Hypertension
Reading File
Finding Sources
Searching PubMed
"hypertension"[MeSH Terms] AND "guideline"[pt]
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
I now have all the information needed for a comprehensive, well-sourced response. Here it is:
Hypertension
Definition and Classification
Hypertension is defined as persistently elevated arterial blood pressure that, over time, damages target organs and raises cardiovascular (CV) risk. The 2017 ACC/AHA guidelines (the most current US standard) classify BP as follows:
| BP Category | SBP | DBP | |
|---|---|---|---|
| Normal | <120 mm Hg | and | <80 mm Hg |
| Elevated | 120-129 mm Hg | and | <80 mm Hg |
| Stage 1 HTN | 130-139 mm Hg | or | 80-89 mm Hg |
| Stage 2 HTN | 140-159 mm Hg | or | 90-99 mm Hg |
| Stage 3 HTN | ≥160 mm Hg | or | ≥100 mm Hg |
If SBP and DBP fall in different categories, the higher category applies (e.g., 162/92 = Stage 3). For CKD patients, any BP >130/80 mm Hg warrants pharmacotherapy.
The figure below shows how the classification threshold has evolved from JNC I (1977) through the current ACC/AHA scheme:
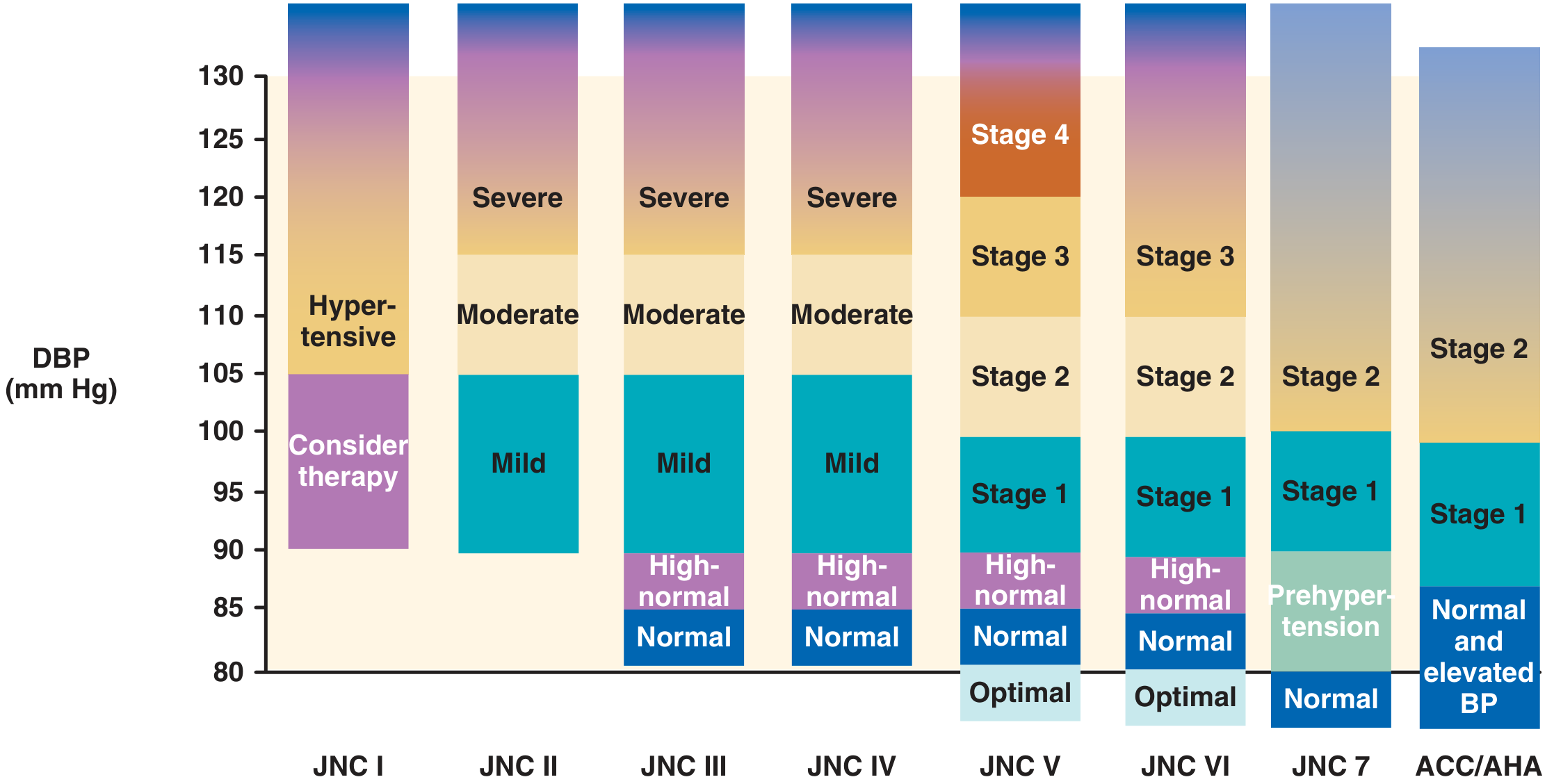
Brenner and Rector's The Kidney, Fig. 46.2 - Evolution of BP classification thresholds across major guidelines
Epidemiology
- Affects approximately 1 billion people worldwide and is the single leading attributable risk for global mortality (Global Burden of Disease Study 2010).
