light clothing, air conditioning |
2. Eye Care (Graves' Ophthalmopathy)
| Measure | Purpose |
|---|---|
| Lubricating eye drops (artificial tears) | Prevent corneal drying/damage |
| Dark sunglasses | Protect from light sensitivity and wind |
| Elevate head when sleeping | Reduce periorbital oedema |
| Selenium 200 mcg/day (mild-moderate eye disease) | Reduces progression of eye disease |
| Ophthalmology referral | For proptosis, diplopia, optic nerve involvement |
| IV Methylprednisolone pulse therapy | For moderate-severe active eye disease |
| Teprotumumab (monoclonal antibody) | FDA-approved 2020; blocks IGF-1R pathway; reduces proptosis |
| Orbital radiotherapy | For moderate-severe; reduces muscle inflammation |
| Orbital decompression surgery | When optic nerve compression threatens vision |
3. Ablative Therapies (Definitive / Long-term)
Radioactive Iodine (¹³¹I) Therapy
- Taken as a single oral capsule/drink
- Thyroid cells absorb the radioactive iodine
- Radiation destroys overactive thyroid tissue over weeks-months
- Dose: 370-555 MBq (10-15 mCi) typically
- Result: ~90% achieve remission; most eventually develop hypothyroidism (need lifelong levothyroxine)
- Contraindicated in: Pregnancy, breastfeeding, active severe Graves' eye disease
- Precautions after: Avoid close contact with children/pregnant women for 5-7 days
Thyroidectomy (Surgery)
- Total or subtotal removal of the thyroid gland
- Indications: Large goitre causing compression, preference for rapid cure, pregnancy (2nd trimester), allergy to antithyroid drugs, suspected malignancy, failed radioiodine
- Preparation required: Patient must be made euthyroid with antithyroid drugs FIRST (prevents thyroid storm intra-operatively)
- Plus potassium iodide (Lugol's solution) for 10-14 days before surgery → reduces gland vascularity and makes surgery safer
- Complications: Hypocalcaemia (parathyroid damage), recurrent laryngeal nerve injury (hoarse voice)
- Result: Requires lifelong levothyroxine replacement afterwards
B. PHARMACOLOGICAL MANAGEMENT (Table Form)
FIRST-LINE: ANTITHYROID DRUGS (THIOAMIDES)
| Drug Name | Drug Class | How It Works (Simple) | Dosage | Key Notes |
|---|---|---|---|---|
| Methimazole (MMI) (Tapazole) | Thioamide antithyroid drug | Blocks thyroid peroxidase enzyme → thyroid CANNOT make T3 or T4 anymore. Also reduces TSH-receptor antibody levels. | INITIAL (moderate-severe): 20-40 mg OD orally INITIAL (mild): 10-20 mg OD MAINTENANCE (titration regimen): 2.5-10 mg OD Block-replace regimen: 20-40 mg/day fixed + levothyroxine | DRUG OF CHOICE - once daily dosing (half-life 6 hrs). Achieves euthyroid in 3-8 weeks. Avoid in 1st trimester pregnancy (risk of congenital malformations). Monitor for agranulocytosis. |
| Propylthiouracil (PTU) | Thioamide antithyroid drug | Blocks thyroid peroxidase (same as MMI) PLUS blocks conversion of T4 → active T3 in peripheral tissues (extra benefit in thyroid storm). | INITIAL: 100-200 mg every 6-8 hours (3-4x daily) MAINTENANCE: 50-100 mg every 8-12 hours Thyroid storm: 500-1000 mg loading, then 250 mg every 4 hours | 2nd line to MMI due to risk of severe hepatitis (BLACK BOX WARNING). Preferred in: 1st trimester pregnancy (less placental crossing), thyroid storm. More strongly protein-bound → less crosses placenta. Divided doses required (short half-life 90 min). |
