

IMG_1521.jpg
IMG_1522.jpg
44 years old lady presented with complaints of intermittent pain in the right lower abdomen. She gives history of laparoscopic ovarian cystectomy one and a half years back, which was reported as Serous cystadenofibroma, right ovary and Endometriotic cyst of left ovary. The histopathology slides could not be retrieved. Now, on examination -pelvic mass present. CT- Multiloculated cystic mass with solid areas, right adnexa. Underwent hysterectomy with bilateral salpingo-oophorectomy. Section from right ovary provided.
analyse_media
analyse_media
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"high grade serous carcinoma" ovary histopathology
Reading File
Finding Sources
Reading File
I now have all the information needed for a comprehensive analysis. Let me compile the complete pathology report.
Histopathological Analysis - Right Ovary
Microscopic Findings (H&E, both slides)
Slide 1 (IMG_1521) - Higher power:
- Dense solid/sheet-like growth of malignant epithelioid cells forming a cohesive nest
- Cells are large and polygonal with amphophilic to eosinophilic cytoplasm
- Marked nuclear pleomorphism - anisokaryosis with coarse, vesicular chromatin
- Prominent macronucleoli (cherry-red, centrally located) in virtually every cell
- Frequent mitotic figures including atypical/multipolar forms
- Multinucleated tumor giant cells present
- Background hemorrhage and focal single-cell necrosis (karyorrhectic debris)
Slide 2 (IMG_1522) - Lower power, showing invasion:
- Solid sheets of pleomorphic epithelioid cells infiltrating into fibromyxoid/desmoplastic stroma (visible on left)
- Same nuclear features: vesicular nuclei, macronucleoli, irregular nuclear membranes
- Highly atypical/multipolar mitotic figures (starburst pattern clearly visible)
- Sparse fibrovascular stroma traversing tumor sheets
- Scattered lymphocytic infiltrate in background
Diagnosis
High-Grade Serous Carcinoma (HGSC) of the Right Ovary
Diagnostic Criteria Met (per Robbins Pathologic Basis of Disease)
The histology is classic for HGSC:
- Complex growth with stromal effacement/infiltration
- Nuclear atypia: >3-fold variation in nuclear size (pleomorphism)
- >12 mitoses per 10 HPF (numerous mitoses visible)
- Atypical/multipolar mitotic figures
- Multinucleation
- Occasional areas where serous features are barely recognizable (solid undifferentiated growth)
As per Robbins: "High-grade serous carcinoma is distinguished by having more complex growth patterns and widespread infiltration or effacement of the underlying stroma. The individual tumor cells display marked nuclear atypia, including pleomorphism (three-fold variation of nuclear size), numerous mitotic figures (greater than 12 mitoses per 10 high-power fields), atypical mitotic figures, and multinucleation."
Clinicopathological Correlation
| Feature | This Case |
|---|---|
| Age | 44 years (typical HGSC age range) |
| Previous history | Serous cystadenofibroma right ovary + Endometriotic cyst left ovary |
| CT finding | Multiloculated cystic mass with solid areas - classic for HGSC |
| Histology | Solid growth, marked pleomorphism, macronucleoli, atypical mitoses |
| Likely origin | Fallopian tube fimbriae (STIC) or cortical inclusion cysts |
The prior serous cystadenofibroma is likely a separate benign diagnosis from 1.5 years ago. The current HGSC likely arose de novo from fallopian tube intraepithelial precursor (STIC pathway - Type II tumor), which is the dominant pathogenesis for sporadic HGSC. These are not "malignant transformation" of the prior benign cyst - HGSC arises directly from high-grade intraepithelial precursors, not through the low-grade pathway.
The background endometriosis (left ovary, prior surgery) may also be relevant - there is a well-established association between endometriosis and clear cell and endometrioid carcinoma, but HGSC can coexist.
Differential Diagnosis Considered and Excluded
| Entity | Against it |
|---|---|
| Low-grade serous carcinoma | Mild atypia, psammoma bodies, KRAS/BRAF mutations - not this pattern |
| Undifferentiated carcinoma | Overlaps with HGSC; IHC would help |
| Adult granulosa cell tumor | Nuclear grooves ("coffee bean"), Call-Exner bodies - not seen |
| Dysgerminoma | Lymphocytic stroma, fibrous septa, younger patients |
| Metastatic carcinoma | No primary elsewhere suggested; bilateral pattern not shown |
| Melanoma | No clinical history; but IHC needed to exclude |
Recommended IHC Panel
| Marker | Expected in HGSC |
|---|---|
| WT1 | Diffusely positive (strong) |
| PAX8 | Positive (Mullerian lineage) |
| p53 | Aberrant (diffuse strong OR complete null pattern - TP53 mutation) |
| p16 | Block-positive (diffuse) |
| CK7 | Positive |
| ER/PR | Variable (often focally positive) |
| Ki-67 | High (>70%) |
| Negative: CK20, CDX2, S100, HMB45, inhibin |
The p53 aberrant pattern (either diffuse 3+ or null/absent) is the single most useful marker - present in virtually 100% of HGSC cases due to TP53 mutations. Combined WT1+/PAX8+/p53 aberrant is essentially diagnostic of HGSC.
