I now have solid textbook content. Let me compile this into a comprehensive, practical prescription guide for a first-year intern in Ophthalmology OPD.
Ophthalmology OPD - Common Prescriptions for Interns
You're going to be fine. Here's a practical, condition-by-condition guide for the most common patients you'll see. For anything that looks serious (severe pain, sudden vision loss, trauma, suspected glaucoma attack), refer to a senior immediately.
🚦 FIRST - How to Quickly Sort Your Patient
Ask 4 questions:
- Itchy? → Think allergic
- Discharge (sticky/mucoid)? → Think bacterial
- Watery + recent URTI / contact with someone with red eye? → Think viral
- Pain + photophobia + blurred vision? → REFER - don't manage alone
1. BACTERIAL CONJUNCTIVITIS
Presentation: Mucopurulent sticky discharge, both eyes (often), no vision change, no significant pain.
Rx:
Ciprofloxacin 0.3% eye drops - 1 drop in affected eye(s) QID × 5-7 days
OR
Tobramycin 0.3% eye drops - 1 drop QID × 5-7 days
OR (cheap & effective)
Chloramphenicol 0.5% eye drops - 1 drop QID × 5 days
- Add Chloramphenicol 1% eye ointment at night (lubricates + treats)
- Counsel: wash hands, don't share towels, do not rub eyes
From Histology A Text and Atlas: Bacterial conjunctivitis is usually treated with antibiotic eye drops or ointments.
2. VIRAL CONJUNCTIVITIS
Presentation: Watery discharge, follicles, unilateral first then bilateral, recent cold/sore throat, very contagious. No pus.
No antibiotic needed. Treatment is supportive.
Rx:
Carboxymethylcellulose (CMC) 0.5% / Hydroxypropyl methylcellulose (HPMC) eye drops
- 1 drop QID (artificial tears for comfort)
Cold compresses 3-4 times/day
If severe inflammation (membranous EKC):
Prednisolone 0.5% eye drops QID (only after ruling out herpes - get senior opinion)
- Self-limiting: resolves in 2-3 weeks
- Strict hygiene: hand wash, no towel sharing, disinfect surfaces
- Stop contact lenses until resolved
From Kanski's Clinical Ophthalmology 10th ed.: "Spontaneous resolution of adenoviral infection usually occurs within 2-3 weeks, so specific treatment is typically unnecessary."
3. ALLERGIC CONJUNCTIVITIS
Presentation: Bilateral itching (hallmark), watering, red eyes, seasonal pattern or perennial. No discharge or just mild watery. Associated with sneezing, nasal discharge.
Rx (mild):
Sodium Cromoglicate 2% eye drops - 1 drop QID (mast cell stabilizer)
OR
Olopatadine 0.1% eye drops - 1 drop BD (dual action - antihistamine + mast cell)
OR
Ketotifen 0.025% eye drops - 1 drop BD
Artificial tears PRN for lubrication
Cold compresses for symptomatic relief
If moderate-severe:
Olopatadine 0.1% eye drops BD
+
Oral antihistamine:
Cetirizine 10 mg OD OR Loratadine 10 mg OD (non-sedating)
(Diphenhydramine/Chlorpheniramine if night itching is dominant - sedating)
Avoid topical steroids unless instructed by senior. Mast cell stabilizers take a few days to work - tell the patient this.
From Kanski's Clinical Ophthalmology 10th ed.: Dual action antihistamine and mast cell stabilizers (olopatadine, ketotifen, azelastine) "act rapidly and are often very effective for exacerbations."
4. VERNAL KERATOCONJUNCTIVITIS (VKC)
Presentation: Young boys, severe itching, cobblestone papillae on upper tarsal conjunctiva, shield ulcer possible, seasonal. Common in South Asia.
Rx (initiation - mild case):
Olopatadine 0.1% eye drops BD
+
Sodium Cromoglicate 2% eye drops QID
+
Lubricating drops QID
Moderate/severe VKC (steroids, cyclosporine) - refer senior.
5. DRY EYE / KERATOCONJUNCTIVITIS SICCA
Presentation: Burning, grittiness, foreign body sensation, worse in the evening or in AC/windy environments. Paradoxically may have watering (reflex tearing).