- In the US, prevalence is markedly higher in non-Hispanic Black adults (~41%) vs. non-Hispanic whites (~28%) - a disparity that persists in mortality data (stroke death rates 41% higher, hypertensive renal disease deaths 111% higher in Blacks vs. whites).
- Men develop hypertension and its complications roughly a decade earlier than women, though after age 70 women overtake men in prevalence.
- Prevalence increases steeply with age.
Pathophysiology
The Hemodynamic Equation
BP = Cardiac Output (CO) × Peripheral Vascular Resistance (PVR)
Antihypertensive drugs target one or both sides of this equation. Four anatomic control sites regulate BP:
- Arterioles (resistance vessels)
- Postcapillary venules (capacitance vessels)
- Heart (CO)
- Kidney (intravascular volume)
These are coordinated by baroreflexes, the autonomic nervous system, and the renin-angiotensin-aldosterone system (RAAS).
Essential Hypertension (90-95% of cases)
No single cause is identifiable. It is a multifactorial disorder driven by:
- Genetic factors (heritability ~30%; polygenic; variants in genes for angiotensinogen, ACE, angiotensin II receptor, β2-adrenoceptor, α-adducin, uromodulin)
- Excess dietary sodium (increased BP with aging does not occur in populations with low sodium intake)
- Obesity and visceral adiposity
- Psychological stress, alcohol, and physical inactivity
Secondary Hypertension (5-10% of cases)
Important to identify because some causes are surgically curable.
| Category | Examples |
|---|---|
| Renal | Renal artery stenosis, acute/chronic glomerulonephritis, polycystic kidney disease, renin-secreting tumors |
| Endocrine | Primary aldosteronism, Cushing syndrome, pheochromocytoma, acromegaly, hyperthyroidism, congenital adrenal hyperplasia |
| Cardiovascular | Coarctation of the aorta, polyarteritis nodosa |
| Hormonal/Drug | Oral contraceptives, glucocorticoids, sympathomimetics, NSAIDs |
| Neurological | Sleep apnea, raised intracranial pressure |
| Pregnancy | Preeclampsia |
Robbins Pathologic Basis of Disease, Table 11.2
Complications (Target Organ Damage)
Hypertension is typically asymptomatic until late in its course. Left untreated:
- ~50% of hypertensive patients die of ischemic heart disease or heart failure
- ~33% die of stroke
Major end-organ complications:
- Cardiac: LV hypertrophy, heart failure, coronary artery disease
- Cerebrovascular: stroke, multi-infarct dementia
- Renal: hypertensive nephrosclerosis, ESKD
- Vascular: aortic dissection, peripheral arterial disease (2.5x risk in men, 3.9x in women)
- Retinal: hemorrhages, exudates, papilledema (in malignant HTN)
Malignant Hypertension
A rapidly progressive form (~5% of hypertensives) with SBP >180 and DBP >120 mm Hg, characterized by renal failure, retinal hemorrhages/exudates, and papilledema. Fatal within 1-2 years if untreated.
Measurement Principles
Proper office measurement requires:
- Patient seated at rest for 5 minutes, feet flat, arm at heart level
- Correct cuff size (use large adult cuff for arm circumference 35-44 cm; thigh cuff for 45-52 cm)
- Cuff lower edge ~2-3 cm above antecubital fossa
- At least two readings, averaged; obtain more if disparity >10 mm Hg between readings
- Measure both arms (~20% of individuals have >10 mm Hg difference; report the higher arm)
- Use Korotkoff phase I (SBP) and phase V (DBP)
ACC/AHA 2017 Guideline measurement protocol
Lifestyle Modifications (Non-Pharmacologic Treatment)
These should be initiated in all hypertensive patients, alongside or before drugs in Stage 1:
| Modification | Recommendation | Expected SBP Reduction |
|---|---|---|
| Weight loss | Maintain BMI 18.5-24.9 | 5-20 mm Hg per 10 kg lost |
| DASH diet | Fruits, vegetables, low-fat dairy; reduced saturated fat | 8-14 mm Hg |
| Sodium restriction | <2,300 mg/day (≤100 mmol/day) | 2-8 mm Hg |
| Aerobic exercise | ≥30 min/day, most days | 5-8 mm Hg |
| Dynamic resistance | 90-150 min/wk | 4 mm Hg |
| Alcohol reduction | ≤2 drinks/day (men); ≤1 drink/day (women) | 2-4 mm Hg |
The DASH diet alone produces an average SBP reduction of 7.6 mm Hg and DBP of 4.2 mm Hg. National Kidney Foundation Primer on Kidney Diseases, Table 64.9
Pharmacologic Treatment
First-Line Drug Classes
All of the following have been shown to reduce hypertensive complications and are appropriate as initial monotherapy:
| Class | Mechanism | Key Notes |
|---|---|---|
| Thiazide diuretics (e.g., chlorthalidone, HCTZ) | Reduce volume; decrease PVR with chronic use | Preferred in Blacks and elderly; better than amlodipine for HF; better than lisinopril for stroke |
| ACE inhibitors (e.g., lisinopril, enalapril) | Block conversion of angiotensin I to II; reduce aldosterone | First-line in CKD with proteinuria, diabetes; avoid in pregnancy |
| ARBs (e.g., losartan, irbesartan) | Block AT1 receptors | Same indications as ACEi; better tolerated (no cough) |
| Calcium channel blockers (e.g., amlodipine, diltiazem) | Reduce PVR via vascular smooth muscle relaxation | Useful with angina; combine well with ACEi/ARB |
Beta-blockers are currently not recommended as first-line therapy for uncomplicated hypertension (less effective at reducing CV events compared to the above classes).
