Q1 Nosocomial infection in ICU. Q2 ROLE of Nmethyl N Aspartate receptor in pain and gate control theory of pain. Answer these question for 10 marks each for dnb final anesthesia exam from standard source
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all the material needed for both comprehensive answers. Let me compile the complete, exam-ready responses.
Q1: Nosocomial (Hospital-Acquired) Infections in the ICU [10 Marks]
Source: Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e, Chapter 57 - Critical Care Medicine
Definition
A nosocomial infection (hospital-acquired infection / HAI) is one that develops 48 hours or more after hospital admission, or within 30 days of a surgical procedure, and was not present or incubating at the time of admission. In the ICU setting, these infections are largely unavoidable because of the nature of critical illness - patients have altered host defenses and require invasive devices.
Predisposing Factors in ICU Patients
- Host factors: Impaired immunity (critical illness, malnutrition, immunosuppression), extremes of age
- Invasive devices: Endotracheal tubes, central venous catheters (CVCs), urinary catheters - each creating a direct conduit bypassing normal host barriers
- Prolonged hospitalization: Duration of mechanical ventilation, ICU stay, and catheterization all increase risk
- Antibiotic pressure: Prior/prolonged broad-spectrum antibiotic use promotes emergence of resistant organisms (MRSA, Pseudomonas, Acinetobacter)
- Surgical stress: Anastomotic leaks, GI perforation, postoperative state
Types of Nosocomial Infections in ICU
1. Ventilator-Associated Pneumonia (VAP)
The most studied ICU-acquired infection. Tracheal intubation and mechanical ventilation significantly increase the risk of pneumonia.
Classification:
- Early-onset VAP (within 48-72 hours of intubation): caused by relatively antibiotic-sensitive oral flora - Haemophilus influenzae, Streptococcus pneumoniae, methicillin-sensitive S. aureus (MSSA). Associated with zero to low attributable mortality.
- Late-onset VAP (>72 hours): associated with virulent, drug-resistant organisms - MRSA, Pseudomonas aeruginosa, Acinetobacter. Associated with higher mortality.
Incidence & Mortality: Mortality ranges 30-70%; incidence >15% at 1 week and >20% at 2 weeks of mechanical ventilation in older studies.
Diagnosis (NHSN/CDC criteria):
- VAE (ventilator-associated event) surveillance requires no radiologic data to reduce subjectivity
- Invasive diagnosis: tracheal aspirate (preferred) or bronchoalveolar lavage (BAL)
- Quantitative thresholds: BAL ≥10^4 CFU/mL; protected brush specimen ≥10^3 CFU/mL
Prevention of VAP ("VAP Bundle"):
| Intervention | Evidence |
|---|---|
| Strict hand hygiene | Negligible risk, should be universal |
| Semirecumbent positioning (HOB ≥30°) | Simple, inexpensive, widely recommended |
| Subglottic suctioning endotracheal tubes | Meta-analysis supports reduction in VAP, shorter ICU stay |
| Selective digestive decontamination (SDD) | Growing evidence supports use |
| Oral decontamination with chlorhexidine | Likely reduces VAP incidence |
| Avoid routine acid suppression | Acid-suppressive therapy promotes gastric bacterial overgrowth; use only in high-risk patients |
Treatment: Ceftriaxone + azithromycin (early VAP); vancomycin + cefepime ± ciprofloxacin (late VAP/MRSA/MDR GNRs). Duration: 8 days (adequate for most; longer for Pseudomonas/Acinetobacter).
2. Catheter-Related Bloodstream Infection (CRBSI / CLABSI)
CDC Definition requires ALL of:
- Clinical suspicion of catheter-related infection (low likelihood of infection elsewhere)
- Positive blood culture drawn through the catheter or catheter segment
- Matching positive blood culture from a peripheral site
Attributable mortality: ~11%
Common organisms: S. epidermidis (most common, rarely true infection), S. aureus, enteric gram-negative bacteria, Pseudomonas, Acinetobacter, Enterococcus.
Prevention:
- Strict aseptic technique with full barrier precautions during insertion
- Chlorhexidine and silver sulfadiazine-coated, or rifampin/minocycline-coated catheters (effective after day 5-6; CDC recommends if expected duration >5 days and local CRBSI rate is high)
- Daily review of the need for continued catheterization
- Routine catheter guidewire exchange is NOT recommended
Management: Remove offending catheter + antibiotics for minimum 7 days (longer for S. aureus due to endocarditis risk). Use empiric vancomycin + broad-spectrum gram-negative coverage pending cultures.
3. Catheter-Associated Urinary Tract Infection (CAUTI)
- The second most common source of infection in the ICU; occurs in up to one-third of ICU patients
- Incidence increases with duration of bladder catheterization
- Bacteremia complicates ~5% of CAUTIs
- Organisms: Staphylococci, Enterococcus, enteric gram-negative bacteria, Pseudomonas
- Prevention: Careful aseptic technique during insertion, minimize catheterization duration, daily assessment of catheter necessity
4. Nosocomial Sinusitis
- Common in patients with indwelling oral and nasal tubes
- Nasotracheal intubation: ~95% radiographic sinusitis at 1 week
- Orotracheal intubation: ~25% radiographic sinusitis at 1 week
- Only ~10% of radiographic sinusitis is truly infected (by quantitative culture)
- May be responsible for 16% of fevers of unknown origin in surgical ICU
- Organisms: Same as VAP (Staphylococci, Pseudomonas, Acinetobacter)
- Prevention/Treatment: Semirecumbent positioning, avoid nasal tubes; nasal irrigation, decongestants; ENT consultation if no resolution in 2-3 days
5. Invasive Fungal Infections (Candida)
- Candida species cause the vast majority in non-neutropenic ICU patients
- Risk factors: CVCs, recent abdominal surgery/anastomotic leakage, dialysis, parenteral nutrition (PN), prolonged broad-spectrum antibiotics, corticosteroids
- Candida albicans accounts for ~50% of invasive Candida infections
- Diagnosis: Positive sterile fluid culture (gold standard; takes 72-96 hours, sensitivity ~50%); β-D-glucan assay (~80% sensitive and specific); PCR (>90% sensitivity, results in hours)
- Treatment: Echinocandins (caspofungin, micafungin, anidulafungin) are first-line in most ICU settings. Continue for at least 2 weeks after last positive blood culture. Remove intravascular catheters. Ophthalmologic exam for endophthalmitis.
- Prophylaxis: Fluconazole for high-risk patients only (not general use - promotes resistant species like C. glabrata, C. krusei)
Empiric Antibiotic Regimens (ICU)
| Infection | Regimen |
|---|---|
| Early VAP | Ceftriaxone + azithromycin (add vancomycin/linezolid if MRSA risk) |
| Late VAP/BSI | Vancomycin OR linezolid + cefepime ± ciprofloxacin (MDR GNRs/ESBLs: use meropenem) |
| Non-catheter UTI | Ceftriaxone |
| Catheter-associated UTI | Ceftazidime (add vancomycin if GPC on Gram stain; meropenem if MDR/ESBL) |
| C. difficile diarrhea | Oral vancomycin; add IV metronidazole if shock/megacolon/ileus |
| Sepsis (unknown source) | Vancomycin + meropenem ± ciprofloxacin |
| Hospital-acquired IAI | Vancomycin + piperacillin-tazobactam OR meropenem |
Note: Always tailor to local antibiogram and de-escalate once culture results are available.
General Principles of Prevention
- Hand hygiene - the single most effective measure
- Aseptic technique for all device insertions
- Bundle approach - bundles of care for VAP, CLABSI, CAUTI
- Antibiotic stewardship - appropriate antibiotic use to prevent resistance
- Minimize device duration - daily review of need for all invasive devices
- Infection surveillance - active monitoring through NHSN (CDC)
Q2: Role of NMDA Receptor in Pain & Gate Control Theory of Pain [10 Marks]
Sources: Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e; Eric Kandel - Principles of Neural Science, 6e; Neuroscience: Exploring the Brain, 5e
PART A: Role of the NMDA Receptor in Pain
Structure and Basic Pharmacology
The N-methyl-D-aspartate (NMDA) receptor is an ionotropic glutamate receptor found abundantly in the dorsal horn of the spinal cord. Key features:
- It is a ligand-gated ion channel permeable to Ca²+, Na⁺, and K⁺
- Requires two co-agonists for activation: glutamate (binds at the glutamate site) and glycine (binds at a co-agonist site)
- Under resting conditions, the channel is voltage-dependently blocked by Mg²+ ions - the channel only opens when the cell is sufficiently depolarized AND ligand-bound (coincidence detector)
