Someone with a stroke, 54 years male, and family history of high cholesterol and blood pressure. Differential diagnosis for this patient.
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"ischemic stroke" AND "differential diagnosis"
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have all the information needed for a comprehensive differential diagnosis. Here is a structured, textbook-grounded answer:
Differential Diagnosis: 54-Year-Old Male Presenting with Stroke + FHx Hypertension & Hypercholesterolemia
This patient's profile (middle-aged male, family history of hypertension and hypercholesterolemia) points strongly toward atherosclerotic cerebrovascular disease, but the full differential must span stroke subtypes and mimics.
Part 1 — Stroke Subtypes (What Type of Stroke?)
The first branch in the differential is ischemic vs. hemorrhagic, as management diverges completely.
A. Ischemic Stroke (~85% of all strokes)
Using the TOAST classification, the etiologic subtypes are:
| Subtype | Mechanism | Relevance to This Patient |
|---|---|---|
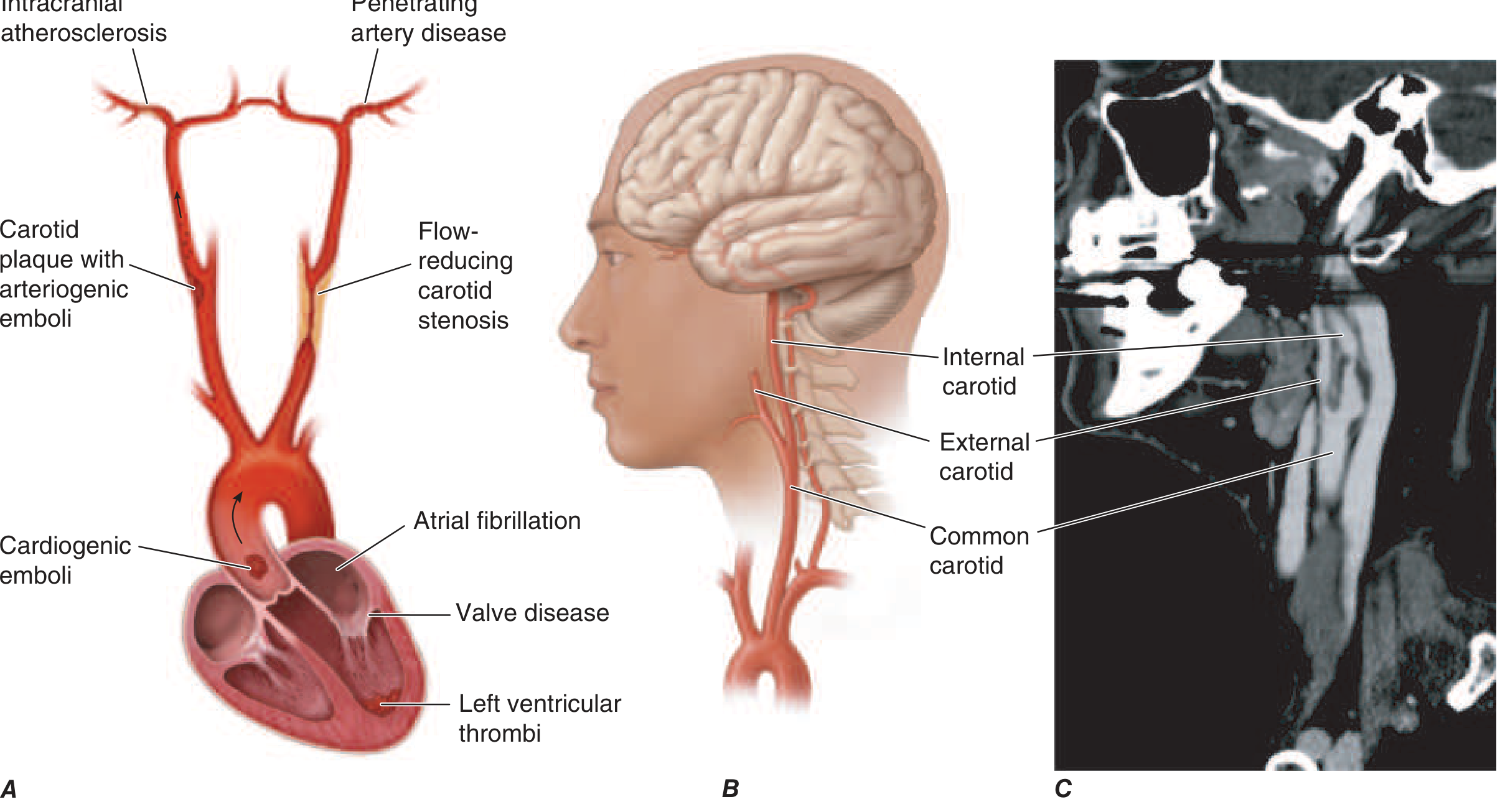
| Large-artery atherosclerosis | Carotid/vertebral stenosis → artery-to-artery embolism or flow reduction | Most likely — hypertension + hypercholesterolemia = classic atherosclerotic risk profile |
| Lacunar (small vessel) | Lipohyalinosis of penetrating arteries from chronic hypertension | Highly relevant — family Hx of HTN; presents as pure motor, pure sensory, or ataxic hemiparesis |
| Cardioembolic | Atrial fibrillation (most common), LV thrombus, valvular disease, cardiomyopathy | Must be excluded — AF accounts for ~20% of ischemic strokes; ECG mandatory |
| Other determined etiology | Hypercoagulable states (antiphospholipid syndrome, protein C/S deficiency), vasculitis, dissection | Less likely at 54 but should be considered if no clear atheroembolic cause |
| Cryptogenic (undetermined) | ~30% of strokes remain unexplained despite workup | Diagnosis of exclusion |
"Focus should be on atrial fibrillation and carotid atherosclerosis, because these etiologies have proven secondary prevention strategies." — Harrison's Principles of Internal Medicine 22E, p. 3487
B. Hemorrhagic Stroke (~15% of all strokes)
| Subtype | Key Features |
|---|---|
| Intracerebral hemorrhage (ICH) | Hypertension is the #1 cause; rupture of Charcot-Bouchard microaneurysms in basal ganglia, thalamus, pons, cerebellum |
| Subarachnoid hemorrhage (SAH) | Sudden onset "thunderclap" worst-of-life headache; rupture of saccular aneurysm |
| Subdural/Epidural hematoma | Trauma history; anticoagulant use; may mimic stroke |
Given the family history of hypertension, ICH from chronic hypertensive vasculopathy is a meaningful consideration.
Part 2 — Stroke Mimics (Rule Out First)
From Tintinalli's Emergency Medicine (Table 167-5), conditions that can present identically to stroke:
