Clinical discussion of pih
Reading File
Finding Sources
Finding Sources
Searching PubMed
pregnancy induced hypertension preeclampsia management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have very rich material from multiple authoritative textbooks. Let me compile the full clinical discussion.
Pregnancy-Induced Hypertension (PIH): A Clinical Discussion
1. Definition and Classification
PIH (Pregnancy-Induced Hypertension) is an umbrella term for hypertensive disorders that arise during pregnancy. Hypertension affects up to 8-10% of all pregnancies and is classified into several distinct entities:
| Category | Definition |
|---|---|
| Gestational Hypertension | New BP ≥ 140/90 mmHg after 20 weeks gestation; resolves postpartum; no proteinuria |
| Preeclampsia | Gestational hypertension + proteinuria (>300 mg/24 hr) or end-organ damage after 20 weeks |
| Eclampsia | Seizures superimposed on preeclampsia |
| Superimposed Preeclampsia | Preeclampsia developing in a woman with pre-existing chronic hypertension |
| Chronic/Coincidental Hypertension | Present before pregnancy or persists >6 weeks postpartum |
- Rosen's Emergency Medicine, 10th Ed.
- Creasy & Resnik's Maternal-Fetal Medicine
2. Epidemiology
- Hypertensive disorders of pregnancy occur at approximately 85 per 1,000 deliveries in the United States.
- Preeclampsia specifically affects 3-7% of pregnancies; eclampsia has become rare with modern care.
- Nulliparity accounts for the largest population-attributable fraction (~32%) of preeclampsia risk.
Risk Factors:
-
Nulliparity (greatest single risk factor)
-
Extremes of maternal age (<20 and >35 years)
-
Prior history of preeclampsia
-
Chronic hypertension (25% risk of superimposed preeclampsia)
-
Pregestational diabetes mellitus (20% overall risk; up to 70% with classes F/R)
-
Chronic renal failure
-
Antiphospholipid syndrome
-
Connective tissue disorders (SLE)