Staging Workup (Post-Surgery)
Staging is surgical per FIGO 2014:
- Gross examination of omentum, peritoneal surfaces, and lymph nodes intraoperatively was essential
- Ascites cytology (if present) should be submitted
- BRCA1/BRCA2 germline testing strongly recommended (therapeutic implications - PARP inhibitors)
- Somatic tumor BRCA testing also recommended
Clinical Significance
HGSC is the most common and most lethal ovarian malignancy (~70% of all ovarian carcinomas). The solid growth pattern seen here, while part of the HGSC morphologic spectrum, can occasionally represent a more aggressive subclone. The prior laparoscopic surgery 1.5 years ago raises the important question of whether any occult malignancy was present at that time (given slides are unavailable for review) - though the prior diagnosis of serous cystadenofibroma is benign and would be a distinct entity.
References:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), pp. 941-943 - HGSC morphology and pathogenesis
- Robbins & Kumar Basic Pathology - Serous carcinoma of ovary, fallopian tube origin
Refer to who and teach me highgrade serous carcinoma
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Searching PubMed
"high grade serous carcinoma" ovary TP53 BRCA treatment
I now have all the textbook content and images needed. Here is a complete structured teaching session on High-Grade Serous Carcinoma, drawn directly from Robbins, Cotran & Kumar Pathologic Basis of Disease and Berek & Novak's Gynecology.
High-Grade Serous Carcinoma (HGSC) of the Ovary
As taught by Robbins Pathologic Basis of Disease & Berek & Novak's Gynecology
1. WHO Classification - Where Does HGSC Fit?
Robbins, Cotran & Kumar - TABLE 22.3 WHO Classification of Ovarian Neoplasms
| Category | Types |
|---|---|
| Surface Epithelial-Stromal Tumors | Serous (Benign / Borderline / Malignant: Low-grade & High-grade) |
| Mucinous, Endometrioid, Clear Cell, Brenner | |
| Sex Cord-Stromal | Granulosa cell, Fibrothecoma, Sertoli-Leydig |
| Germ Cell | Teratoma, Dysgerminoma, Yolk sac |
| Metastatic | Colonic, Gastric, Breast, etc. |
HGSC is a malignant surface epithelial-stromal tumor of serous type. It is the most common and deadliest ovarian malignancy.
