CTG graph to test myself
Asking for Preferences
Searching the Web
CTG cardiotocography trace image for teaching beginners interpret
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I have a real textbook CTG image with 5 different patterns. Here is your self-test!
CTG Self-Test - Beginner Level
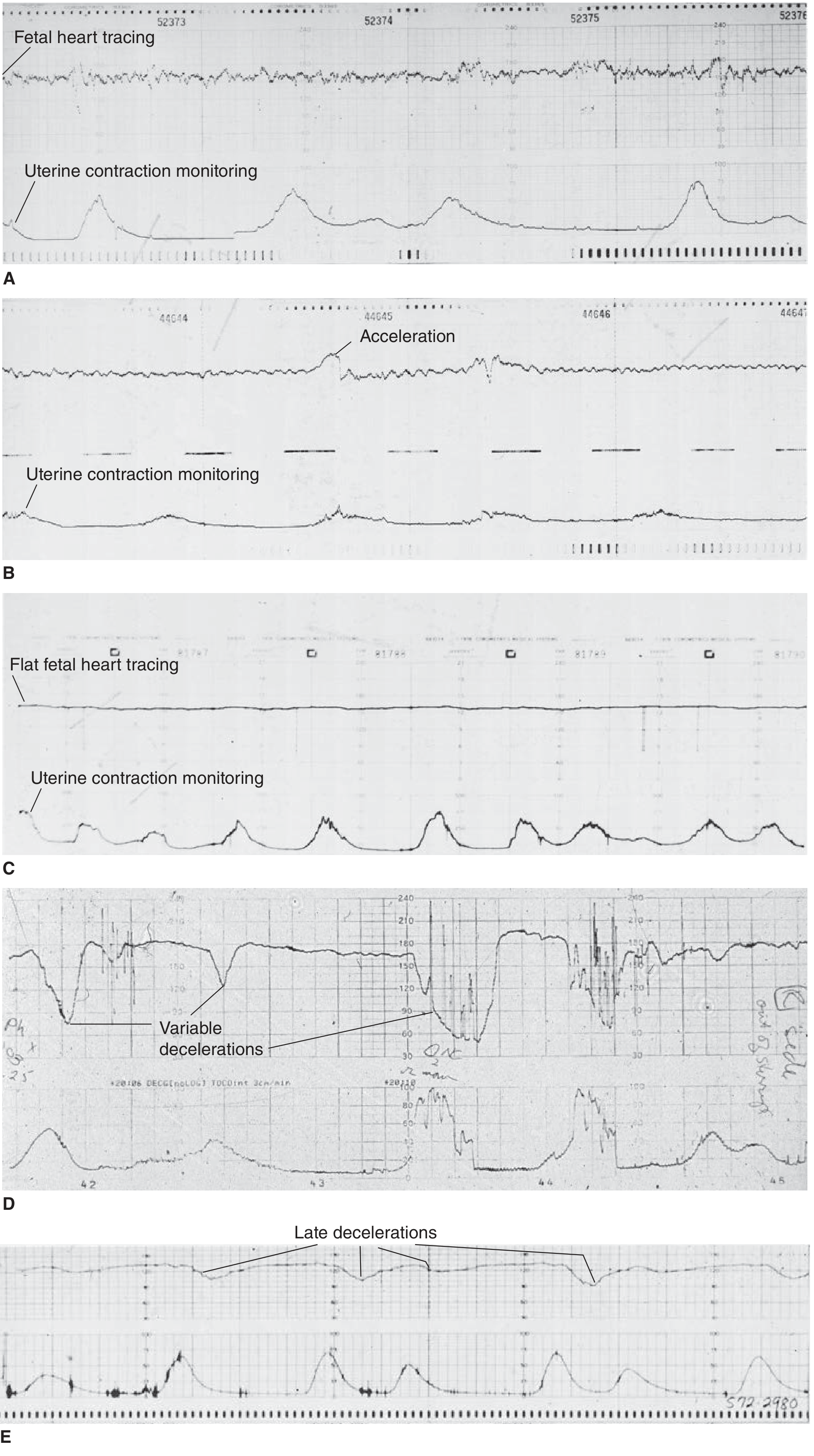
Here is a real CTG trace from Tintinalli's Emergency Medicine showing 5 different patterns (A to E). Each panel shows the fetal heart rate (top) and uterine contractions (bottom).
Your Questions
Look at each panel and answer before reading the explanation below:
1. Panel A - What do you notice about the fetal heart rate tracing? Is this reassuring or concerning?
2. Panel B - There is a brief rise in the fetal heart rate visible. What is this called, and what does it tell you?
3. Panel C - The fetal heart tracing is described as "flat." What does this mean, and what might cause it?
4. Panel D - The fetal heart rate shows sudden sharp dips. What type of deceleration is this, and what is the likely cause?
5. Panel E - The heart rate dips are labeled. Look at their timing relative to the contractions. What type is this, and why is it dangerous?
Answers (read after you've tried!)
| Panel | Pattern | What it means |
|---|---|---|
| A | Good variability | The FHR wiggles continuously around the baseline (~120-160 bpm). This is reassuring - it shows an intact fetal autonomic nervous system. |
| B | Accelerations | Brief rises of FHR above baseline. Reactive = at least 2 accelerations of ≥15 bpm lasting ≥15 seconds. This is the most reassuring CTG feature. |
| C | Poor / absent variability (flat trace) | The FHR is suspiciously smooth with very little beat-to-beat variation. May indicate fetal hypoxia, deep sleep, or drug effect. Concerning. |
| D | Variable decelerations | Abrupt, unpredictable dips with no fixed relationship to contractions. Caused by cord compression - the cord is being intermittently squeezed. |
| E | Late decelerations | Dips that start after the contraction begins and recover slowly after it ends. Caused by uteroplacental insufficiency - the placenta can't deliver enough oxygen during contractions. This is the most sinister pattern. |
Key Beginner Framework (remember these 4 features)
| Feature | Normal | Concerning |
|---|---|---|
| Baseline rate | 110-160 bpm | <110 (bradycardia) or >160 (tachycardia) |
| Variability | Moderate (6-25 bpm fluctuation) | Absent/minimal (<5 bpm) |
| Accelerations | Present (reactive) | Absent for >40 min |
| Decelerations | Early decs (benign) | Late or prolonged variable decs |
- Source: Tintinalli's Emergency Medicine, Fig. 101-1
- Source: Textbook of Family Medicine 9e, Chapter 20
Want to move on to the next level - interpreting FIGO categories (I/II/III) or case-based scenarios with management decisions?
This is a shared conversation. Sign in to Orris to start your own chat.