PILON FRACTURE-STAGED MANAGEMENT CONCEPT
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pilon fracture" AND "staged management"
Reading File
Searching PubMed
"tibial pilon" AND "external fixator" AND ORIF
Searching Images
pilon fracture staged management external fixator ORIF
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content. Let me compile the full answer:
Pilon Fracture — Staged Management Concept
What Is a Pilon Fracture?
First described by French radiologist Destot in 1911, a pilon fracture (from French pilon, meaning pestle) is an intra-articular fracture of the distal tibial plafond, where the talus acts as a pestle driving upward into the tibial "ceiling." They are primarily high-energy injuries (MVAs, falls from height) and represent one of the most challenging problems in orthopaedic traumatology — involving both devastating articular comminution and severe soft tissue injury.
Historical Evolution Leading to Staged Treatment
| Era | Approach | Problem |
|---|---|---|
| 1960s–1980s | Rüedi: immediate ORIF (low-energy ski injuries) | Good results, but specific to low-energy fractures |
| 1988 | Mast et al.: delay definitive surgery >8–12 h → wait 7–10 days | First acknowledgment of soft tissue importance |
| 1980s–90s | Early (1–5 day) ORIF became US standard | 50% poor results; wound necrosis, deep sepsis, osteomyelitis |
| Mid-1990s | External fixation alone or hybrid fixation | Higher malunion/nonunion; pin-tract infections |
| 1999 | Sirkin et al.: staged protocol | Major complication rate: 3% closed, 11% open |
The 1999 Sirkin paper is the seminal manuscript that established the modern staged approach. Patterson and Cole corroborated these results. This gave rise to the "span, scan, and plan" philosophy:
Apply external fixation → obtain CT scan → plan definitive ORIF
The Two-Stage Treatment Protocol
STAGE I — Ankle-Spanning External Fixation ± Fibular ORIF
(Performed urgently as soon as the patient's general condition permits)
Goals of Stage I:
- Restore limb length, alignment, and rotation
- Eliminate skin tenting, soft tissue distortion, and areas of ischemia from displaced fragments
- Allow soft tissues to stabilize before definitive surgery
- NOT perfect anatomic reduction — this is a temporary frame
Surgical technique highlights:
- Patient supine on radiolucent table; ipsilateral buttock bump; foam ramp beneath leg
- Two Schanz pins in the tibial diaphysis (anterior-medial cortex) above zone of injury
- Two Schanz pins in the calcaneus ± one in the first metatarsal (to prevent equinus)
- Frame applied to bring ankle to length — do not overdistract (risk of skin necrosis and chronic dystrophy)
- Length reference: normal relationship of the lateral process of talus with distal fibula tip
- CT scan of distal tibia obtained after external fixator placement for surgical planning
- A semicircular bar can elevate the foot off the bed to prevent heel ulcers
Fibular fixation in Stage I:
- Fibular plate/nail almost always indicated — provides rigid lateral construct against coronal (varus/valgus) collapse
- Fibular incision must be placed posterior to the fibula to allow a wide skin bridge with future anterior/medial incisions
- If the Stage I surgeon will NOT perform Stage II: apply external fixator only — do not attempt ORIF to avoid poorly placed incisions or malreduced fibula requiring revision
Equipment needed:
- Large external fixator set
- Periarticular fibular plates (1/3 tubular, mini-fragment)
- Small-fragment and mini-fragment screws
INTERVAL: WAITING FOR SOFT TISSUE RECOVERY
The critical window between Stage I and Stage II.
Readiness criteria for Stage II:
- Return of skin wrinkles over the dorsum of the foot/ankle (indicates resolution of swelling)
- Fracture blisters have re-epithelialized
- Wounds healed
- Typically 10–21 days from injury
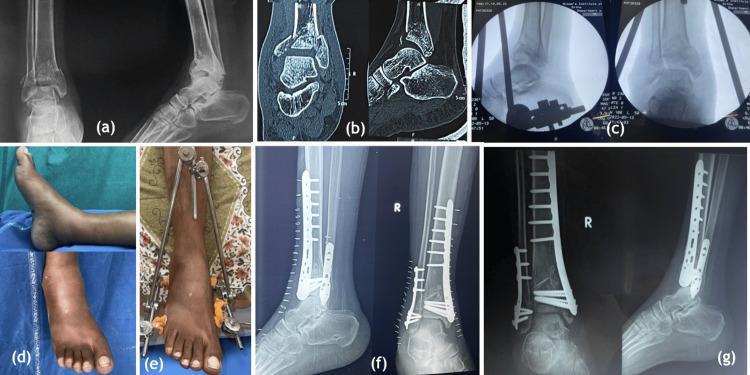
STAGE II — Definitive ORIF of the Tibial Plafond
(After soft tissue recovery, typically at 10–21 days)
Three overriding surgical goals:
- Anatomic articular reduction
- Stable metaphyseal-diaphyseal fixation with acceptable alignment
- Avoidance of soft tissue complications
The Column Theory (planning framework):
The distal tibia is divided into three columns, each requiring mechanically appropriate fixation:
| Column | Anatomy | Implant |
|---|---|---|
| Medial | Medial tibia → medial malleolus | Medial periarticular locking plate |
| Lateral | Anterolateral tibia → Chaput tubercle + fibula | Anterolateral plate ± fibular fixation |
| Posterior | Posterior tibia → posterior malleolus (Volkmann fragment) | Posterior buttress plate or AP lag screws |
Most early failures are due to inadequate fixation constructs or fixation placed on the wrong column.
Surgical approach principles:
- Anterior and anteromedial approaches most common
- Wide skin bridge ≥7 cm between any two incisions (critical to prevent wound breakdown)
- Femoral distractor used for indirect ligamentotaxis reduction
- K-wires provisionally hold articular fragments
- Lag screws compress articular fragments → followed by periarticular plate to shaft
Implants:
- Precontoured periarticular anterolateral and medial distal tibial locking plates — multiple epiphyseal screws + indirect metaphyseal reduction
- Supplementary malleable plates (distal radius T-plates, ¼ tubular) only in conjunction with stiffer metadiaphyseal implants
Classification (AO/OTA) — Relevance to Staging
| Type | Description | Typical Management |
|---|---|---|
| 43A | Extra-articular | May tolerate earlier ORIF or IM nail |
| 43B | Partial articular (split/depression) | Staged if significant soft tissue injury |
| 43C | Complete articular (C1–C3) | Classic indication for staged protocol |
43C fractures (especially C3 with severe comminution) are the paradigmatic indication for the two-stage protocol.
Author's Preferred Treatment Summary (Rockwood & Green, 10th ed.)
For 43B:
- Stage I: External fixation ± fibular fixation
- Stage II: Articular ORIF via limited approach; bone graft for split-depression defects (elevate impacted articular surface using talus as template)
For 43C:
- Stage I: Spanning external fixator + fibular ORIF (posterior fibular incision)
- Interval: CT scan + surgical planning
- Stage II: Full articular reconstruction — anterolateral and/or medial plates based on column analysis; posterior malleolus addressed first when significantly displaced
Complications
| Complication | Comment |
|---|---|
| Superficial wound dehiscence | Most common; manage with local wound care |
| Deep infection / osteomyelitis | Most feared; often requires hardware removal + bone transport |
| Nonunion | Requires staged management — hardware removal → grafting ± correction of alignment |
| Posttraumatic arthritis | Occurs even with perfect reduction due to cartilage apoptosis from axial impaction; may require eventual ankle fusion or total ankle replacement |
Key Takeaways
- The staged protocol was popularized by Sirkin et al. (1999) — "span, scan, and plan"
- Stage I (emergency): restore length/alignment with spanning external fixator ± fibular ORIF
- Interval (10–21 days): wait for soft tissue recovery — wrinkle sign is the clinical marker
- Stage II (definitive): anatomic articular ORIF using column theory; wide skin bridges mandatory
- Fibular incision must be posterior; definitive tibial surgeon should plan all Stage I incisions
- Even anatomic reduction does not guarantee freedom from posttraumatic arthritis — patient counseling is essential
Rockwood and Green's Fractures in Adults, 10th ed. 2025; Sirkin et al., J Orthop Trauma 1999;13(2):78–84
This is a shared conversation. Sign in to Orris to start your own chat.