"Most of the malignant epithelial tumors are high-grade serous carcinomas, which have a poor prognosis in large part because they are usually detected after they have spread beyond the ovary and/or the fallopian tube."
- Robbins, Cotran & Kumar
2. The Type I vs Type II Concept (The Two-Pathway Model)
This is the conceptual backbone. Look at the diagram:
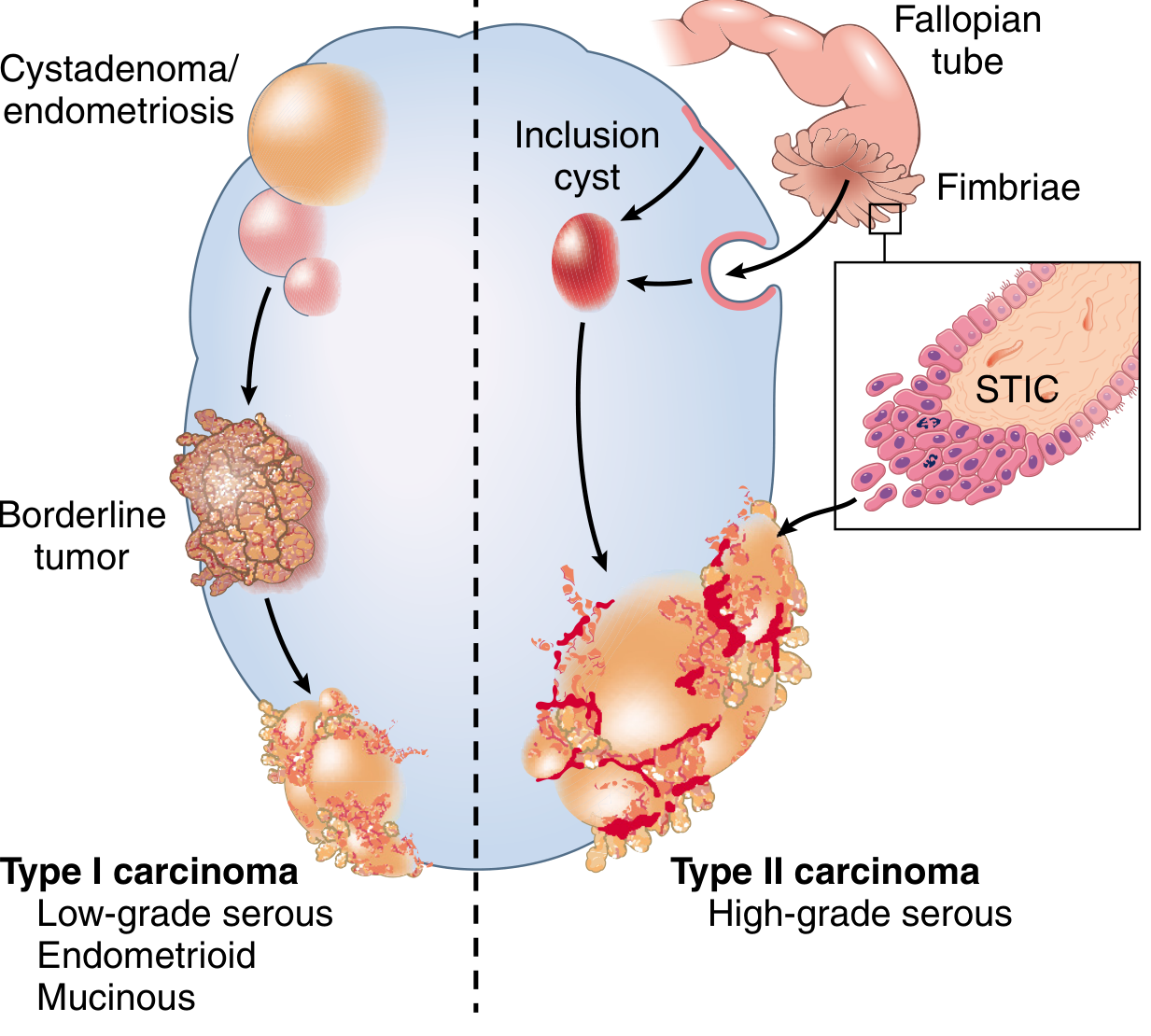
| Feature | Type I | Type II = HGSC |
|---|---|---|
| Precursor | Cystadenoma → Borderline | Serous Tubal Intraepithelial Carcinoma (STIC) |
| Grade | Low-grade | High-grade |
| Mutations | KRAS, BRAF, PTEN, CTNNB1 | TP53 (>96%), BRCA1/2 |
| Genomic stability | Relatively stable | Highly unstable |
| Progression | Slow (years) | Rapid |
| At diagnosis | Usually confined | Usually widespread |
| Examples | Low-grade serous, endometrioid, mucinous | High-grade serous |
3. Origin and Pathogenesis
The Fallopian Tube Origin - STIC
Robbins:
"Serous tubal intraepithelial carcinoma (STIC) lesions...have since been described in association with sporadic high-grade serous ovarian cancers, suggesting that at least some high-grade serous carcinomas arise from the fallopian tube."
The sequence is:
- Normal secretory cells of fallopian tube fimbriae acquire TP53 mutation
- → p53 signature (subclinical atypia)
- → STIC (morphologically malignant cells, no invasion yet)
- → STIC cells exfoliate and implant on ovary surface / peritoneum
- → Cortical inclusion cysts form on ovary → frank HGSC
Why Does This Matter Clinically?
- Risk-reducing bilateral salpingo-oophorectomy (RRSO) in BRCA carriers must include the tube
- Risk-reducing salpingectomy alone is being studied as a fertility-sparing option
- Prophylactic salpingo-oophorectomy in BRCA1/2 carriers revealed STIC as the "smoking gun"
Molecular Alterations in HGSC
| Gene | Alteration | Significance |
|---|---|---|
| TP53 | Mutation (>96% of cases) | Diffuse/null p53 on IHC; hallmark of HGSC |
| BRCA1 | Germline/somatic mutation | ~15% germline; homologous recombination defect |
| BRCA2 | Germline/somatic mutation | Therapeutic target (PARP inhibitors) |
| PIK3CA | Amplification | Signaling pathway |
| RB | Deletion | Cell cycle dysregulation |
| KRAS/BRAF | Absent | Distinguishes from low-grade serous |
4. Epidemiology & Risk Factors
(Robbins, Cotran & Kumar, p. 941)
-