- Blocked by ketamine and other NMDA antagonists
NMDA Receptors in Primary Nociceptive Transmission
Under normal conditions, NMDA receptors play a minimal role in primary pain transmission. As illustrated in Barash's Clinical Anesthesia (Figure 55-9):
- Primary nociceptive input is transmitted via AMPA receptors, neurokinin-1 (NK1) receptors, and calcitonin gene-related peptide (CGRP) synapses
- Glutaminergic NMDA synapses do NOT participate significantly in primary nociceptive transmission
- Even after complete NMDA blockade in the spinal cord, primary afferent nociceptive information is transmitted to the thalamus
- Therefore, NMDA antagonists have an antihyperalgesic rather than analgesic effect in the spinal cord
NMDA Receptors in Central Sensitization and Wind-Up
The critical role of NMDA receptors is in the development of pathological pain states:
Wind-Up:
- Repetitive C-fiber stimulation causes progressive amplification of dorsal horn neuron responses
- With each successive nociceptive input, increasing glutamate release progressively depolarizes the postsynaptic membrane
- Once the Mg²+ block is relieved by sufficient depolarization, NMDA receptors become activated
- This generates an explosive increase in intracellular Ca²+ triggering intracellular signaling cascades
Central Sensitization:
NMDA receptor activation in the dorsal horn leads to:
- Increased neuronal excitability (hyperalgesia - exaggerated pain response to noxious stimuli)
- Allodynia (pain from non-noxious stimuli)
- Expansion of receptive fields
- Long-term potentiation (LTP) - persistent changes in synaptic efficacy
- Facilitation of ongoing pain
Per Barash's (Chapter 55): "Preventing NMDA receptor activation in the dorsal horn... prevents wind-up, facilitation, central sensitization, expansion of receptive fields, and long-term potentiation, all of which can lead to a chronic pain state."
Microglia and astrocyte activation also contribute, further amplifying nociceptive signals (Principles of Neural Science, 6e).
Clinical Implications - Preventive Analgesia
The concept of preventive analgesia (formerly "preemptive analgesia") is directly based on NMDA receptor physiology:
- Goal: block the development of sustained pain by preventing NMDA-driven sensitization
- Three critical principles:
- Depth of analgesia must be adequate to block ALL nociceptive input
- Analgesic technique must cover the entire surgical field
- Duration must cover both surgical AND postsurgical periods
Ketamine is the prototypical NMDA receptor antagonist used clinically:
- Provides analgesia at subanesthetic blood concentrations
- Works primarily by preventing central sensitization and hyperalgesia rather than blocking primary pain transmission
- Reduces postoperative opioid requirements
- Particularly useful in opioid-tolerant patients and chronic pain patients
- IV ketamine: induction dose 1-2 mg/kg; analgesic infusion 1-2 μg/kg/hr in ICU
- Also used via intraspinal/extradural routes for chronic pain
PART B: Gate Control Theory of Pain (Melzack and Wall, 1965)
Historical Background
In 1965, Ronald Melzack and Patrick Wall (working at MIT) published their landmark paper: "Pain mechanisms: a new theory" in Science (150:971, 1965). This was a refinement of the earlier "pattern and specificity" concepts and represented the first mechanistic model explaining the modulation of pain.
Their observations in decerebrate and spinal cats showed that peripheral stimulation of large myelinated fibers (Aβ) could inhibit pain perception - the basis for the "gate" concept.
Neuroanatomical Basis
The gate operates in the dorsal horn of the spinal cord (substantia gelatinosa, Rexed laminae I, II, V):
Fibers involved:
- C fibers (unmyelinated, slow): nociceptive afferents, transmit burning/aching pain
- Aδ fibers (thinly myelinated): nociceptive, transmit sharp/fast pain
- Aβ fibers (large diameter, myelinated, fast): non-nociceptive mechanoreceptors (touch, vibration, pressure)
Neurons involved:
- Projection neurons (T cells - transmission cells): receive convergent input from both Aβ and C fibers; send signals up the anterolateral (spinothalamic) tract to the thalamus and cortex
- Inhibitory interneurons (in the substantia gelatinosa): the "gate keepers"
The Gate Mechanism
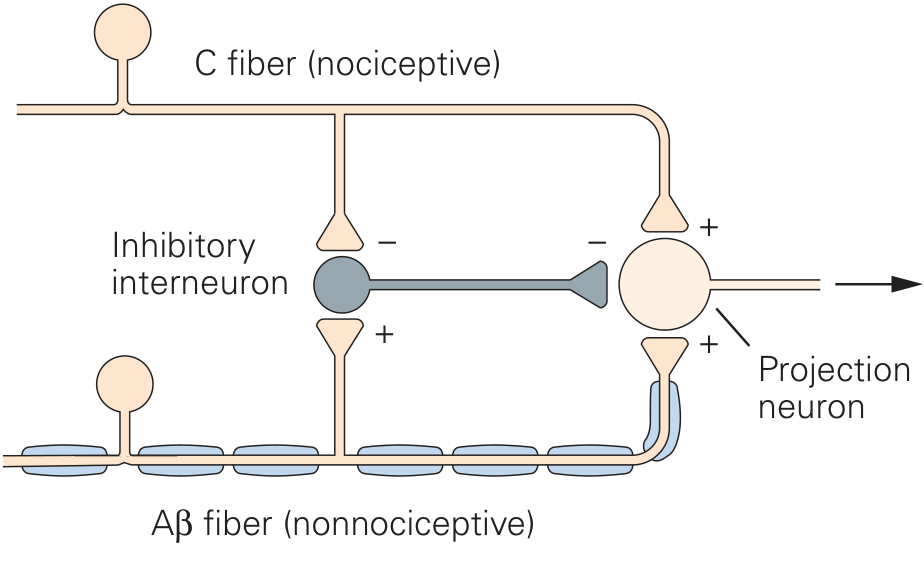
Figure: Gate Control Theory of Pain - Kandel, Principles of Neural Science 6e
When the Gate is OPEN (pain perceived):
- C fiber (nociceptive) activity predominates
- C fibers inhibit the inhibitory interneuron (indirect inhibition via interneuron)
- Inhibitory interneuron becomes inactive, releasing projection neuron from inhibition
- Projection neuron fires freely → pain signals ascend to brain
When the Gate is CLOSED (pain suppressed):
- Aβ fiber (non-nociceptive) activity predominates (e.g., rubbing injured skin, TENS)
- Aβ fibers excite the inhibitory interneuron
- Active inhibitory interneuron suppresses the projection neuron
- Projection neuron fires less → reduced pain transmission
In summary:
| Input | Effect on Interneuron | Effect on Projection Neuron | Gate |
|---|---|---|---|
| C fiber (nociceptive) predominance | Inhibited | Excited (less inhibition) | Open |
| Aβ fiber (non-nociceptive) predominance | Excited | Inhibited | Closed |
Modifications and Expanded Understanding
The original circuit has been refined over decades:
- Supraspinal modulation: Gate interactions also occur at many supraspinal relay centers, not just the spinal cord
- Descending inhibition: The periaqueductal gray (PAG) - periventricular gray matter sends inhibitory signals descending to the dorsal horn via the raphe nuclei and locus coeruleus, releasing endorphins, serotonin, and norepinephrine
- Multiple neurotransmitters modulate the dorsal horn gate: substance P (NK1 receptors), endorphins (μ-opioid receptors), norepinephrine (α2 receptors)
- Psychological/cognitive input: The brain itself can modulate the gate via descending pathways - explaining the analgesic effects of distraction, stress-induced analgesia in soldiers/athletes
Clinical Applications of Gate Control Theory
| Application | Mechanism |
|---|---|
| TENS (Transcutaneous Electrical Nerve Stimulation) | Activates large Aβ fibers → closes gate; useful in arthritis, tendonitis, bursitis, chronic pain |
| Spinal cord stimulation (SCS) | Dorsal column stimulation activates Aβ fibers → inhibits pain transmission |
| Rubbing an injury | Mechanoreceptor (Aβ) activation closes gate temporarily |
| Acupuncture | Postulated to activate Aβ and Aδ fibers to modulate gate |
| Opioids | Act on μ-opioid receptors on inhibitory interneurons and descending pathways |
| Local anesthetics (neuraxial) | Block all afferents including nociceptors |
Summary Table
| Feature | Gate Control Theory | NMDA Receptor in Pain |
|---|---|---|
| Location | Dorsal horn (substantia gelatinosa) | Dorsal horn (postsynaptic) |
| Key concept | Balance of Aβ vs. C fiber input determines pain | NMDA activation drives central sensitization |
| Gate "closed" by | Aβ fiber activation via inhibitory interneurons | NMDA antagonists (ketamine) |
| Gate "opened" by | C fiber/nociceptive fiber predominance | Repetitive C-fiber input, Mg²+ unblocking |
| Clinical use | TENS, SCS, rubbing skin | Ketamine infusion, preventive analgesia |
| Long-term effect | Explains modulation of acute pain | Explains wind-up, chronification of pain |
References
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - Chapters 19 (Ketamine), 55 (Acute Postoperative Pain), 57 (Critical Care Medicine)
- Eric Kandel - Principles of Neural Science, 6e - Chapter 20: Pain Perception
- Neuroscience: Exploring the Brain, 5e - Chapter 12: The Somatic Sensory System (Afferent Regulation)
- Melzack R, Wall PD. Pain mechanisms: a new theory. Science 1965;150:971.
This is a shared conversation. Sign in to Orris to start your own chat.