-
Twin/multiple gestation, molar pregnancy
-
Obesity, hypercholesterolemia
-
Family history of PIH
-
In vitro fertilization
-
Creasy & Resnik's Maternal-Fetal Medicine
3. Pathophysiology
This is the most complex and fascinating aspect of PIH. The central defect is inadequate trophoblastic invasion of the spiral arteries.
3a. Normal Placentation vs. PIH
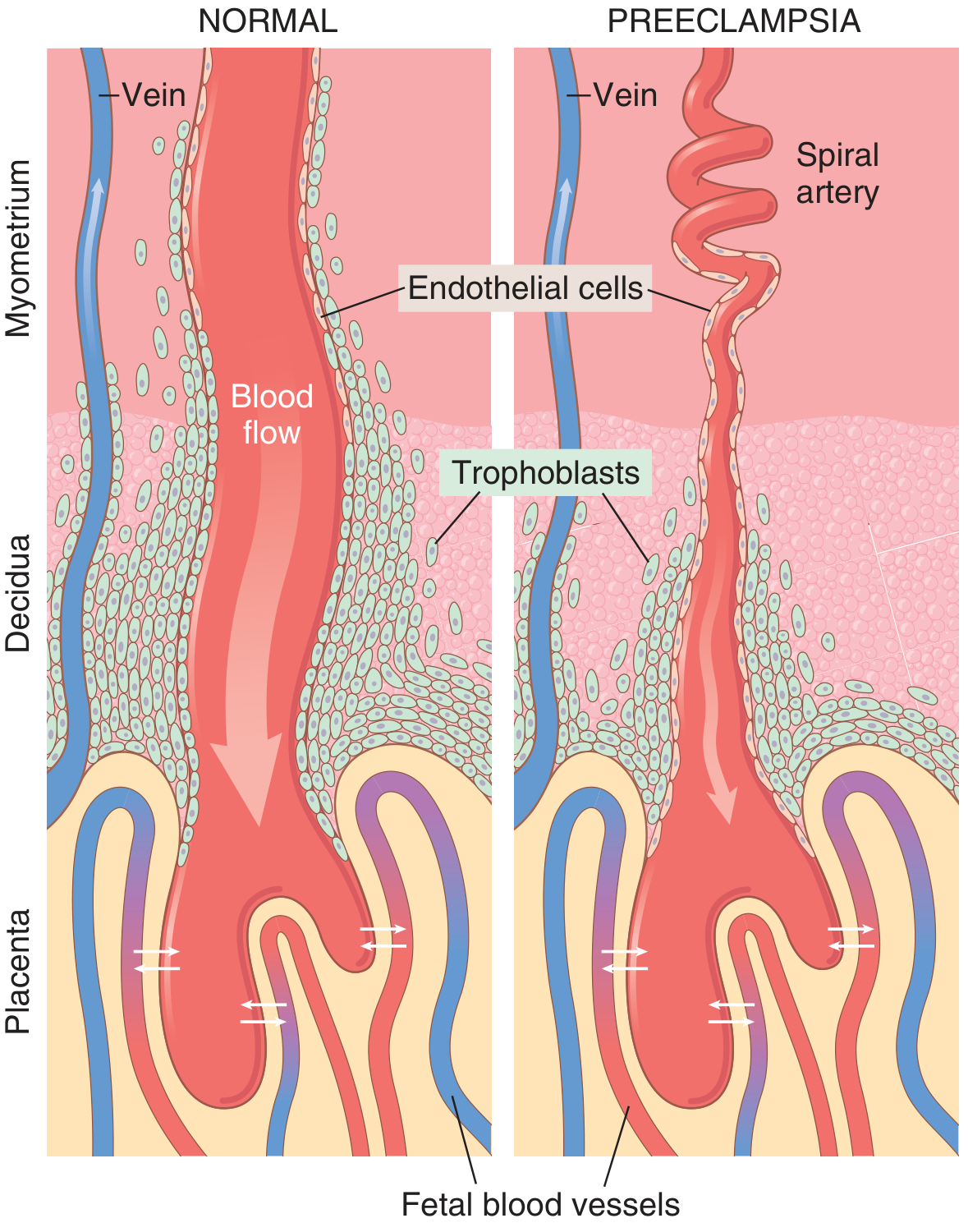
Normal pregnancy (left): Trophoblasts deeply invade spiral arteries, transforming them into wide, low-resistance sinusoids with high blood flow. Preeclampsia (right): Trophoblastic invasion fails; arteries remain narrow and coiled, resulting in placental ischemia. (Guyton & Hall Textbook of Medical Physiology)
In normal pregnancy, trophoblasts invade the spiral arteries of the uterine endometrium, remodeling their musculoelastic walls into wide vascular sinusoids with high flow and low resistance. In preeclampsia, this remodeling fails. The arteries retain their musculoelastic walls, remain narrow, and produce chronic placental hypoperfusion.
3b. The Cascade from Placental Ischemia to Systemic Disease
Placental ischemia triggers release of circulating vasoactive and anti-angiogenic factors into the maternal bloodstream:
- Anti-angiogenic proteins - Soluble FMS-like tyrosine kinase 1 (sFlt-1) and soluble endoglin are released by the ischemic placenta. These antagonize the effects of VEGF and TGF-β, causing widespread maternal endothelial dysfunction.
- Pro-inflammatory cytokines - TNF-α and IL-6 levels rise, amplifying vascular injury.
- Prostanoid imbalance - Reduced endothelial production of vasodilators (prostacyclin/PGI₂, PGE₂) combined with increased vasoconstrictor thromboxane A₂ results in systemic vasoconstriction.
- Endothelial dysfunction - Results in vascular hyperreactivity, increased peripheral resistance, and microangiopathy across organs.