Peak age: 55-65 years (postmenopausal); can occur in 40s
-
Risk factors:
- Nulliparity
- Family history of breast/ovarian cancer
- BRCA1 germline mutation: 20-60% lifetime risk of ovarian cancer by age 70
- BRCA2 germline mutation: lower but significant ovarian risk
- BRCA1 mutations present in ~5% of patients under age 70
-
Protective factors:
- Oral contraceptive use
- Tubal ligation
- Multiparity
- Salpingectomy (by removing the site of STIC origin)
5. Gross Morphology
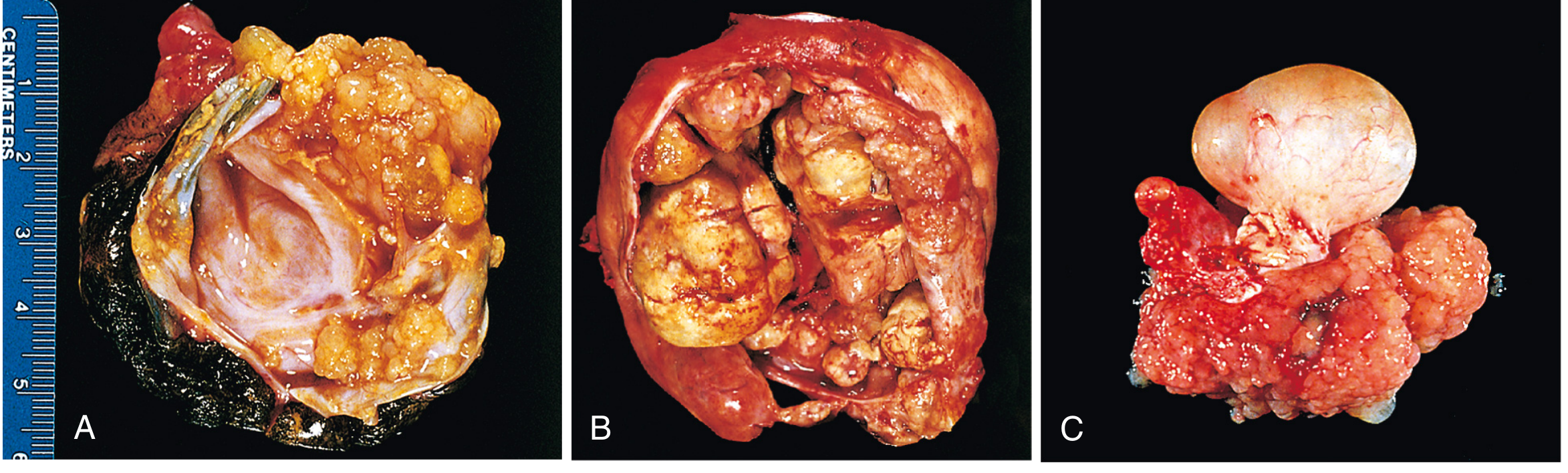
HGSC gross features:
- Multiloculated cystic mass with solid areas (exactly as in this case's CT)
- Papillary excrescences inside cysts and on surface
- Capsular fixation, nodularity - signs of malignancy
- Necrosis and hemorrhage in solid areas
- Bilaterality in ~66% of serous carcinomas (vs 20% benign, 30% borderline)
- Frequently with peritoneal studding, omental "cake," ascites
6. Microscopic Morphology - The Key to Diagnosis
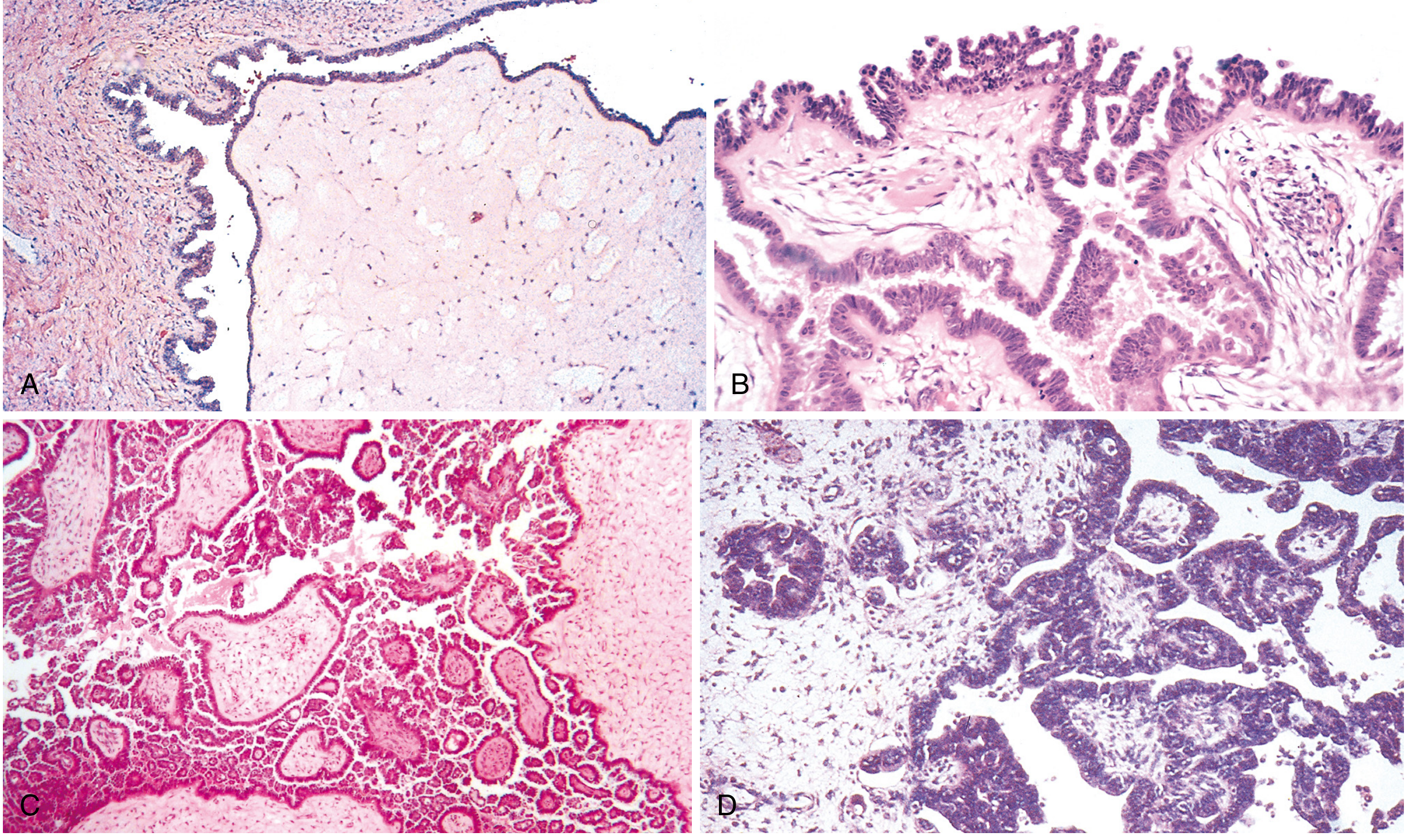
Diagnostic Criteria for HGSC (Robbins + Berek & Novak)
| Feature | Description |
|---|---|
| Growth pattern | Solid sheets, papillary, glandular - often effacement of underlying stroma |
| Nuclear pleomorphism | >3-fold variation in nuclear size (anisokaryosis) |
| Mitoses | >12 mitoses per 10 HPF |
| Atypical mitoses | Multipolar, ring, tripolar forms - seen in your slides |
| Multinucleation | Tumor giant cells |
| Macronucleoli | Prominent eosinophilic "cherry-red" nucleoli |
| Stromal invasion | Essential - differentiates from borderline |
| Psammoma bodies | Laminated calcifications, found in ~80% of serous carcinomas |
| Desmoplasia | Fibrous stromal response at invasion front |
Berek & Novak:
"In malignant serous tumors, stromal invasion is present. High-grade neoplasms are characterized by solid sheets of cells, nuclear pleomorphism, and high mitotic activity."
7. Grading System
HGSC uses the binary grading system (Malpica/MD Anderson), not the 3-tier FIGO system:
| Low-Grade Serous Carcinoma | High-Grade Serous Carcinoma | |
|---|---|---|
| Nuclear atypia | Mild-moderate | Severe, marked |
| Mitoses per 10 HPF | <12 | >12 |
| Architecture | Papillary, glandular | Solid sheets predominate |
| TP53 mutation | Absent | Present (>96%) |
| BRCA | Absent | Frequent |