| Mimic | Distinguishing Feature |
|---|---|
| Hypoglycemia | Bedside glucose — must be excluded immediately before any intervention |
| Hypertensive encephalopathy (PRES) | Gradual onset, global dysfunction, headache, elevated BP, diffuse edema on imaging |
| Todd's paralysis (post-ictal) | Transient hemiparesis after seizure; seizures can themselves be caused by stroke |
| Complicated migraine | History of migraines, preceding aura — but new onset at 54 is a red flag |
| Brain tumor/abscess | Focal findings, may have subacute onset; detected on CT/MRI |
| Subdural hematoma | Trauma or anticoagulation history; crescentic hyperdensity on CT |
| Meningitis/encephalitis | Fever, neck stiffness, CSF analysis confirms |
| Demyelinating disease (MS) | Uncommon at 54 as new presentation; MRI white matter lesions |
| Wernicke's encephalopathy | Triad of ataxia, ophthalmoplegia, confusion; alcoholism/malnutrition hx |
| Conversion disorder | Non-anatomic deficits, normal imaging |
| Labyrinthitis / Ménière's | Predominantly vestibular; no other focal neurologic signs (can mimic cerebellar stroke) |
Part 3 — Risk Factor-Driven Priorities for This Patient
Given the specific profile:
| Risk Factor | Most Likely Diagnosis It Points To |
|---|---|
| Family Hx Hypertension | Lacunar infarct, ICH (hypertensive), carotid atherosclerosis |
| Family Hx Hypercholesterolemia | Large-artery atherosclerosis (carotid stenosis, intracranial atherosclerosis) |
| 54-year-old male | Atherosclerosis peaks in this demographic; atrial fibrillation also common |
Immediate Workup to Narrow the Differential
- Non-contrast CT head — first step: differentiates hemorrhagic from ischemic; rules out mass lesion
- Blood glucose (stat) — excludes hypoglycemia mimic
- ECG + cardiac telemetry — identifies AF as cardioembolic source
- MRI brain with DWI — most sensitive for acute ischemia; identifies lacunar vs. cortical patterns
- CT/MRI angiography — carotid and intracranial vessels; identifies stenosis or dissection
- Lipid panel, HbA1c, CBC, ESR, coagulation studies
- Echocardiogram — left atrial thrombus, patent foramen ovale, valvular disease
- Holter monitor / extended cardiac monitoring — paroxysmal AF
Summary Ranking for This Patient
- Atherothrombotic large-artery disease (carotid atherosclerosis) — most likely given HTN + hypercholesterolemia FHx
- Lacunar infarct (small vessel disease from chronic hypertension)
- Cardioembolic stroke (atrial fibrillation — must actively exclude)
- Hypertensive intracerebral hemorrhage — possible; excludes with CT
- Cryptogenic stroke — diagnosis of exclusion
- Stroke mimic — hypoglycemia, hypertensive encephalopathy — rule out immediately
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 3487; Tintinalli's Emergency Medicine, Table 167-5; Bradley and Daroff's Neurology in Clinical Practice, Stroke Etiology section.
Create a diagnostic flowchart for ischemic vs hemorrhagic vs mimic stroke
Generating Image
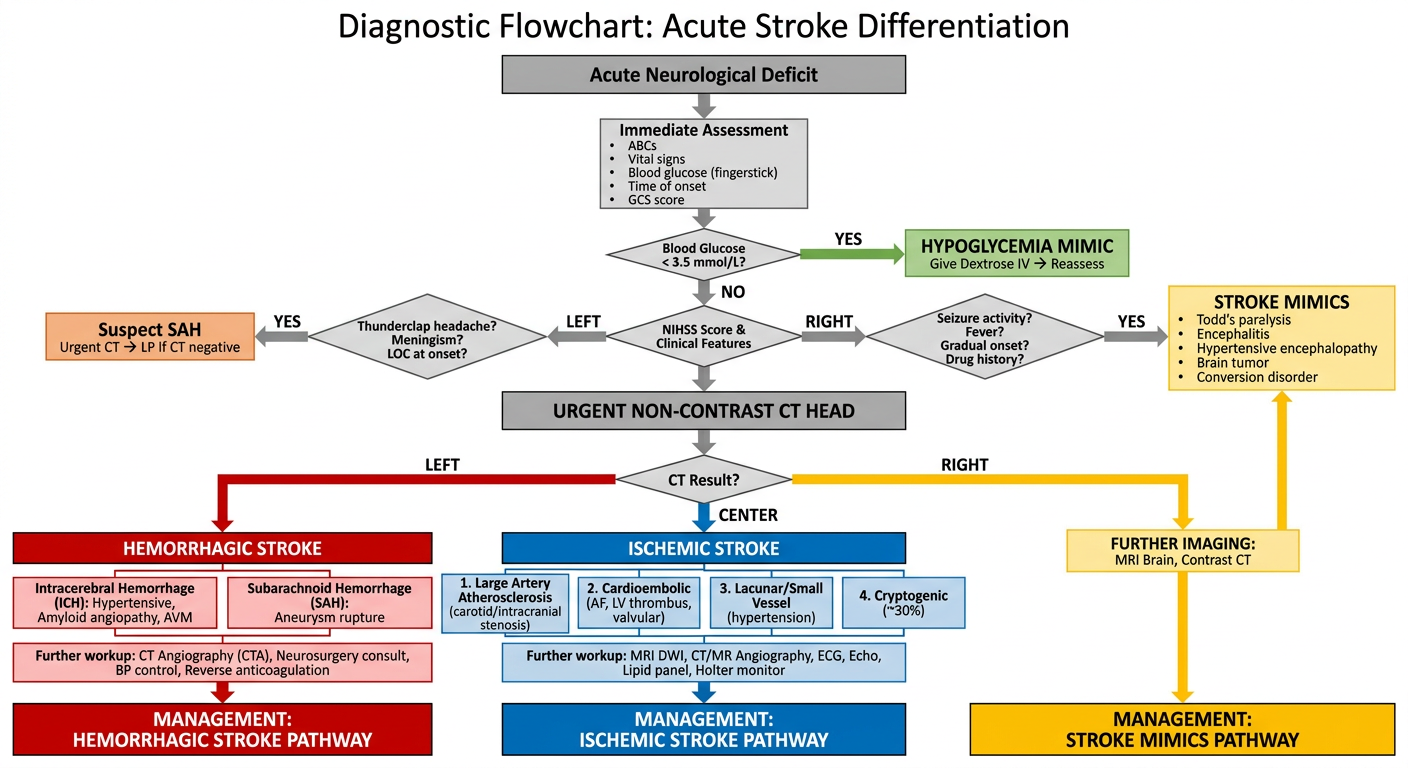
Here's the diagnostic flowchart. Here's how to read it:
Entry Point → Immediate Bedside Steps
Every patient with an acute neurological deficit gets an immediate triage: ABCs, vitals, fingerstick glucose, GCS, and time of onset documentation.
First Branch — Rule Out Mimics Early
- Hypoglycemia is eliminated first with a glucose check (fastest, cheapest mimic to reverse).
- Clinical red flags (thunderclap headache, seizure, fever, gradual onset) redirect toward SAH or other mimics before imaging.
Central Step — Non-Contrast CT Head
This is the mandatory pivot point. It separates:
| CT Finding | Diagnosis |
|---|---|
| Hyperdense blood (red) | Hemorrhagic stroke → ICH or SAH |
| No blood / early ischemic change (blue) | Ischemic stroke → further TOAST subtyping |
| Mass lesion / atypical (yellow) | Mimic → MRI ± contrast for tumor, abscess, MS |
Ischemic Arm drills down into the four TOAST subtypes (large-artery atherosclerosis, cardioembolic, lacunar/small vessel, cryptogenic), each requiring specific downstream workup (MRI DWI, CTA, ECG, echo, Holter).
Hemorrhagic Arm separates ICH from SAH and routes to neurosurgical consultation, BP management, and anticoagulation reversal.
Hey
Hey! How can I help you?
What is your name?
My name is Orris. I'm a knowledgeable AI assistant here to help you with questions across all domains — including medical, clinical, and general topics. What can I do for you?
This is a shared conversation. Sign in to Orris to start your own chat.