The net hemodynamic pattern evolves:
-
Early: Elevated cardiac output, then rising peripheral resistance
-
Late: Cardiac output drops as peripheral resistance markedly increases
-
Robbins & Kumar Basic Pathology; Guyton & Hall Medical Physiology
3c. Consequences of Endothelial Dysfunction
| Organ/System | Effect |
|---|---|
| Kidneys | Decreased RBF and GFR, glomerular endotheliosis, proteinuria, oliguria |
| Brain | Cerebral vasospasm, encephalopathy, seizures (eclampsia), intracranial hemorrhage |
| Liver | Periportal hemorrhage, hepatocellular necrosis, RUQ pain |
| Placenta | Infarction, retroplacental hemorrhage, fetal growth restriction |
| Coagulation | Hypercoagulability, thrombocytopenia, possible DIC |
| Cardiovascular | Systemic vasoconstriction, hypertension, pulmonary edema |
4. Clinical Features
4a. Preeclampsia
Classic triad: Hypertension + Proteinuria + Edema (after 20 weeks)
- BP ≥ 140/90 mmHg on two occasions, at least 4 hours apart
- Proteinuria >300 mg/24 hr (or protein:creatinine ratio ≥0.3)
- Edema (particularly face and hands; non-dependent edema)
- Symptoms: headache, visual disturbances (scotomata, blurring), epigastric/RUQ pain, nausea
4b. Severe Preeclampsia Features
Any of:
- BP ≥ 160/110 mmHg (persistent ≥15 min)
- Thrombocytopenia (<100,000/µL)
- Renal insufficiency (creatinine >1.1 mg/dL)
- Impaired liver function (AST/ALT ≥2x upper limit)
- Pulmonary edema
- New-onset headache unresponsive to medication
- Visual disturbances
4c. HELLP Syndrome
A particularly severe variant (~10% of severe preeclampsia):
- Hemolysis (microangiopathic hemolytic anemia)
- Elevated Liver enzymes (ALT/AST >70 U/L)
- Low Platelets (<100,000/mL)
- Can be complicated by DIC
- High mortality if not recognized promptly
4d. Eclampsia
-
Generalized tonic-clonic seizures in a patient with signs/symptoms of preeclampsia
-
Can occur antepartum, intrapartum, or postpartum (20% of eclampsia occurs >48 hours after delivery)
-
Progression from preeclampsia to eclampsia is unpredictable and can be rapid
-
Rosen's Emergency Medicine; Goodman & Gilman's Pharmacology
5. Pathological (Morphological) Changes
Placental:
- Numerous placental infarcts
- Retroplacental hemorrhage
- Ischemic changes of villi (excess syncytial knot formation)
- Abnormal decidual vessels with fibrinoid necrosis and "acute atherosis" (lipid-laden macrophage accumulation)
Renal:
-
Glomerular endotheliosis: swelling of glomerular endothelial cells, protein deposits in basement membranes, reduced glomerular filtration
-
Thickened glomerular tufts
-
Robbins & Kumar Basic Pathology; Guyton & Hall Medical Physiology
6. Investigations
| Investigation | Expected Finding |
|---|---|
| BP monitoring | ≥ 140/90 (gestational) or ≥ 160/110 (severe) |
| 24-hr urine protein | >300 mg/24hr (or spot P:Cr ≥0.3) |
| CBC + platelets | Thrombocytopenia, hemolysis (schistocytes, low Hb) |
| LFTs (AST/ALT) | Elevated in HELLP/severe |
| Serum creatinine | Elevated in severe disease |
| Uric acid | Elevated (marker of disease severity) |
| Coagulation profile | Prolonged PT/PTT, low fibrinogen in DIC |
| Fetal monitoring | NST, BPP, Doppler studies (umbilical artery waveforms) |
| Neuroimaging (CT/MRI) | If altered consciousness or focal neurology |
7. Management
The only definitive treatment is delivery of the baby and placenta, which reverses the placenta-driven pathophysiology. The management strategy balances maternal safety against fetal maturity.