| Psammoma bodies | More common | Present but fewer |
| Prognosis | Relatively indolent (but chemo-resistant) | Aggressive but initially chemo-sensitive |
8. Immunohistochemistry Profile
| Marker | HGSC Result | Significance |
|---|---|---|
| WT1 | Diffuse strong + | Best marker for serous differentiation |
| PAX8 | Positive | Mullerian origin |
| p53 | Aberrant (diffuse 3+ OR null/absent) | Reflects TP53 mutation - most specific |
| p16 | Block-positive (diffuse) | Correlates with high-grade |
| CK7 | Positive | Epithelial, not colonic |
| CK20 | Negative | Excludes colonic metastasis |
| ER/PR | Variable (often focally +) | |
| Ki-67 | >70% | High proliferation index |
| Inhibin | Negative | Excludes granulosa cell tumor |
| S100/HMB45 | Negative | Excludes melanoma |
The single most useful IHC marker: p53 aberrant pattern + WT1 positivity = essentially diagnostic of HGSC in the right context.
9. Clinical Course and Spread
Robbins:
"High-grade tumors are often widely metastatic throughout the abdomen at the time of presentation, a picture associated with rapid clinical deterioration."
Routes of Spread
- Transcoelomic (dominant): Exfoliation of tumor cells → peritoneal seeding → omental cake, diaphragmatic implants, bowel surface nodules
- Lymphatic: Para-aortic and pelvic nodes
- Hematogenous (late): Liver parenchyma, lungs, pleura
FIGO Staging (surgical)
| Stage | Description | 5-Year Survival |
|---|---|---|
| I | Confined to ovary/tube | ~70-90% |
| II | Pelvic extension | ~55-70% |
| III | Peritoneal implants / retroperitoneal nodes | ~20-40% |
| IV | Distant metastases (liver parenchyma, pleura) | <10% |
Robbins: 5-year survival for malignant tumor confined to ovary: 70%; with peritoneal spread: ~25%
Most patients present with Stage III disease - which is why early detection remains an unmet challenge.
10. Tumor Markers
| Marker | Role |
|---|---|
| CA-125 | NOT for screening; used to monitor response to treatment and recurrence |
| HE4 | Better specificity than CA-125, used with ROMA score |
| BRCA1/2 | Germline testing - all HGSC patients should be offered testing |
Robbins: "The serum marker CA-125 is used in patients with known disease to monitor disease recurrence/progression." No marker has sufficient sensitivity/specificity for population screening.