Rx:
Carboxymethylcellulose (CMC) 0.5% eye drops - 1 drop TID-QID PRN
OR
HPMC 0.3% eye drops QID
OR (preservative-free preferred for long-term)
Sodium Hyaluronate 0.1-0.2% eye drops - 1 drop TID-QID
Carbomer gel (Viscotears) at night for prolonged lubrication
- Counsel: blink exercises, avoid AC/fans blowing directly, screen breaks (20-20-20 rule)
- Omega-3 supplements can help long-term
6. BLEPHARITIS (Lid Margin Disease)
Presentation: Crusting at lid margins, morning stickiness, burning, dandruff-like flakes on lashes. Chronic, bilateral.
Rx:
Lid hygiene (MOST IMPORTANT):
Warm compress to closed eyes × 5-10 min BD
Lid scrub with diluted baby shampoo or commercial lid wipes BD
Chloramphenicol 1% ointment applied to lid margins at night × 2-4 weeks
OR
Tobramycin ointment at lid margin at night
If Meibomian gland dysfunction:
Doxycycline 100 mg OD × 6-12 weeks (adults, anti-inflammatory dose)
7. SUBCONJUNCTIVAL HAEMORRHAGE
Presentation: Bright red patch on white of eye, no pain, no vision change. Alarming to patient but benign.
No treatment needed. Reassure the patient. Resolves in 1-2 weeks.
Artificial tears QID (for comfort if any irritation)
- Check BP if spontaneous and recurrent
- If associated with trauma or vision change → refer
8. CORNEAL ABRASION
Presentation: History of foreign body / finger poke / contact lens, acute pain, photophobia, excessive tearing. Fluorescein staining positive.
Rx:
Tobramycin 0.3% eye drops - 1 drop QID × 3-5 days
OR
Chloramphenicol 0.5% eye drops QID × 3-5 days
Homatropine 2% eye drops - 1 drop BD (cycloplegic for ciliary spasm pain)
OR
Cyclopentolate 1% for larger abrasions
Lubricating drops/ointment at night
- Do NOT patch the eye - can mask worsening infection
- Do NOT give topical steroids - absolutely contraindicated with epithelial defect
- Review in 24-48 hours
- If dendritic ulcer seen → Acyclovir 3% ointment 5×/day (herpetic)
From Rosen's Emergency Medicine: "Prophylactic topical antibiotics are not indicated for corneal abrasions, and eye patches are not recommended because they can mask a worsening infection."
9. STYE (External Hordeolum) and CHALAZION
Presentations:
- Stye = acute, painful, red swelling at lid margin (infected lash follicle)
- Chalazion = chronic, non-tender, firm nodule in lid (blocked Meibomian gland)
Rx for Stye:
Warm compress × 5-10 min, 3-4 times/day (to bring to a head)
Chloramphenicol 1% ointment applied to lid margin TID × 5-7 days
Oral antibiotic only if spreading cellulitis:
Amoxicillin-Clavulanate 625 mg BD × 5 days
Rx for Chalazion:
Warm compress BD-TID (most resolve spontaneously over weeks-months)
Lid massage after compresses
If persistent > 6 weeks: refer for incision and curettage (I&C)
10. ACUTE ANGLE-CLOSURE GLAUCOMA
Presentation: Sudden severe headache + eye pain, blurred vision with halos, nausea/vomiting, fixed mid-dilated pupil, rock-hard eye, corneal haze.
⛔ THIS IS AN EMERGENCY. CALL SENIOR IMMEDIATELY.
While waiting:
Tab Acetazolamide 500 mg STAT (oral if able to take)
Timolol 0.5% eye drops - 1 drop
Pilocarpine 2% eye drops - 1 drop (after IOP starts to fall)
Do not give any mydriatic (tropicamide, atropine) - will worsen the attack.