| Carbimazole | Thioamide (prodrug of methimazole) | Converted to methimazole in the body → same mechanism as MMI | INITIAL: 20-40 mg/day in divided doses MAINTENANCE: 5-15 mg/day | Available in UK/Europe; not available in USA. Effectively interchangeable with methimazole. Same precautions. |
ADJUNCT: BETA-BLOCKERS (Symptom Control)
| Drug Name | Drug Class | How It Works (Simple) | Dosage | Key Notes |
|---|---|---|---|---|
| Propranolol | Non-selective beta-blocker | Blocks adrenaline-like effects of thyroid hormone → controls fast heart, tremor, anxiety, sweating. BONUS: also blocks T4→T3 conversion (unique among beta-blockers). | 20-40 mg every 6 hours orally IV (thyroid storm): 1-2 mg IV slowly; repeat as needed | Preferred beta-blocker in thyrotoxicosis. Used in early treatment before antithyroid drugs take effect (3-4 weeks). Also used in thyroid storm. Avoid in asthma/COPD. Controls symptoms only - does NOT treat the underlying disease. |
| Atenolol | Selective beta-1 blocker | Selectively blocks heart's beta-1 receptors → slows heart rate, reduces palpitations | 25-100 mg OD | Better choice if patient has asthma/COPD (more selective). Once-daily dosing → better adherence |
| Esmolol | Ultra-short-acting IV beta-1 blocker | Very fast-acting IV beta blocker; easy to titrate | Loading 250-500 mcg/kg IV, then 50-100 mcg/kg/min infusion | Used in thyroid storm when rapid beta-blockade needed or concerns about tolerability |
| Metoprolol | Selective beta-1 blocker | Slows heart rate specifically | 25-100 mg BD | Alternative to atenolol; useful if asthma present |
ADJUNCT: IODIDES (Short-term / Pre-surgery / Thyroid Storm)
| Drug Name | Drug Class | How It Works (Simple) | Dosage | Key Notes |
|---|---|---|---|---|
| Potassium Iodide - Saturated Solution (SSKI) | Iodide solution | High doses of iodine paradoxically BLOCK thyroid hormone release (Wolff-Chaikoff effect). Also reduces vascularity of thyroid → safer surgery. Works within 2-7 days. | Pre-surgery: 5 drops (250 mg) 3x daily for 10-14 days Thyroid storm: 5 drops (250 mg) every 6 hours | MUST give at least 1 hour AFTER antithyroid drug (otherwise iodine worsens the storm). SHORT-TERM USE ONLY - gland "escapes" block after 2-8 weeks. Do NOT use if radioiodine therapy planned. Avoid in pregnancy (risk of fetal goitre). |
| Lugol's Solution (Strong Iodine Solution) | Iodide preparation | Same as SSKI - blocks hormone release and reduces thyroid vascularity | Pre-surgery: 8-10 drops TDS for 10-14 days Thyroid storm: 10 drops every 8 hours | Used pre-thyroidectomy. Contains both iodine (5%) and potassium iodide (10%). Give AFTER antithyroid drug started. |
ADJUNCT: CORTICOSTEROIDS (Thyroid Storm / Eye Disease)
| Drug Name | Drug Class | How It Works (Simple) | Dosage | Key Notes |
|---|---|---|---|---|
| Hydrocortisone | Corticosteroid | Blocks T4→T3 conversion. Treats relative adrenal insufficiency in thyroid storm (stress hormones depleted). | Thyroid storm: 300 mg IV loading, then 100 mg IV every 8 hours | Essential in thyroid storm management. Continue until storm resolved. |
| Dexamethasone | Corticosteroid | Same as hydrocortisone; more potent, longer acting | 2-4 mg IV every 6 hours | Alternative to hydrocortisone in thyroid storm. Also given pre-operatively. |
| Methylprednisolone | Corticosteroid | Reduces orbital inflammation in Graves' eye disease | IV pulse: 500 mg-1 g IV weekly for 6-12 weeks (for moderate-severe ophthalmopathy) | Standard of care for active moderate-severe Graves' ophthalmopathy. |
FOR GRAVES' OPHTHALMOPATHY - SPECIALIST DRUG
| Drug Name | Drug Class | How It Works (Simple) | Dosage | Key Notes |
|---|---|---|---|---|
| Teprotumumab (Tepezza) | Monoclonal antibody (IGF-1R inhibitor) | Blocks insulin-like growth factor-1 receptor (IGF-1R) on orbital fibroblasts → reduces retrobulbar tissue expansion → reduces proptosis | 10 mg/kg IV infusion (1st dose), then 20 mg/kg IV every 3 weeks × 8 infusions total | FDA-approved January 2020. First disease-modifying treatment for Graves' eye disease. Significantly reduces proptosis (eye bulging). Expensive. |
THYROID STORM EMERGENCY PROTOCOL
ORDER OF DRUGS IS CRITICAL - must give in sequence below:
| Order | Drug | Dose | Purpose |
|---|---|---|---|
| 1st | Propranolol (beta-blocker) | 20-40 mg PO / 1-2 mg IV every 4 hours | Control heart rate immediately |
| 2nd | PTU (propylthiouracil) | 500-1000 mg loading, then 250 mg q4h | Block new hormone synthesis AND T4→T3 conversion |
| 2nd (alt) | Methimazole | 20-25 mg every 4-6 hours | If PTU not available |
| 3rd (≥1 hr after PTU) | Lugol's iodine or SSKI | 10 drops q8h / 5 drops q6h | Block hormone RELEASE (give ONLY after antithyroid drug!) |
| 4th | Hydrocortisone | 300 mg IV load, 100 mg q8h | Block T4→T3; treat adrenal crisis |
| Supportive | Paracetamol/Acetaminophen | Standard doses | Fever control (NOT aspirin - aspirin displaces T4 from protein → worsens storm) |
| Supportive | Cooling blankets, IV fluids, benzodiazepines | As needed | Temperature control, fluid replacement, agitation |
| If iodine allergy | Lithium carbonate | 300 mg every 6 hours (oral/NG) | Blocks hormone release (alternative to iodine) |
Quick Summary Box
| Topic | Key Point |
|---|---|
| What is it? | Thyroid makes too much hormone → everything in body speeds up |
| Most common cause | Graves' disease (autoimmune TSH-receptor antibodies) |
| Graves' Triad | Goitre + Exophthalmos (bulging eyes) + Pretibial myxoedema |
| Classic symptoms | Weight loss despite eating more, palpitations, heat intolerance, tremor, anxiety |
| Gold standard test | Serum TSH (suppressed/low in primary hyperthyroidism) |
| Confirm with | Free T4 (high) + TRAb antibodies (positive in Graves') |
| Radioiodine uptake scan | Differentiates Graves' (↑ diffuse) vs thyroiditis (↓) vs toxic nodule (focal) |
| Drug of choice | Methimazole (once daily; 20-40 mg initially) |
| Pregnancy 1st trimester | PTU preferred (less placental crossing; methimazole teratogenic) |
| Pregnancy 2nd/3rd trimester | Switch back to Methimazole (PTU hepatotoxicity risk) |
| Beta-blocker of choice | Propranolol (also blocks T4→T3 conversion) |
| Pre-surgery preparation | Antithyroid drug → Lugol's iodine (10-14 days) → Surgery |
| Thyroid storm drug order | Propranolol → PTU → Iodine (wait 1 hr!) → Hydrocortisone |
| Do NOT give in thyroid storm | Aspirin (displaces T4 from protein → worsens storm) |
| Radioiodine contraindications | Pregnancy, breastfeeding, severe active eye disease |
| Definitive cure | Radioiodine OR Thyroidectomy (both usually cause hypothyroidism → need levothyroxine) |
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), pp. 3075-3083
- Katzung's Basic and Clinical Pharmacology, 16th Edition, pp. 1083-1092
- Lippincott Illustrated Reviews - Pharmacology, pp. 783-785
- Rosen's Emergency Medicine, 9th Edition (Thyroid Storm protocol)
- Goodman & Gilman's Pharmacological Basis of Therapeutics, 14th Edition
- Sabiston Textbook of Surgery, 21st Edition