11. Treatment Principles
| Component | Details |
|---|---|
| Primary surgery | Cytoreductive surgery (debulking) - TAH + BSO + omentectomy + peritoneal biopsies + lymph node sampling |
| Goal of surgery | Optimal debulking = residual disease <1cm (ideally R0) |
| Chemotherapy | Carboplatin + Paclitaxel (6 cycles) - first-line standard |
| BRCA+ patients | PARP inhibitors (Olaparib, Niraparib, Rucaparib) - maintenance therapy after platinum response |
| Bevacizumab | Anti-VEGF, added to chemo in advanced/high-risk disease |
| Recurrence | Platinum-sensitive vs platinum-resistant determines second-line options |
12. Prognosis Determinants
- FIGO stage - most important
- Residual disease after debulking - R0 vs R1 vs R2
- BRCA1/2 mutation status - paradoxically better prognosis (more chemo-sensitive, PARP inhibitor benefit)
- Platinum sensitivity - responses beyond 6 months = platinum-sensitive
- Performance status
Summary Mnemonic - "HGSC STAMP"
- S - Serous, Solid sheets, STIC origin
- T - TP53 mutation (>96%), Tubal origin
- A - Atypical mitoses, Advanced stage at presentation
- M - Macronucleoli, Marked pleomorphism, >12 Mitoses/10HPF
- P - PARP inhibitors (BRCA+), Poor prognosis (Stage III/IV most common)
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), pp. 940-945 - Epithelial Ovarian Tumors
- Berek & Novak's Gynecology, Chapter 39 - Serous Carcinomas of the Ovary
Generate a histology quiz on HGSC vs borderline serous tumor findings
Finding Sources
Finding Sources
Reading File
Reading File
I have all the source material needed. Here is your complete quiz, built entirely from Robbins and Berek & Novak.
🔬 Histology Quiz: HGSC vs Borderline Serous Tumor
Based on Robbins, Cotran & Kumar & Berek & Novak's Gynecology
20 Questions | MCQ + True/False + Short Answer | Answers with explanations at the end
SECTION A - Multiple Choice Questions (1 mark each)
Q1. A 38-year-old woman undergoes ovarian cystectomy. Histology shows complex papillary fronds with hierarchical branching, pseudostratification of columnar epithelium, mild nuclear atypia, and detached cell clusters. The basement membrane separating epithelium from stroma is intact. What is the diagnosis?
- A) Serous cystadenoma
- B) High-grade serous carcinoma
- C) Serous borderline tumor
- D) Low-grade serous carcinoma
- E) Endometrioid carcinoma
Q2. Which of the following is the single most critical histological feature that distinguishes serous carcinoma from a serous borderline tumor?
- A) Nuclear pleomorphism
- B) Psammoma bodies
- C) Destructive stromal invasion
- D) Papillary architecture
- E) Detached cell clusters
Q3. On high-power examination of an ovarian tumor, you count 15 mitoses per 10 HPF, see multinucleated giant cells, and find >3-fold variation in nuclear size. The stroma is being infiltrated and effaced by solid sheets of cells. What is the diagnosis?
- A) Serous borderline tumor with microinvasion
- B) Low-grade serous carcinoma
- C) High-grade serous carcinoma
- D) Adult granulosa cell tumor
- E) Undifferentiated endometrial carcinoma
Q4. According to Berek & Novak, which of the following is NOT a diagnostic criterion for a serous borderline tumor?
- A) Epithelial hyperplasia with pseudostratification and tufting
- B) Mild nuclear atypia and mildly increased mitotic activity
- C) Detached cell clusters
- D) Destructive stromal invasion
- E) Absence of tissue destruction at the stromal interface
Q5. A serous borderline tumor with micropapillary features differs from a usual borderline tumor in which way?
- A) It shows destructive stromal invasion
- B) It has a higher mitotic count (>12/10 HPF)
- C) It is more frequently bilateral, exophytic, and high-stage
- D) It has TP53 mutations
- E) It arises from STIC lesions in the fallopian tube
Q6. The mutation pattern in HGSC is best described as:
- A) KRAS and BRAF mutations with TP53 wild-type
- B) CTNNB1 and PTEN mutations
- C) TP53 mutation (>96%) with frequent BRCA1/2 alterations
- D) MLH1 and MSH2 mismatch repair deficiency
- E) KRAS mutation in >85% of cases
Q7. On IHC, a high-grade serous carcinoma shows which of the following p53 patterns?
- A) Focal weak positivity in <10% of cells (wild-type pattern)
- B) Cytoplasmic positivity only
- C) Negative staining for p53 throughout (wild-type)
- D) Either diffuse strong positivity (3+) OR complete absence of staining (null pattern)
- E) Patchy moderate positivity in ~40% of cells
Q8. Which combination of IHC markers is most specific for confirming HGSC in an ovarian tumor?
