What can you do
Here's what I can do for you:
Research & Information
- Answer questions across medicine, science, law, history, tech, finance, and more
- Search the web for current events and up-to-date information
- Search PubMed for peer-reviewed medical literature and clinical guidelines
- Access a medical textbook library for clinical/pharmacology/anatomy questions
Document & File Work
- Word (.docx) - create, edit, format professional documents
- PowerPoint (.pptx) - build slide decks and presentations
- Excel (.xlsx) - create/edit spreadsheets, formulas, charts
- PDF - read, extract text, merge, split, watermark, OCR
Medical & Clinical
- Look up drugs, diagnoses, mechanisms, procedures, physiology
- Search medical textbooks for detailed clinical content
- Find recent studies and systematic reviews via PubMed
- Retrieve medical images (microscopy, anatomy, diagrams) from textbooks
Tax & Accounting (India)
- Indian income tax, direct taxes, transfer pricing (CA Bhanwar Borana materials)
- GST, indirect taxes, CA Final, ACCA prep (Navkar Institute materials)
Images & Media
- Generate original images, posters, diagrams, flashcards, postcards
- Analyze and describe uploaded images or videos
- Fetch and display images from URLs
Code & Computation
- Write and execute code (Python, JavaScript, shell, and more)
- Run calculations, data analysis, file processing
- Build scripts and automation tools
Specialized Skills
- Orthopaedic hip surgery database (surgical videos + clinical guidelines)
- Citation management and PubMed literature reviews
What would you like to work on?
What is trench foot
Reading File
Searching the Web
trench foot pathophysiology treatment clinical
Finding Sources
Reading File
Reading File
Trench Foot (Immersion Foot)
What Is It?
Trench foot - also called immersion foot - is a non-freezing cold injury caused by prolonged exposure of the feet to wet, cold, and often unsanitary conditions. The feet do not need to freeze; temperatures around 5-8°C combined with moisture are enough to cause serious damage.
The name comes from World War I, where soldiers on the Western Front stood in cold, waterlogged trenches for days, killing approximately 75,000 British soldiers. It continues to affect homeless populations, festival-goers, fishermen, and outdoor workers today.
Synonyms
Trench foot goes by many names: swamp foot, jungle rot, foxhole foot, paddy-field foot, peripheral vasoneuropathy, nonfreezing cold injury.
Pathophysiology
The core problem is overhydration of the stratum corneum (the outermost skin layer). The plantar (sole) skin is about 10x more permeable than dorsal foot skin, so it absorbs water rapidly - the plantar stratum corneum can absorb up to 200% of its dry weight in water.
In cold-water immersion (the classic form), cold-induced vasospasm is layered on top of this. Since water conducts heat 23 times faster than air, cooling is rapid. Prolonged cold causes:
- Peripheral vasoconstriction - reduced blood flow and tissue ischemia
- Direct nerve and soft tissue injury from sustained cooling
- Inflammatory changes - progressing to lymphocytic vasculitis with vascular compromise
- Secondary infection - macerated skin becomes a portal for pathogens, which can penetrate deep tissues within 3-4 days
Clinical Stages
| Stage | Features |
|---|---|
| Initial (cold phase) | Pale, mottled, numb foot; appears pulseless and immobile; tingling progressing to anesthesia |
| Hyperemic phase (hours after rewarming) | Severe burning pain, return of proximal sensation, intense redness |
| Post-rewarming (2-3 days) | Edema and blisters (bullae) form as circulation returns |
| Late complications | Anesthesia persisting weeks to months, hyperhidrosis (excess sweating), cold sensitivity, tissue sloughing, gangrene in severe cases |
Permanent peripheral neuropathy is possible, and feet that have suffered immersion injury are significantly more sensitive to re-injury.
Risk Factors
- Prolonged wet occupational/recreational exposure
- Constrictive footwear, immobility
- Dehydration and poor nutrition
- Smoking, peripheral vascular disease, diabetes
- Homelessness, altered mental status
- Prior frostbite or trench foot
Treatment
Treatment is primarily supportive:
- Gently rewarm the feet (do not rub or apply direct heat)
- Keep feet clean, dry, and elevated
- Dryly bandage and monitor closely for infection
- Vasodilators may help - oral prostaglandin E1 (limaprost 20 mcg three times daily) has been shown to increase skin temperature and improve circulation
- Treat infection aggressively if present; deep infections can spread to bone and bloodstream
Prevention
- Keep feet warm and dry; change wet socks multiple times daily
- Never sleep in wet socks or boots
- Ensure proper boot fit (avoid constrictive footwear)
- At first signs (tingling, numbness), immediately warm, dry, and elevate the feet
Sources: Tintinalli's Emergency Medicine, p. 1510-1512; Dermatology 2-Volume Set 5e (Immersion Foot section); Cleveland Clinic overview
What is paroxysmal nocturnal dysneoa
Finding Sources
Searching the Web
paroxysmal nocturnal dyspnea mechanism heart failure pathophysiology
Reading File
Reading File
Loading Image
Paroxysmal Nocturnal Dyspnea (PND)
Definition
PND is acute, severe shortness of breath that suddenly awakens a patient from sleep, typically occurring about 1 hour after lying down. It subsides within minutes of sitting upright or standing. It is a cardinal symptom of severe left-sided heart failure and is associated with increased mortality.