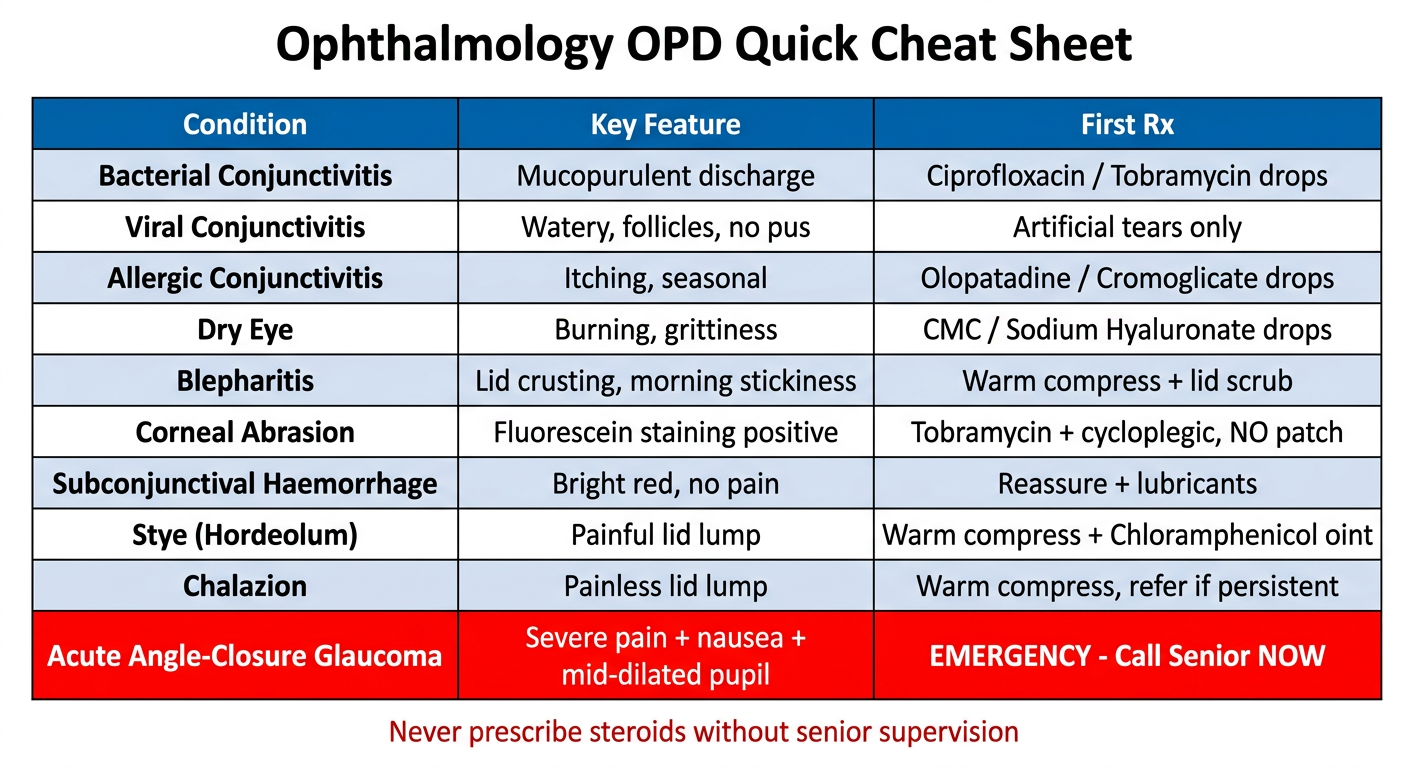
QUICK CHEAT SHEET
| Condition | Key Feature | First Rx |
|---|
| Bacterial conjunctivitis | Mucopurulent discharge | Ciprofloxacin / Tobramycin drops |
| Viral conjunctivitis | Watery, follicles, no pus | Artificial tears only |
| Allergic conjunctivitis | Itching, seasonal | Olopatadine / Cromoglicate drops |
| Dry eye | Burning, grittiness | CMC / Sodium hyaluronate drops |
| Blepharitis | Lid crusting, morning stickiness | Warm compress + lid scrub |
| Corneal abrasion | Fluorescein staining | Tobramycin + cycloplegic, NO patch |
| Subconj haemorrhage | Bright red, no pain | Reassure + lubricants |
| Stye | Painful lid lump | Warm compress + chloramphenicol oint |
| Chalazion | Painless lid lump | Warm compress, refer if persistent |
| Acute glaucoma | Severe pain + nausea + mid-dilated pupil | EMERGENCY - call senior |
GENERAL TIPS FOR WRITING OPHTHA PRESCRIPTIONS
- Always write "in affected eye(s)" or "in the right/left eye" - not just "eye drops."
- Wash hands before instilling drops - counsel every patient.
- Wait 5 minutes between two different drops if prescribing multiple drops.
- Suspensions need to be shaken before use (e.g., prednisolone acetate).
- Ointments go after drops and are typically prescribed at bedtime.
- Never give steroids without senior supervision unless you're confident there's no corneal ulcer / herpes.
- Topical NSAIDs (e.g., Ketorolac 0.5%, Diclofenac 0.1%) are useful for pain in corneal abrasion and post-op.
You've got this. For anything with vision loss, severe pain, trauma, or that just doesn't fit the simple patterns above, call your senior without hesitation. That's the right call every time.
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. | Rosen's Emergency Medicine | Textbook of Family Medicine 9e