- A) CK20+, CDX2+, CK7-
- B) Inhibin+, Calretinin+, p53 wild-type
- C) S100+, HMB45+, Melan-A+
- D) WT1+, PAX8+, p53 aberrant (diffuse or null)
- E) CK5/6+, p40+, p63+
Q9. A serous borderline tumor spreads to the peritoneum forming "noninvasive implants." According to Berek & Novak, what does this finding mean for the diagnosis?
- A) It automatically upgrades the diagnosis to high-grade serous carcinoma
- B) It confirms low-grade serous carcinoma at Stage III
- C) It does not change the diagnosis - the primary tumor histology determines the diagnosis
- D) It requires neoadjuvant chemotherapy before restaging
- E) It represents hematogenous spread
Q10. Psammoma bodies are:
- A) Pathognomonic of HGSC only
- B) Never found in borderline tumors
- C) Laminated calcified concentric structures found in ~80% of serous carcinomas, also seen in borderline tumors
- D) A sign of stromal invasion
- E) Found exclusively in mucinous tumors
Q11. A 35-year-old woman is found to have a serous ovarian tumor. Histology shows invasive implants in the omentum that resemble well-differentiated serous carcinoma with atypical cells forming irregular glands with sharp borders. The primary ovarian tumor shows borderline features. What is the clinical significance?
- A) This is normal peritoneal spread of borderline tumor with no added risk
- B) These invasive implants represent low-grade serous carcinoma and behave more aggressively (5-year OS ~50%)
- C) This confirms HGSC origin with peritoneal spread
- D) This is a Krukenberg tumor pattern
- E) This means BRCA testing is mandatory
Q12. Which of the following growth patterns is most characteristic of HGSC compared to borderline serous tumor?
- A) Hierarchical papillary branching with open stroma
- B) Simple cyst lining with ciliated cells
- C) Micropapillary structures without stromal cores
- D) Solid sheets of cells with effacement/infiltration of the underlying stroma
- E) Cribriform glands without nuclear atypia
SECTION B - True or False (1 mark each; correct the false statement)
Q13. Borderline serous tumors with spread beyond the ovary always represent malignant carcinoma and must be treated as Stage III HGSC.
Q14. High-grade serous carcinoma shows >3-fold variation in nuclear size and more than 12 mitoses per 10 high-power fields.
Q15. HGSC most commonly arises from the stepwise malignant transformation of a serous cystadenoma, just like low-grade serous carcinoma.
Q16. Bilaterality occurs in approximately 66% of serous carcinomas, compared to only 20% of benign serous cystadenomas.
Q17. A serous borderline tumor may safely be diagnosed even when the patient has peritoneal implants, as long as the primary ovarian tumor shows no destructive stromal invasion on histology.
SECTION C - Short Answer / Spot the Feature (2 marks each)
Q18. List FOUR histological criteria for diagnosing a serous borderline tumor as defined by Berek & Novak.
Q19. A pathologist describes the following findings on an ovarian biopsy:
"Solid nests and sheets of large pleomorphic cells infiltrating fibrotic stroma. Nuclei are vesicular with prominent macronucleoli. Atypical multipolar mitotic figures are easily identified. Occasional multinucleated giant cells present. No glandular lumina formed."
a) What is the diagnosis?
b) Name THREE IHC markers you would order and state the expected result for each.
c) What molecular alteration is present in >96% of such tumors?
Q20. Fill in the comparison table:
| Feature | Borderline Serous Tumor | HGSC |
|---|---|---|
| Stromal invasion | ? | ? |
| Nuclear atypia | ? | ? |
| Mitoses per 10 HPF | ? | ? |
| TP53 mutation | ? | ? |
| Precursor/origin | ? | ? |
| Typical age | ? | ? |
| 5-year survival (confined to ovary) | ? | ? |
✅ ANSWER KEY WITH EXPLANATIONS
A1. C - Serous borderline tumor
Classic Berek & Novak criteria: complex papillae + pseudostratification + mild atypia + detached clusters + no stromal invasion. Age under 40 is a clue (50% of borderline tumors occur before age 40).
A2. C - Destructive stromal invasion
Per Robbins: borderline tumors show all forms of epithelial complexity but lack stromal invasion. Berek & Novak explicitly states "absence of destructive stromal invasion" as a required criterion for borderline. Everything else (atypia, papillae, psammoma bodies) can appear in both.
A3. C - High-grade serous carcinoma
The triad of: (1) >12 mitoses/10 HPF, (2) >3-fold nuclear size variation, and (3) stromal effacement with solid sheets = Robbins' diagnostic criteria for HGSC. Multinucleated giant cells are also a HGSC feature.
A4. D - Destructive stromal invasion
This is what is absent in borderline tumors - it is the defining feature of carcinoma, not a criterion for borderline. The four Berek & Novak criteria are: epithelial hyperplasia, mild atypia/mitoses, detached clusters, and absence of destructive invasion.
A5. C - More frequently bilateral, exophytic, and high-stage
Per Berek & Novak: micropapillary variant borderline tumors do NOT have stromal invasion or TP53 mutations - they are still borderline. But they tend to be exophytic and present at higher stage more often than usual borderline tumors.