Selecting by Comorbidity
- Diabetes / CKD with proteinuria: ACEi or ARB
- Angina: Beta-blocker or calcium channel blocker
- Heart failure: Diuretics, ACEi/ARB, beta-blockers, hydralazine + nitrates
- Benign prostatic hyperplasia: Alpha-1 blocker (doxazosin, terazosin)
- Black patients: Diuretics or CCBs preferred over beta-blockers and ACEi
Combination Therapy
Most patients with moderate-severe hypertension require 2+ agents. Effective combinations:
- Diuretic + ACEi or ARB + CCB (triple combination)
- If a 4th drug is needed: add a sympatholytic (beta-blocker or clonidine)
- Fixed low-dose triple combination (e.g., telmisartan 20 mg + amlodipine 2.5 mg + chlorthalidone 12.5 mg once daily) has demonstrated high efficacy with minimal side effects
BP target: systolic <120 mm Hg for high-CV-risk patients (SPRINT trial data).
Katzung's Basic & Clinical Pharmacology, 16th Ed.
Resistant Hypertension
BP remaining above goal despite an optimal 3-drug regimen that includes a diuretic. Common causes:
- Poor medication compliance
- Excessive sodium intake or alcohol
- Inadequate diuretic dosing
- Concomitant conditions: obesity, sleep apnea, primary aldosteronism, CKD, metabolic syndrome
- Interfering drugs: NSAIDs, sympathomimetics, corticosteroids, tricyclic antidepressants, oral contraceptives, stimulants (amphetamine, cocaine)
Hypertensive Emergency vs. Urgency
| Emergency | Urgency | |
|---|---|---|
| BP level | SBP >180 or DBP >120 mm Hg | SBP >180 or DBP >120 mm Hg |
| Target organ damage | Present (stroke, MI, acute pulmonary edema, acute renal failure, retinal changes) | Absent |
| Treatment route | Intravenous | Oral |
| Initial BP reduction goal | Reduce MAP by no more than 25% within minutes to hours (avoid rapid drop) | Gradual reduction over 24-48 hours |
IV Agents for Hypertensive Emergency
| Drug | Class | Notes |
|---|---|---|
| Nicardipine, clevidipine | CCB | Widely used; titratable |
| Sodium nitroprusside | Nitric oxide donor | Potent but risk of cyanide toxicity with prolonged use |
| Nitroglycerin | Nitric oxide donor | Preferred when HTN + pulmonary edema or ACS |
| Labetalol | Alpha + beta blocker | Good for aortic dissection, post-op HTN |
| Esmolol | Beta-1 blocker (IV) | Short half-life (~10 min); useful when concerned about HF exacerbation |
| Phentolamine | Alpha blocker | Pheochromocytoma crisis |
| Fenoldopam | Dopamine agonist | Renal protection |
| Enalaprilat | ACEi (IV) | Acute LV failure |
Lippincott Illustrated Reviews Pharmacology
Special Populations
- Children/Adolescents: BP interpretation uses age-, sex-, and height-adjusted percentile tables. Hypertension = BP between 95th-99th percentile (average of 3 visits).
- Elderly: Isolated systolic hypertension (SBP ≥160 with normal DBP) is common and should be treated; systolic BP predicts ~89% of age-stratified stroke deaths and ~93% of CHD deaths.
- Pregnancy: Preeclampsia is a distinct entity. Standard oral antihypertensives (ACEi, ARBs) are contraindicated in pregnancy.
- PAD patients: Beta-blockers are safe (do not worsen claudication per meta-analysis). ACEi may provide vascular protection beyond BP lowering.
Sources: Brenner and Rector's The Kidney (2-Volume Set) | Katzung's Basic & Clinical Pharmacology, 16th Ed. | Robbins, Cotran & Kumar Pathologic Basis of Disease | Lippincott Illustrated Reviews Pharmacology | National Kidney Foundation Primer on Kidney Diseases, 8e | Textbook of Family Medicine, 9e
This is a shared conversation. Sign in to Orris to start your own chat.