7a. Antihypertensive Therapy
Threshold for treatment:
- Diastolic BP >105 mmHg OR systolic BP >160 mmHg requires drug therapy
- Persistent BP ≥ 160/110 mmHg for ≥15 minutes is a hypertensive emergency requiring immediate treatment
Drugs safe in pregnancy:
| Drug | Route/Dose | Notes |
|---|---|---|
| Methyldopa | 250 mg PO twice daily | Centrally acting α-agonist; gold standard for chronic use; FDA former category B |
| Labetalol | 100 mg PO twice daily (chronic); 20 mg IV → 40 mg IV (acute) | Combined α/β-blocker; first-line for acute severe HTN |
| Nifedipine | 30 mg PO once daily (slow release) | Ca²⁺ channel blocker; safe; reasonable evidence |
| Hydralazine | 5-10 mg IV/IM, repeat q20 min | Direct vasodilator; used for acute BP control |
Drugs CONTRAINDICATED in pregnancy:
- ACE inhibitors (fetotoxic: renal agenesis, oligohydramnios, IUGR)
- Angiotensin receptor blockers (same mechanism, same fetal risk)
7b. Seizure Prophylaxis and Treatment: Magnesium Sulfate
Magnesium sulfate (MgSO₄) is the cornerstone of eclampsia prevention and treatment:
- Has minimal antihypertensive effect
- Is the most effective anticonvulsant in eclampsia
- Maintains uterine and fetal blood flow (unlike other anticonvulsants)
- Used in all women with severe preeclampsia or CNS features (headache, visual disturbance, altered mental status)
- Also given postpartum to women with CNS manifestations
- Loading dose typically 4-6 g IV over 15-20 min; maintenance 1-2 g/hr
Monitoring for MgSO₄ toxicity:
- Loss of patellar reflexes (first sign)
- Respiratory depression (>12 breaths/min required)
- Antidote: Calcium gluconate 1 g IV
7c. Obstetric Management
- Mild preeclampsia at term (≥37 weeks): Deliver
- Severe preeclampsia at any gestation: Deliver after maternal stabilization (BP control + MgSO₄)
- Preterm severe preeclampsia (<34 weeks): Hospitalization, close monitoring, corticosteroids for fetal lung maturity, attempt to prolong pregnancy if safe
- Eclampsia: Stabilize seizures with MgSO₄, control BP, then deliver
7d. Postpartum Care
- BP can worsen in the first 48-72 hrs postpartum
- ~20% of eclampsia cases occur >48 hours after delivery
- Women with severe features should remain on MgSO₄ for 24-48 hrs postpartum
- BP monitoring for at least 1 week postpartum
8. Complications
Maternal:
- Intracranial hemorrhage (leading cause of PIH-related maternal death)
- Hepatic rupture
- Pulmonary edema
- Acute kidney injury
- Placental abruption
- DIC
- Death
Fetal/Neonatal:
- Intrauterine growth restriction (IUGR)
- Preterm birth
- Fetal distress/hypoxia
- Intrauterine fetal death
- Low birth weight
Long-term (maternal):
- Women with preeclampsia have significantly elevated lifetime risk of hypertension, stroke, and cardiovascular disease
9. Prevention
- Low-dose aspirin (75-150 mg/day) from 12-16 weeks is recommended in high-risk women (prior preeclampsia, chronic HTN, diabetes, CKD, multiple gestation). It reduces thromboxane A₂ production and has the best evidence for preeclampsia prevention.
- Calcium supplementation in calcium-deficient populations
- Optimal management of pre-existing conditions (diabetes, HTN, lupus)
- Weight optimization before pregnancy
Sources:
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Robbins & Kumar Basic Pathology (Robbins Pathology)
- Guyton and Hall Textbook of Medical Physiology
- Rosen's Emergency Medicine: Concepts and Clinical Practice, 10th Ed.
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice
This is a shared conversation. Sign in to Orris to start your own chat.