The name breaks down simply: paroxysmal = sudden/episodic, nocturnal = at night, dyspnea = breathlessness.
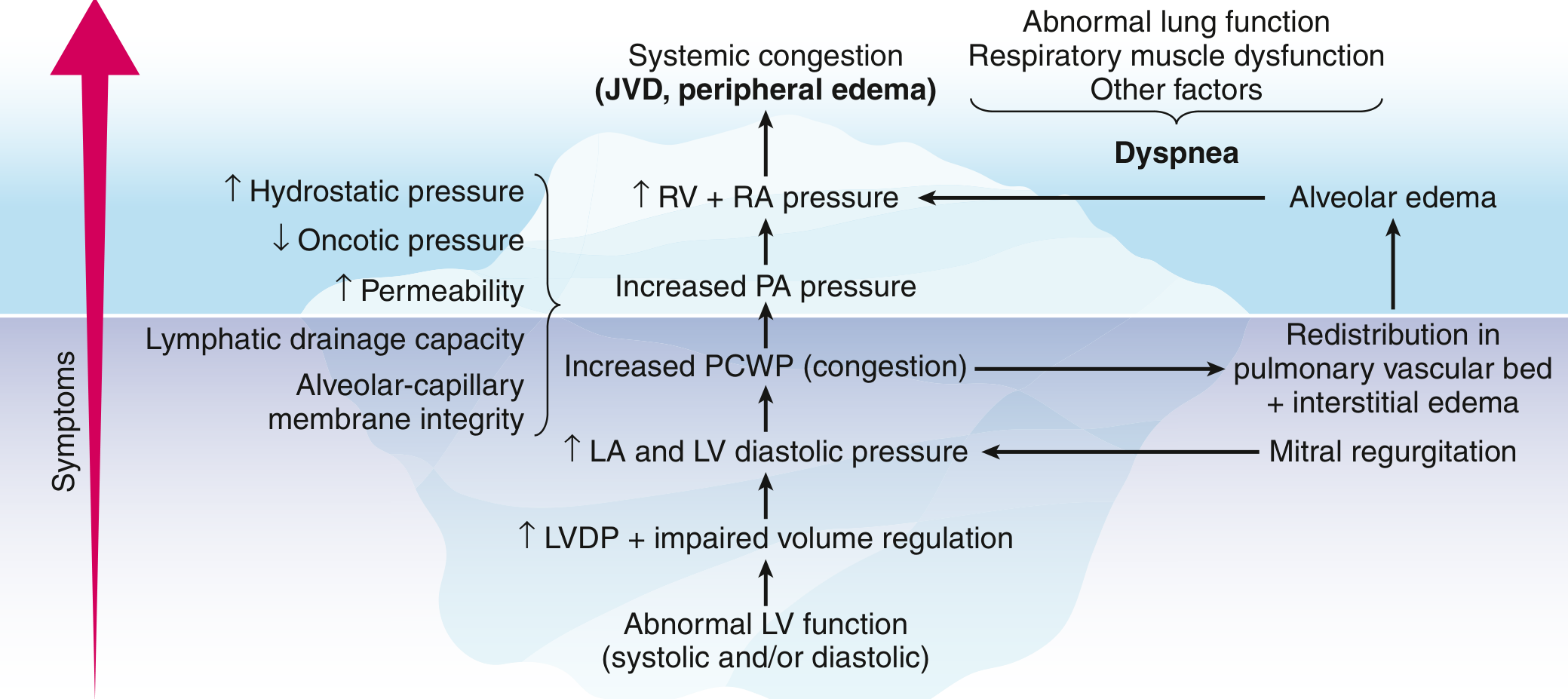
Mechanism - Why Does It Happen at Night?
When a person with heart failure lies flat (recumbent), several things happen:
- Fluid redistribution - Interstitial fluid that pooled in the legs and splanchnic (gut) circulation during the day is reabsorbed into the bloodstream and returned to the heart
- Increased venous return (preload) raises left ventricular diastolic pressure and pulmonary capillary wedge pressure (PCWP)
- This raises pressure in the pulmonary vasculature, driving fluid from capillaries into the alveoli - acute pulmonary edema
- The patient wakes up gasping, typically 1-2 hours after falling asleep (it takes this long for fluid to redistribute)
- Sitting or standing quickly relieves it by reversing venous return back to the legs
The diagram below from Goldman-Cecil Medicine illustrates this cascade:
PND vs. Related Symptoms
| Symptom | Trigger | Timing | Relief |
|---|---|---|---|
| PND | Lying flat + time for fluid to redistribute | Wakes patient 1-2 hrs after sleep onset | Sitting/standing within minutes |
| Orthopnea | Immediately on lying flat | Prevents sleep unless propped up on pillows | Elevating head of bed |
| Bendopnea | Bending forward | During the act of bending | Straightening up |
| Dyspnea on exertion | Physical activity | During exercise | Rest |
PND is considered more severe than orthopnea - it almost always represents advanced heart failure.
Causes
The most common underlying causes include:
- Left ventricular failure (systolic or diastolic) - the classic cause
- Ischemic heart disease / prior MI
- