
IMG_0681.jpg
Answering 2nd question
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Kanski's. Let me compile a thorough, exam-ready answer.
Question 2 - Ophthalmology Case: 65-year-old male, bilateral painless progressive diminution of vision, lenticular opacities, normal fundus
Diagnosis: Bilateral Senile (Age-related) Cataract
Part (a) - Differential Diagnoses of Gradually Progressive, Painless Diminution of Vision in an Elderly Patient (3 marks)
The key differentials are classified by the anatomical site of the problem:
Lens (Lenticular causes)
- Senile/Age-related cataract (most likely here - lenticular opacities confirmed)
- Nuclear sclerosis, cortical, posterior subcapsular
- Diabetic cataract - snowflake cortical opacities; age-related cataract also occurs earlier in diabetics
Retinal causes
- Age-related macular degeneration (AMD) - dry or wet; central vision loss
- Diabetic retinopathy with macular oedema - bilateral, gradual
- Central retinal artery occlusion / vein occlusion (usually acute, but chronic changes can cause gradual loss)
- Retinitis pigmentosa - peripheral field loss + night blindness, can present in elderly
Glaucoma
- Chronic open-angle glaucoma - slow, painless peripheral field loss; often asymptomatic until late
Optic nerve / Neurological
- Optic atrophy (secondary to glaucoma, vascular, compressive) - afferent pupil defect, pallor
Corneal causes
- Corneal degeneration / dystrophy (e.g., Fuchs' endothelial dystrophy, band keratopathy)
Vitreous
- Vitreous haemorrhage or degeneration (though usually more acute)
In this case: The slit-lamp finding of lenticular opacities and a normal dilated fundus in both eyes points strongly to bilateral senile cataract as the diagnosis, excluding retinal and optic nerve causes.
Part (b) - Clinical Evaluation and Preoperative Investigations Before Cataract Surgery (6 marks)
Clinical Evaluation
History
- Duration and rate of progression of visual loss
- Occupation and visual requirements of the patient
- Symptoms: glare, halos, monocular diplopia, difficulty reading or driving (especially night driving)
- History of trauma, corticosteroid use, diabetes, uveitis
- Current medications - especially systemic alpha-blockers (tamsulosin) which cause intraoperative floppy iris syndrome (IFIS)
- Anticoagulant or antiplatelet use
Visual Function Assessment
- Best-corrected visual acuity (BCVA) - Snellen chart
- Contrast sensitivity and glare testing
- Potential acuity testing (to assess whether retinal function is adequate for surgery to be worthwhile)
Slit-Lamp Examination
- Type of cataract: nuclear sclerosis, cortical, posterior subcapsular, or combined
- Maturity: immature, mature, hypermature (Morgagnian)
- Anterior segment: corneal clarity, depth of anterior chamber, condition of iris
- Status of posterior capsule
Dilated Fundus Examination
- Macula: exclude AMD, diabetic macular oedema
- Optic disc: exclude glaucoma
- Peripheral retina: exclude lattice degeneration, tears (especially if myopic)
Other Examinations
- Intraocular pressure (IOP) measurement - baseline and to exclude glaucoma
- Keratometry and axial length measurement (biometry) for IOL power calculation (A-scan ultrasonography or optical biometry)
- Corneal endothelial count (specular microscopy) if Fuchs' dystrophy is suspected or repeat surgery
Preoperative Investigations
| Investigation | Purpose |
|---|---|
| Biometry (A-scan / optical, e.g. IOLMaster) | IOL power calculation |
| Keratometry | Corneal curvature for IOL calculation; to plan toric IOL if astigmatism >1D |
| Specular microscopy | Endothelial cell count if corneal disease suspected |
| Blood glucose / HbA1c | Diabetic patients (diabetic macular oedema worsens postoperatively) |
| Blood pressure | Hypertension management perioperatively |
| Urea and electrolytes, full blood count, ECG | Only if general anaesthesia is planned |
| Coagulation profile / INR | If on anticoagulants; managed per local protocol |
| Fundus fluorescein angiography (FFA) / OCT | If macular disease suspected before surgery |
Per Kanski's: "Routine preoperative general medical examination, blood tests and ECG are not usually required for local anaesthesia." Investigations are targeted based on systemic history.
Part (c) - Management of Senile Cataract: Preferred Surgical Procedure and Postoperative Care (6 marks)
Indications for Surgery
- Visual: Opacity causing difficulty with daily activities (the most common indication); patient-reported functional impairment
- Medical: Phacolytic glaucoma, phacomorphic glaucoma, to allow fundus monitoring for diabetic retinopathy
Preferred Surgical Procedure: Phacoemulsification with IOL Implantation
This is the gold standard for cataract surgery worldwide.
Steps of Phacoemulsification
- Corneal incision: A small self-sealing clear corneal tunnel incision (~2.2-2.8 mm)
- Continuous curvilinear capsulorhexis (CCC): Circular tear of the anterior capsule (~5-6 mm)
- Hydrodissection and hydrodelineation: Fluid injection to separate nucleus from capsule
- Phacoemulsification: Ultrasonic probe emulsifies and aspirates the lens nucleus using sculpting and cracking techniques (divide and conquer, stop and chop, etc.)
- Irrigation-aspiration (I/A): Removes residual cortical material
- IOL implantation: A foldable acrylic IOL is inserted into the capsular bag through the same small incision
- Wound hydration: The self-sealing incision is hydrated; sutures rarely needed
Advantages of Phacoemulsification
- Small incision (sutureless) → less surgically induced astigmatism
- Rapid visual recovery (often the next day)
- Low complication rate
- Can be done under topical or local anaesthesia as a day-case procedure
Alternative: MSICS (Manual Small Incision Cataract Surgery)
- Used in resource-limited settings (developing countries)
- Comparable visual outcomes to phacoemulsification
- Faster and cheaper, does not require expensive technology
- Suitable for dense/hard cataracts
IOL Selection
- Monofocal IOL (standard): Set for distance vision; patient needs reading glasses
- Multifocal/bifocal IOL: Reduces need for spectacles at all distances; higher rate of dysphotopsia
- Toric IOL: Corrects pre-existing corneal astigmatism
- Square-edged optic: Reduces posterior capsule opacification (PCO)
- Power calculated using biometry (SRK-T or Haigis formula)
Anaesthesia
- Usually topical anaesthesia (drops) or peribulbar/sub-Tenon's local anaesthesia
- General anaesthesia for very anxious, uncooperative, or paediatric patients
Postoperative Care
Immediate Postoperative (Day 0-1)
- Eye shield/pad applied to protect the eye
- Patient instructed to avoid rubbing the eye
- Snellen VA checked at first postoperative visit (usually day 1)
- Corneal clarity, IOP, and anterior chamber checked at slit lamp
Medications (typical regime)
- Topical antibiotic eye drops (e.g., moxifloxacin or chloramphenicol) - for 1-4 weeks to prevent endophthalmitis
- Topical corticosteroid (e.g., prednisolone acetate 1%) - to reduce postoperative inflammation; tapered over 4-6 weeks
- Topical NSAID (e.g., ketorolac or diclofenac) - reduces cystoid macular oedema (CMO)
- IOP-lowering drops if pressure elevated
Activity Restrictions
- No swimming, heavy lifting, or straining for 2-4 weeks
- Avoid rubbing the eye
- Night-time eye shield for 1 week
Follow-up Schedule
- Day 1, Week 1, Week 4-6 post-surgery
- Refraction and spectacle prescription at 4-6 weeks (when the eye has stabilized)
Complications to Watch For
- Posterior capsule opacification (PCO): Most common late complication; treated with Nd:YAG laser capsulotomy
- Cystoid macular oedema (CMO): Most common cause of reduced vision postoperatively
- Endophthalmitis: Rare but vision-threatening; presents with pain, hypopyon, reduced vision
- Corneal oedema (bullous keratopathy if endothelium damaged)
- Posterior capsule rupture with vitreous loss (intraoperative complication)
- IOL-related: Decentration, dysphotopsia
- Elevated IOP (steroid response or retained viscoelastic)
Summary Table
| Aspect | Key Point |
|---|---|
| Diagnosis | Bilateral senile cataract (lenticular opacities, normal fundus) |
| Preferred surgery | Phacoemulsification + foldable acrylic IOL implantation |
| Biometry | Essential preoperative step for IOL power calculation |
| Anaesthesia | Topical or local (peribulbar) |
| Postop drops | Antibiotic + steroid + NSAID |
| Most common late complication | PCO (treated with Nd:YAG laser) |
References: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition - Chapter 10: Lens; Goldman-Cecil Medicine
Moorens ulcer ophthalmology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, exam-ready short note on Mooren's ulcer.
Mooren's Ulcer
Definition
Mooren's ulcer is a rare, chronic, painful, progressive peripheral ulcerative keratitis (PUK) of autoimmune etiology, characterized by circumferential stromal ulceration of the peripheral cornea with later central spread, in the absence of scleritis or systemic disease. It is a diagnosis of exclusion.
Etiology and Pathogenesis
- Autoimmune mechanism: The leading theory is a host immune reaction against calgranulin C, a normally hidden antigen in corneal keratocytes, possibly unmasked by prior corneal insult (infection or surgery)
- Precipitating factors: Prior corneal surgery, infections (notably Hepatitis C virus - associated with Mooren-like ulcer)
- T-cell mediated stromal destruction with upregulation of matrix metalloproteinases (collagenases) leads to progressive corneal melting
- No infection is causative; it is sterile inflammation
Clinical Types
| Feature | Type 1 (Benign) | Type 2 (Aggressive) |
|---|---|---|
| Age | Older patients | Younger patients |
| Laterality | Usually unilateral | Often bilateral |
| Severity | Mild-moderate | Severe, painful |
| Geography | Western countries | South Asia, Africa |
| Response | Good to topical therapy | Needs systemic immunosuppression |
| Prognosis | Better | Poorer |
Clinical Features
Symptoms
- Severe, unrelenting pain - characteristic and often the dominant complaint
- Photophobia
- Lacrimation
- Blurred vision (due to corneal involvement)
- No systemic symptoms (distinguishes from systemic PUK)
Signs (Slit-Lamp)
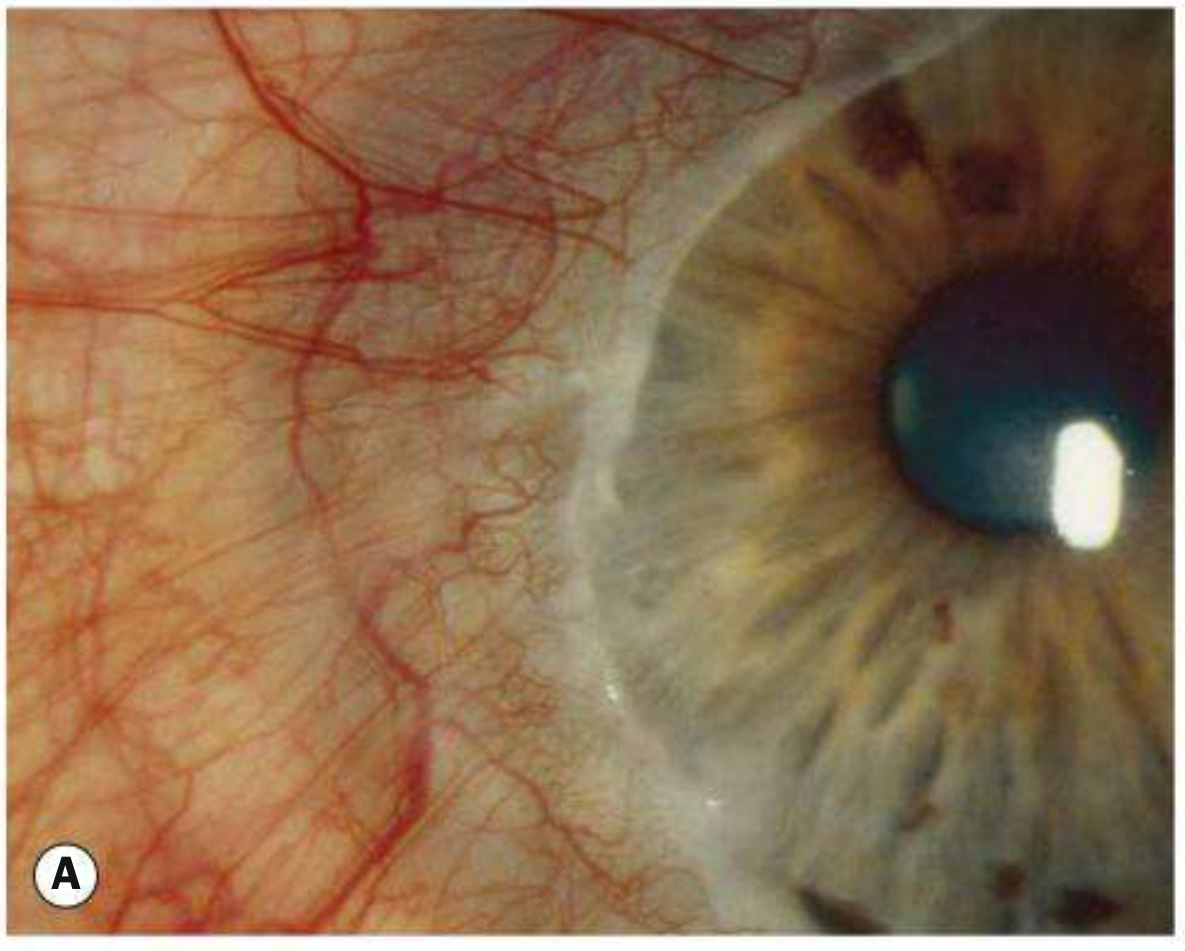
- Peripheral ulceration - starts nasally or temporally, involves the superficial one-third of the stroma, with variable epithelial loss
- Undermined and infiltrated leading (central) edge - pathognomonic feature; the edge overhangs the bed of the ulcer
- Circumferential spread - progresses along the limbus, then centrally
- No clear zone between ulcer and limbus - the ulcer always involves the limbus (unlike marginal keratitis which has a lucid interval)
- Vascularization - limbal vessels grow into the bed of the ulcer up to its leading edge but not beyond
- Limbitis present; scleritis absent (key differentiating feature from systemic PUK)
- Iritis may be present
- Healing stage: thinning, vascularization, and scarring of the involved area
Differentials (Peripheral Corneal Ulcers)
| Condition | Key Distinguishing Features |
|---|---|
| PUK (systemic - RA, GPA, SLE) | Associated scleritis, systemic connective tissue disease |
| Marginal keratitis (staphylococcal hypersensitivity) | Clear zone between ulcer and limbus, responds to steroids + antibiotic |
| Terrien's marginal degeneration | Painless, non-inflammatory, superior, intact epithelium, lipid line |
| Pellucid marginal degeneration | Painless, inferior thinning, no inflammation |
| Bacterial/fungal ulcer | Infective signs, culture positive |
| Furrow degeneration | Painless, adjacent to arcus senilis, elderly |
Key rule: "Peripheral ulcerative keratitis is caused by infection until proven otherwise. In the absence of infection, investigate for systemic autoimmune disease." - Kanski's
Investigations
Mooren's ulcer is a diagnosis of exclusion. Workup to rule out:
- Corneal scraping - Gram stain, KOH mount, culture (to exclude infection)
- Blood investigations: ANA, anti-dsDNA, ANCA (c-ANCA/p-ANCA), RF, anti-CCP (to exclude systemic autoimmune disease)
- Hepatitis B and C serology (Mooren-like ulcers associated with HCV)
- Chest X-ray (GPA/sarcoidosis)
- Syphilis serology (VDRL/TPHA)
- FBC, ESR, CRP
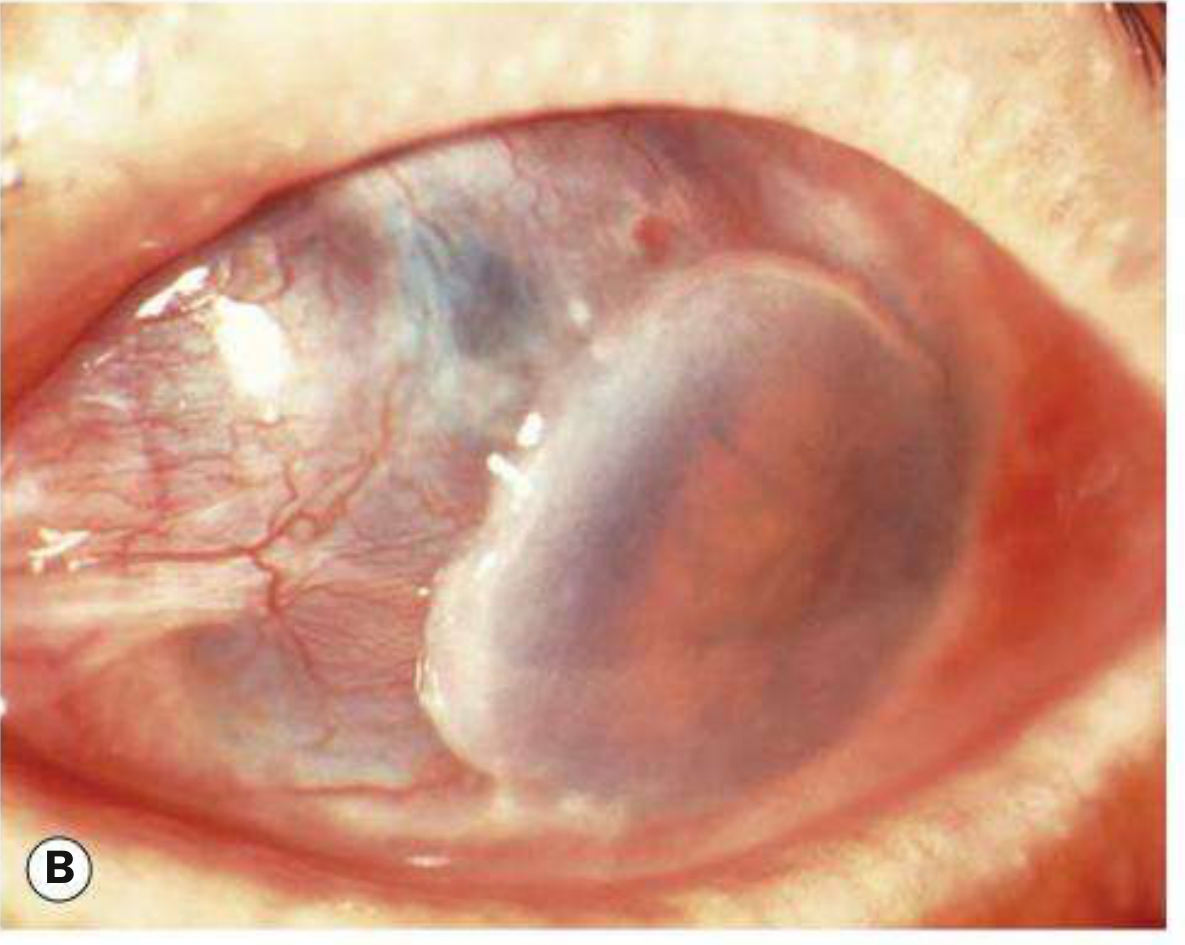
Complications
- Severe irregular astigmatism (from corneal thinning and scarring)
- Corneal perforation - particularly after minor trauma; spontaneous perforation is rare
- Secondary bacterial infection
- Cataract and glaucoma (secondary)
- Corneal scarring with permanent visual loss
Treatment
Treatment follows a step-ladder approach based on severity.
Step 1 - Topical Medical Therapy (first line)
- Topical corticosteroids (e.g., prednisolone acetate 1%) - as frequently as hourly in active disease, then slowly tapered over several months
- Prophylactic topical antibiotic (low-frequency, to prevent secondary infection)
- Artificial tears (lubricants) - adjunctive, reduce desiccation
- Collagenase inhibitors - topical acetylcysteine 10-20% to inhibit stromal melting
- Topical ciclosporin (up to 2%) - takes weeks to act; used in resistant cases
- Tacrolimus 0.1% ointment - effective in refractory cases
Step 2 - Surgical (if no response to topical steroids)
- Conjunctival resection - excision of the perilimbal conjunctiva to remove the immune effector tissue driving corneal destruction
- Excision extends 4 mm back from the limbus and 2 mm beyond the circumferential margins of the ulcer
- May be combined with excision of necrotic tissue
- Keratoepithelioplasty: suturing of a donor corneal lenticule onto the scleral bed to act as a physical barrier against conjunctival regrowth and further melting
- Topical steroids continued postoperatively
Step 3 - Systemic Immunosuppression (bilateral/advanced/refractory disease)
- Systemic corticosteroids (prednisolone) - for rapid effect
- Methotrexate, azathioprine, mycophenolate - steroid-sparing agents
- Cyclophosphamide - for very severe cases
- Biological agents: Rituximab (anti-CD20) - shows promise in refractory cases
- Systemic doxycycline - acts as a systemic collagenase inhibitor
Step 4 - Management of Complications
- Lamellar keratectomy - in advanced disease with a "central island" of cornea; removes the inflammatory stimulus
- Corneal perforation: Tissue adhesive (cyanoacrylate glue), bandage contact lens, or penetrating keratoplasty (with immunosuppressive cover)
- Visual rehabilitation: Keratoplasty considered once inflammation has fully settled; systemic immunosuppression cover is required
Key Exam Points Summary
| Feature | Mooren's Ulcer |
|---|---|
| Type | Sterile peripheral ulcerative keratitis |
| Pathognomonic sign | Undermined, infiltrated central (leading) edge |
| Limbus involvement | Always involved; no clear zone |
| Scleritis | Absent (key negative feature) |
| Systemic association | None (diagnosis of exclusion) |
| Bilateral form | More aggressive, younger patients, South Asians |
| First-line treatment | Topical steroids (hourly) + antibiotic |
| Surgical treatment | Conjunctival resection |
| Systemic treatment | Steroids, immunosuppressants, Rituximab |
| HCV association | Mooren-like ulcer |
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition; Wills Eye Manual
Orbital cellulitis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, multi-source content. Here is the complete short note.
Orbital Cellulitis
Definition
Orbital cellulitis (postseptal cellulitis) is a serious, sight- and life-threatening infection of the soft tissues posterior to the orbital septum. It must be distinguished from preseptal (periorbital) cellulitis, which is infection anterior to the orbital septum and carries a far lower risk.
Orbital Septum - Key Anatomical Landmark
The orbital septum is a fibrous membrane extending from the orbital rims to the eyelid margins. It is the critical barrier:
- Preseptal cellulitis = infection anterior to septum (periorbital) - less dangerous
- Orbital cellulitis = infection posterior to septum - dangerous, requires hospitalization
Etiology and Sources of Infection
| Source | Details |
|---|---|
| Paranasal sinusitis | Most common (90%); especially ethmoid sinusitis (via thin lamina papyracea) |
| Preseptal cellulitis | Direct posterior spread |
| Dacryocystitis / dacryoadenitis | Via contiguous spread |
| Midfacial skin or dental abscess | Dental infections tend to be aggressive and may spread to cavernous sinus |
| Orbital trauma | Fractures, penetrating injury, intraorbital foreign body |
| Ocular surgery | Post-surgical seeding |
| Hematogenous spread | From distant infection (bacteremia) |
| Cavernous sinus thrombosis | Can spread retrogradely |
Causative Organisms
| Population | Organisms |
|---|---|
| Adults (most common) | Staphylococcus aureus, Streptococcus pneumoniae, Streptococcus pyogenes, anaerobes (Bacteroides) |
| Children | Haemophilus influenzae (rare in vaccinated children), S. aureus, S. pneumoniae |
| Post-trauma | Gram-negative rods |
| Dental abscess | Mixed aerobes and anaerobes |
| Immunocompromised / diabetics | Fungi - Mucormycosis (Zygomycosis), Aspergillus |
| Hospital-associated | MRSA |
Note: Mucormycosis in diabetic or immunocompromised patients is rapidly progressive and life-threatening - always look for black eschar in nasal passages.
Clinical Features
Symptoms
- Rapid onset of periorbital pain, worsened by eye movement
- Swelling and redness of the eyelids
- Malaise, fever, headache
- Blurred vision and diplopia (double vision)
- Recent history of nasal congestion, sinusitis, or upper respiratory infection
- Tooth pain (if dental source)
Signs

- Pyrexia - often marked
- Eyelid signs: Tender, firm, warm, erythematous, edematous eyelids; periocular swelling
- Conjunctival chemosis and injection, sometimes subconjunctival hemorrhage
- Proptosis (exophthalmos) - may be non-axial (dystopia) if an abscess is present; may be obscured by lid swelling
- Painful ophthalmoplegia - restricted, painful extraocular movements (hallmark distinguishing from preseptal)
- Reduced visual acuity and dyschromatopsia (impaired color vision) - indicate optic nerve compression
- Relative afferent pupillary defect (RAPD) - in severe cases; indicates optic neuropathy
- Fundus: Choroidal folds, optic disc swelling, retinal venous congestion
- Signs are usually unilateral, though edema may spread to the contralateral eyelid
Preseptal vs. Orbital Cellulitis - Key Differences
| Feature | Preseptal (Periorbital) | Orbital (Postseptal) |
|---|---|---|
| Septum | Anterior | Posterior |
| Proptosis | Absent | Present |
| Ophthalmoplegia | Absent | Present (painful) |
| Visual acuity | Normal | May be reduced |
| Pupillary reaction | Normal | May show RAPD |
| Pain on eye movement | Absent | Present |
| Fever | May be mild | Usually marked |
| Risk | Low | High - sight and life threatening |
| Management | Oral antibiotics (mild cases) | Hospital admission + IV antibiotics |
Investigations
Imaging (Most Important)
- CT scan of orbits, paranasal sinuses, and brain with contrast - investigation of choice
- Confirms postseptal location of infection
- Identifies sinusitis (typically ethmoiditis)
- Detects subperiosteal abscess (most common along medial orbital wall)
- Detects orbital abscess, intracranial extension
- Excludes retained foreign body

- MRI - sometimes performed; better for intracranial complications (brain abscess, meningitis, cavernous sinus thrombosis)
Laboratory
- White cell count (WBC) with differential - leukocytosis
- Blood cultures - to identify bacteremia and guide antibiotic therapy
- Culture of nasal discharge
- Gram stain and culture of any wound discharge
- Lumbar puncture if meningeal/cerebral signs develop
Other
- Tetanus immunization status (in trauma cases)
- Blood glucose (to assess for diabetes/mucormycosis risk)
- Check nasal passages for black eschar in immunocompromised/diabetic patients (mucormycosis)
Complications
Ocular Complications
- Optic neuropathy - from direct compression or ischemia; can lead to permanent blindness
- Exposure keratopathy - from proptosis and chemosis
- Raised intraocular pressure (IOP)
- Endophthalmitis
- Central retinal artery or vein occlusion
Orbital Complications
- Subperiosteal abscess - most commonly along the medial orbital wall (adjacent to ethmoid sinuses)
- Orbital abscess
Intracranial Complications (uncommon - 3-4% - but extremely serious)
- Cavernous sinus thrombosis - suggested by CN III, IV, VI palsies + bilateral eye signs + high fever
- Meningitis
- Brain abscess
- Subdural empyema, epidural abscess
- Frontal bone osteomyelitis
Management
1. Immediate Steps
- Hospital admission is mandatory
- Urgent ophthalmology consultation
- Otorhinolaryngology (ENT) assessment for sinus disease
- Paediatric/Infectious disease specialist consultation (especially in children)
- Mark extent of periorbital erythema with a surgical marker to monitor progress
- Optic nerve function monitored at least every 4 hours (VA, color vision, light brightness appreciation, pupillary reactions)
2. Medical Treatment - IV Antibiotics (First Line)
Broad-spectrum IV antibiotics to cover Gram-positive, Gram-negative, and anaerobic organisms:
| Regimen | Details |
|---|---|
| Ampicillin-sulbactam | 3 g IV q6h (adults); first choice for community-acquired |
| Piperacillin-tazobactam | 4.5 g IV q8h (adults) |
| Ceftazidime + Metronidazole | Typical choice (Kanski's); ceftazidime covers Gram-negatives, metronidazole covers anaerobes |
| Vancomycin | Added if MRSA is suspected or meningitis is possible; 15-20 mg/kg q8-12h |
| Ceftriaxone + Metronidazole | Penicillin-allergic patients (with vancomycin) |
| Moxifloxacin/Ciprofloxacin + Metronidazole | Penicillin + cephalosporin allergic patients |
- IV antibiotics continued until apyrexial for 4 days, then switched to oral antibiotics for 1-3 weeks
- Add nasal decongestant spray (e.g., oxymetazoline) for up to 3 days
- Nasal corticosteroid spray to aid resolution of sinusitis
- Lubricant eye ointment (erythromycin/bacitracin) for corneal exposure from chemosis
3. Surgical Treatment
Indications for surgery:
- Presence of orbital abscess (requires drainage and debridement)
- No response to 48-72 hours of IV antibiotics
- Very severe sinus disease (sinus drainage by ENT)
- Rising IOP or worsening optic neuropathy despite antibiotics
Surgical options:
- Drainage of subperiosteal or orbital abscess - surgical or endoscopic (transnasal endoscopic drainage preferred for medial subperiosteal abscess in children)
- Drainage of infected paranasal sinuses (functional endoscopic sinus surgery - FESS)
- Lateral canthotomy and cantholysis - emergency procedure for severely elevated IOP or acute optic nerve compression; decompresses the orbit by releasing the lateral canthal tendon
- Biopsy of inflammatory tissue in atypical presentations
Chandler Classification of Orbital Complications of Sinusitis
A classical staging system frequently asked in exams:
| Stage | Name | Features |
|---|---|---|
| I | Inflammatory edema (Preseptal) | Eyelid edema, no proptosis, no ophthalmoplegia |
| II | Orbital cellulitis | Edema of orbital fat; mild proptosis; mild ophthalmoplegia |
| III | Subperiosteal abscess | Pus between periorbita and orbital wall; proptosis, ophthalmoplegia |
| IV | Orbital abscess | Pus within orbital fat; marked proptosis, complete ophthalmoplegia, visual loss |
| V | Cavernous sinus thrombosis | Bilateral eye signs, high fever, meningism, CN III/IV/VI palsies |
Key Exam Points Summary
| Feature | Key Point |
|---|---|
| Definition | Infection posterior to orbital septum |
| Most common source | Ethmoid sinusitis (via lamina papyracea) |
| Hallmark signs | Proptosis + painful ophthalmoplegia + fever |
| Differentiates from preseptal | Proptosis and restricted eye movement |
| Investigation of choice | Contrast CT of orbit + sinuses + brain |
| Most dangerous complication | Cavernous sinus thrombosis |
| Most common abscess location | Medial orbital wall (subperiosteal) |
| Treatment | IV antibiotics + hospital admission |
| Emergency surgery indication | Orbital abscess, rising IOP, worsening vision |
| Mucormycosis alert | Diabetics/immunocompromised; black nasal eschar |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition; Wills Eye Manual; Tintinalli's Emergency Medicine
Dry eye disease according to A K Khurana ophthalmology textbook
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Important note: A K Khurana's Comprehensive Ophthalmology is not available in the library. The answer below is compiled from Kanski's Clinical Ophthalmology (10th ed.) and the Wills Eye Manual - both are authoritative references covering the same content as Khurana. The structure, classification, tests, and management follow the standard Khurana syllabus closely.
Dry Eye Disease (Keratoconjunctivitis Sicca - KCS)
Definition
Dry eye disease (DED) is a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film, accompanied by ocular symptoms, in which tear film instability, hyperosmolarity, ocular surface inflammation and damage, and neurosensory abnormalities play etiological roles.
(2017 TFOS DEWS II definition)
The Tear Film - Normal Structure
The normal tear film has three layers (from outside in):
| Layer | Produced by | Function |
|---|---|---|
| Lipid (outer) | Meibomian glands, glands of Zeis/Moll | Retards evaporation; stabilizes tear film |
| Aqueous (middle) | Main lacrimal gland, accessory lacrimal glands (Krause, Wolfring) | Oxygen supply to cornea; antibacterial (lysozyme, lactoferrin, IgA); washes debris |
| Mucin (inner) | Conjunctival goblet cells, corneal/conjunctival epithelium | Wets the hydrophobic corneal epithelium; anchors tear film |
Normal tear film break-up time (TBUT): >10 seconds
Etiology and Classification
The 2007 International Dry Eye Workshop (DEWS) classification - the most widely used:
A. Aqueous-Deficient Dry Eye (ADDE)
1. Sjögren Syndrome (SS) Dry Eye
- Primary SS: Dry eyes + dry mouth + parotid enlargement (sicca complex), without associated autoimmune disease
- Secondary SS: As above, associated with rheumatoid arthritis, SLE, or other connective tissue diseases
- Mechanism: Lymphocytic infiltration of lacrimal and salivary glands
2. Non-Sjögren Syndrome Dry Eye
- Lacrimal gland deficiency:
- Primary: Age-related dry eye (most common), congenital alacrima, familial dysautonomia (Riley-Day syndrome)
- Secondary: Lacrimal gland infiltration (sarcoidosis, lymphoma, AIDS), graft-versus-host disease, lacrimal gland ablation
- Lacrimal gland duct obstruction: Trachoma, cicatricial pemphigoid, chemical injuries, Stevens-Johnson syndrome
- Reflex hyposecretion:
- Sensory block: contact lens wear, diabetes mellitus, refractive surgery (LASIK), neurotrophic keratitis
- Motor block: VII cranial nerve palsy, systemic anticholinergic drugs
B. Evaporative Dry Eye (EDE) - More Common
Intrinsic causes
- Meibomian gland dysfunction (MGD) - most common cause overall; posterior blepharitis, rosacea
- Disorders of lid aperture: Lagophthalmos, lid retraction, proptosis (exposure keratopathy), facial nerve palsy
- Low blink rate: Parkinson's disease, prolonged computer/reading/television use
- Drug action: Antihistamines, beta-blockers, antispasmodics, diuretics
Extrinsic causes
- Vitamin A deficiency (goblet cell loss → mucin deficiency)
- Topical drugs and preservatives (BAK - benzalkonium chloride toxicity)
- Contact lens wear
- Ocular surface diseases: allergic conjunctivitis, trachoma
Key pathophysiologic mechanism: Four core inter-related mechanisms - tear instability → hyperosmolarity → inflammation → ocular surface damage - form a vicious cycle. Inflammation (present in 80% of patients) is both a cause and consequence of dry eye.
Symptoms
- Burning and stinging sensation
- Grittiness / foreign body sensation
- Dryness
- Excess reflex tearing (paradoxical - due to irritation)
- Blurred or fluctuating vision (clears transiently with blinking)
- Stringy or ropy mucous discharge
- Photophobia
- Redness
- Crusting of lids on waking
Aggravating factors (increase evaporation or reduce blink rate):
- Wind, air-conditioning, central heating, low humidity
- Smoke, dust, allergens
- Prolonged reading, computer use, television (reduce blink rate)
- Symptoms characteristically worsen over the course of the day (aqueous deficient) or may be worse in the morning (evaporative/MGD)
Note: "Symptoms are often out of proportion to clinical signs" - Wills Eye Manual
Clinical Signs
Eyelids
- Posterior (seborrhoeic) blepharitis with meibomian gland dysfunction - oil globules at gland orifices, inflamed gland margins
- Reduced blink rate; incomplete blink
- Lid margin irregularities
Tear Film
- Reduced or absent tear meniscus at inferior lid margin
- Normal height: ≥0.5 mm, convex shape
- Dry eye: Scanty, concave, or absent meniscus
- Excess debris or mucus in tear film
- Foam or froth at lid margins (MGD)
Conjunctiva
- Redness (injection)
- Rose Bengal staining - stains devitalized/dead epithelial cells (interpalpebral pattern)
- Lissamine green staining - similar to rose Bengal but better tolerated
- Conjunctivochalasis (redundant bulbar conjunctival folds)
- Keratinization (in severe/chronic disease)
Cornea
- Punctate epithelial erosions (PEE) - in the interpalpebral zone (inferior cornea), stained with fluorescein
- Mucous filaments (filamentary keratitis) - in severe cases
- Reduced corneal sensation (in severe/long-standing disease)
Investigations / Diagnostic Tests
1. Tear Film Break-Up Time (TBUT) - Most Important
- Fluorescein dye instilled; patient blinks, then keeps eyes open
- Time measured from last blink to first random dry spot appearing in the tear film
- Normal: >10 seconds
- Abnormal (dry eye): <10 seconds
- Non-invasive TBUT (NIBUT) can be measured with topographer or keratometer
2. Schirmer's Test - Measures Aqueous Secretion
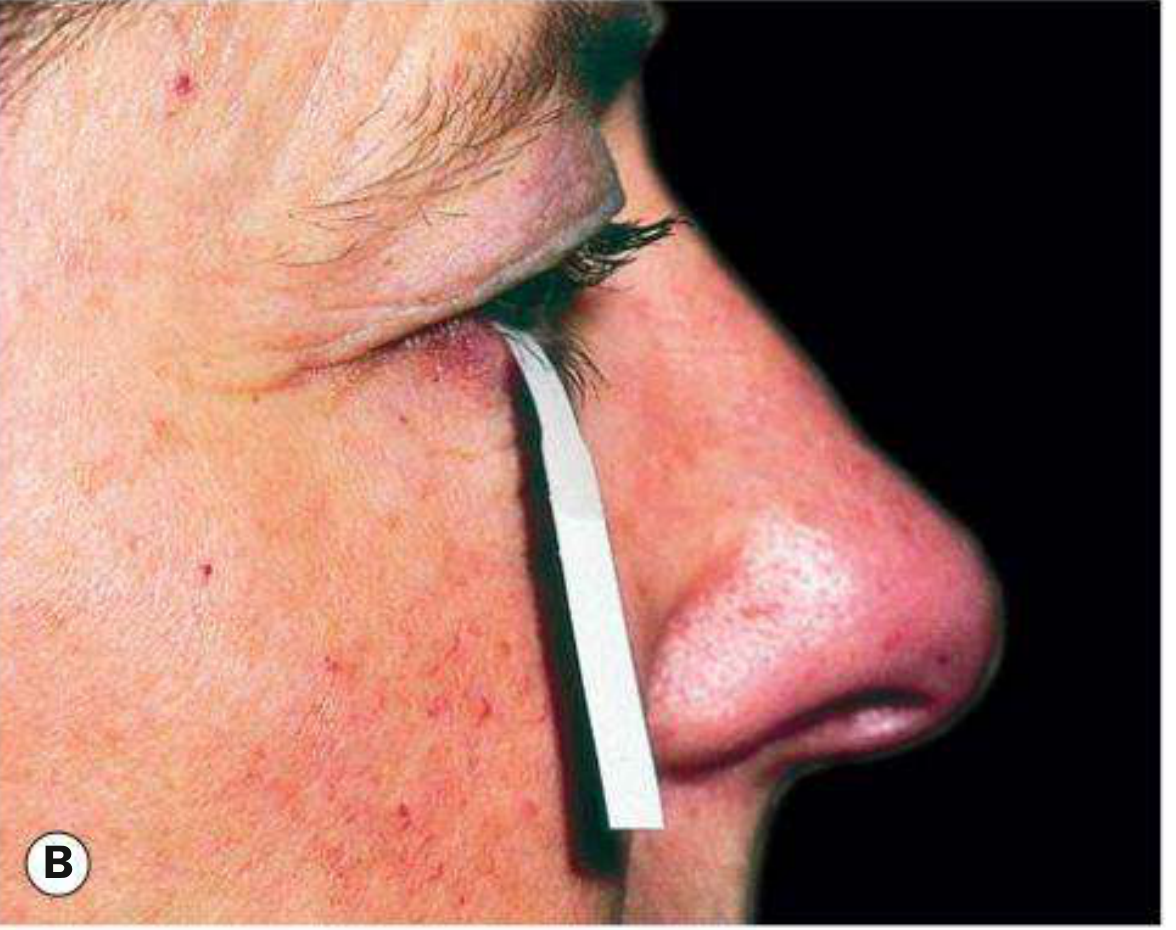
A sterile Whatman No. 41 filter paper strip (5 mm × 35 mm) is folded and hooked over the lower lid at the junction of the medial 2/3 and lateral 1/3.
| Test | Method | Normal | Abnormal |
|---|---|---|---|
| Schirmer I (without anaesthesia) | Measures basic + reflex secretion | ≥15 mm/5 min | <10 mm/5 min |
| Schirmer II (with topical anaesthesia) | Measures basic secretion only | ≥10 mm/5 min | <6 mm/5 min |
| Jones test (basic secretion test) | With anaesthesia + nasal stimulation | Measures reflex secretion | - |
Single Schirmer test should not be the sole criterion; repeatedly abnormal results are highly supportive.
3. Ocular Surface Staining
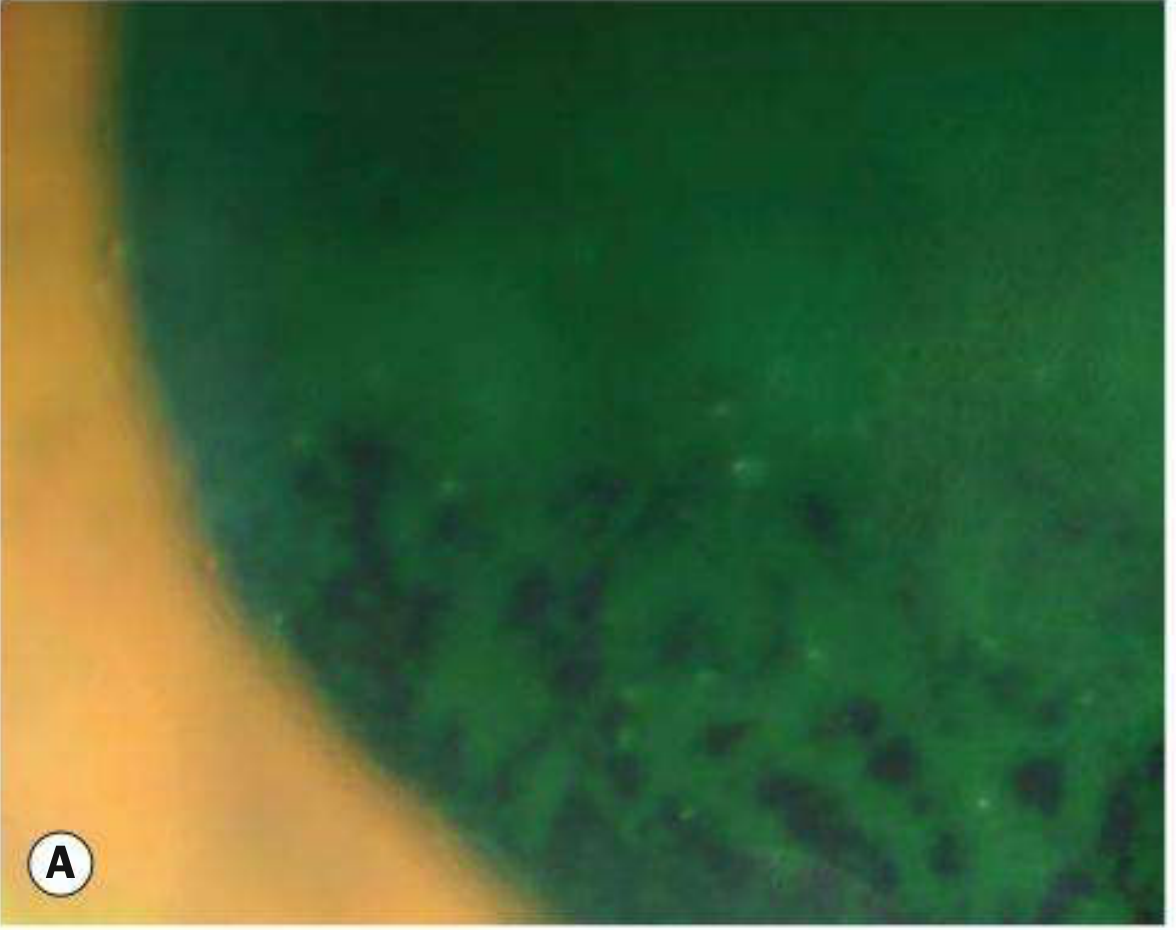
- Fluorescein (blue light): Stains areas of epithelial loss (erosions); also used for TBUT
- Rose Bengal: Stains devitalized and dead epithelial cells and mucus strands; more irritating
- Lissamine green: Similar to rose Bengal, better tolerated, stains dead cells and mucus
- Distribution: Typically interpalpebral (exposed area between lids) and inferior cornea
4. Tear Film Osmolarity
- Measured with TearLab osmometer (point-of-care device)
- Normal: <308 mOsm/L
- Dry eye: ≥316 mOsm/L (hyperosmolarity is the core pathogenic mechanism)
- High specificity but variable between tests
5. Meibomian Gland Assessment
- Slit-lamp: Expressed secretions (clear/cloudy/solid), gland orifice obstruction
- Meibography: Infrared imaging of meibomian gland architecture (dropout/atrophy)
6. Conjunctival Impression Cytology
- Sample of conjunctival epithelium analyzed for:
- Goblet cell density (reduced in dry eye)
- Squamous metaplasia (keratinization)
- Inflammatory cells
7. Tear Lysozyme / Lactoferrin Levels
- Reduced in aqueous-deficient dry eye
- Not routinely measured in clinical practice
8. Phenol Red Thread Test
- Thread impregnated with phenol red dye placed in lower fornix for 15 seconds
- Normal: >9 mm of wetting; Dry eye: <9 mm
Grading of Dry Eye Severity (DEWS 2007)
| Level | Symptoms | Signs |
|---|---|---|
| 1 (Mild) | Mild, episodic | Mild conjunctival signs |
| 2 (Moderate) | Moderate, episodic or chronic | TBUT ≤10 sec; mild punctate staining |
| 3 (Severe) | Frequent, chronic | Marked staining; filamentary keratitis |
| 4 (Very Severe) | Constant, disabling | Corneal ulceration; scarring |
Treatment - Step-Ladder Approach (DEWS Levels)
Level 1 (Mild) - Education and Environment
- Patient education: reduce screen time, increase blink frequency
- Lifestyle modification: humidifiers, avoid smoke/wind/air-conditioning
- Artificial tears (preservative-free preferred) 4 times daily - first-line
- Cellulose derivatives (hypromellose, methylcellulose) - mild cases
- Carbomer gels - longer-lasting, slight blurring
- Sodium hyaluronate, polyvinyl alcohol (PVA), propylene glycol
- Lid hygiene and warm compresses for MGD/blepharitis
Level 2 (Moderate) - Add Anti-inflammatory + Conserve Tears
- Increase artificial tears to every 1-2 hours (preservative-free only)
- Lubricating gel or ointment at bedtime
- Cyclosporine 0.05-0.09% eye drops b.i.d. (Restasis)
- Immunomodulatory; reduces T-cell mediated inflammation
- Takes 1-3 months for significant effect; often burns initially
- A short course of mild topical steroid (loteprednol 0.5%, fluorometholone 0.1%) b.i.d.-q.i.d. for 1 month can be given concurrently to hasten effect
- Lifitegrast 5% eye drops b.i.d. (LFA-1 antagonist, blocks T-cell adhesion)
- Symptomatic improvement within 2 weeks; full effect by 3 months
- Punctal occlusion (if above measures fail or impractical)
- Collagen plugs (temporary, dissolve in 1-2 weeks)
- Silicone/acrylic plugs (reversible, longer lasting)
- Treat blepharitis/inflammation before occluding puncta
- Omega-3 fatty acid supplements (oral flaxseed oil)
- Topical short-term steroids (prednisolone, loteprednol) for acute exacerbations
- Moisture chamber spectacles / side shields
Level 3 (Severe) - Advanced Measures
- Autologous serum eye drops (contains growth factors, fibronectin, vitamins - approximates natural tears better than artificial tears)
- Umbilical cord serum drops
- All four puncta occluded (upper + lower)
- Bandage soft contact lens (for filamentary keratitis, corneal exposure)
- Scleral contact lenses (large PMMA/silicone lens that vaults the cornea; maintains fluid reservoir)
- Acetylcysteine 10% drops for filamentary keratitis (mucolytic)
- Manual debridement of corneal filaments
Level 4 (Very Severe) - Surgery
- Systemic anti-inflammatory agents (methotrexate, hydroxychloroquine for Sjögren's)
- Tarsorrhaphy (permanent or temporary) - reduces exposed ocular surface area and evaporation
- Salivary gland autotransplantation (parotid duct transposed to the temporal conjunctival fornix)
- Mucous membrane / amniotic membrane transplantation for corneal complications
- Conjunctival/limbal stem cell transplantation for severe surface disease
Special Conditions Associated with Dry Eye
Sjögren Syndrome
- Classic triad: Dry eyes + Dry mouth + Parotid gland enlargement
- Autoimmune: Anti-Ro (SSA) and Anti-La (SSB) antibodies
- Diagnosis: ACR criteria - anti-SSA/SSB positivity, ocular surface staining, labial salivary gland biopsy showing focal lymphocytic sialadenitis
Filamentary Keratitis
- Fine strands of mucus and desquamated epithelial cells anchored to the cornea
- Seen in severe dry eye, prolonged patching, keratoconus
- Treatment: Lubricants, acetylcysteine, bandage lens, manual debridement
Key Exam Points Summary
| Feature | Key Point |
|---|---|
| Most common cause | Meibomian gland dysfunction (evaporative) |
| Core mechanism | Tear instability → hyperosmolarity → inflammation → surface damage |
| Paradoxical finding | Excess tearing (reflex lacrimation due to irritation) |
| Best screening test | TBUT (<10 sec = abnormal) |
| Aqueous secretion test | Schirmer's test (<10 mm/5 min with anaesthesia) |
| Vital staining | Rose Bengal / Lissamine green (dead cells); Fluorescein (erosions) |
| Distribution of staining | Interpalpebral / inferior cornea |
| First-line treatment | Preservative-free artificial tears |
| Anti-inflammatory drops | Cyclosporine 0.05-0.09% OR Lifitegrast 5% |
| Conserve tears surgically | Punctal occlusion |
| Most common systemic association | Sjögren syndrome / Rheumatoid arthritis |
| Severe corneal complication | Filamentary keratitis, sterile ulceration |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition (Chapter 5: Dry Eye); Wills Eye Manual (Section 4.3); aligned with A K Khurana Comprehensive Ophthalmology syllabus
This is a shared conversation. Sign in to Orris to start your own chat.