A6. C - TP53 mutation (>96%) with frequent BRCA1/2 alterations
Per Robbins: "High-grade tumors have a high frequency of TP53 mutations and lack mutations in either KRAS or BRAF." KRAS/BRAF are Type I (low-grade) mutations. This distinction is diagnostically and therapeutically critical.
A7. D - Diffuse strong (3+) OR complete absence (null pattern)
Both patterns represent aberrant p53 due to TP53 mutation. A missense mutation → protein accumulates → diffuse 3+. A nonsense/frameshift/splice mutation → no protein → null/absent. The normal "wild-type" pattern is heterogeneous moderate staining in ~40-60% of cells.
A8. D - WT1+, PAX8+, p53 aberrant
WT1 marks serous Mullerian differentiation. PAX8 marks Mullerian origin. Aberrant p53 confirms TP53 mutation = HGSC. Option A = colorectal. Option B = sex cord-stromal. Option C = melanoma. Option E = squamous cell carcinoma.
A9. C - Primary tumor histology determines the diagnosis
Per Berek & Novak: "Up to 40% of serous borderline tumors are associated with spread beyond the ovary, but high-stage disease does not necessarily warrant a diagnosis of an invasive carcinoma. The diagnosis...is based on the histologic features of the primary tumor."
A10. C - Laminated calcified concentric structures found in ~80% of serous carcinomas
Per Berek & Novak: psammoma bodies are found in ~80% of serous carcinomas. They also occur in borderline tumors. They are not restricted to HGSC, not a sign of invasion, and not pathognomonic.
A11. B - Invasive implants represent low-grade serous carcinoma with ~50% 5-year OS
Per Berek & Novak: "Up to 10% of women with ovarian serous borderline tumors and extraovarian implants may have invasive implants (i.e., low-grade serous carcinoma), and these can behave more aggressively. The 5-year overall survival...is about 50%." These are low-grade, not high-grade carcinoma.
A12. D - Solid sheets with effacement/infiltration of stroma
Per Robbins: "High-grade serous carcinoma is distinguished by having more complex growth patterns and widespread infiltration or effacement of the underlying stroma." Borderline shows hierarchical papillae with intact stroma.
A13. FALSE
Per Berek & Novak: "up to 40% of serous borderline tumors are associated with spread beyond the ovary, but high-stage disease does not necessarily warrant a diagnosis of an invasive carcinoma." The diagnosis is based on the primary ovarian tumor histology, not the stage.
A14. TRUE
Per Robbins: diagnostic criteria for HGSC include pleomorphism with >3-fold variation in nuclear size AND >12 mitoses per 10 HPF, along with atypical mitoses and multinucleation.
A15. FALSE
HGSC is a Type II tumor that arises directly from STIC lesions in the fallopian tube fimbriae (or cortical inclusion cysts). It does NOT follow the stepwise cystadenoma → borderline → carcinoma pathway. That is the Type I pathway leading to low-grade serous carcinoma. HGSC bypasses the borderline stage entirely.
A16. TRUE
Per Robbins: "Bilaterality is common, occurring in 20% of benign serous cystadenomas, 30% of serous borderline tumors, and approximately 66% of serous carcinomas."
A17. TRUE
Per Berek & Novak: the diagnosis of borderline vs. carcinoma is based on the histological features of the primary ovarian tumor. If the primary shows no destructive stromal invasion, it remains a borderline diagnosis even with peritoneal spread - though invasive implants would reclassify it to low-grade serous carcinoma.
A18. Four Berek & Novak criteria for serous borderline tumor:
- Epithelial hyperplasia - pseudostratification, tufting, cribriform, and micropapillary architecture
- Mild nuclear atypia and mild increased mitotic activity
- Detached cell clusters
- Absence of destructive stromal invasion
A19.
-
a) High-Grade Serous Carcinoma (HGSC)
-
b) IHC panel:
| Marker | Expected Result |
|---|---|
| WT1 | Diffuse strong positive |
| p53 | Aberrant - diffuse 3+ OR null/absent |
| PAX8 | Positive |
| Ki-67 | High (>70%) |
- c) TP53 mutation - present in >96% of HGSC cases; reflected as aberrant p53 IHC pattern
A20. Comparison table completed:
| Feature | Borderline Serous Tumor | HGSC |
|---|---|---|
| Stromal invasion | Absent | Present (infiltrative/effacing) |
| Nuclear atypia | Mild | Marked (>3-fold size variation) |
| Mitoses per 10 HPF | Mild increase | >12, with atypical forms |
| TP53 mutation | Absent | >96% of cases |
| Precursor/origin | Cystadenoma → stepwise (Type I) | STIC in fallopian tube (Type II) |
| Typical age | <40 years (50% of cases) | 55-65 years |
| 5-year survival (confined) | ~100% | ~70% |
Sources: All questions derived directly from Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), pp. 940-945, and Berek & Novak's Gynecology, Chapter 39 (Serous Carcinomas and Borderline Tumors of the Ovary).
This is a shared conversation. Sign in to Orris to start your own chat.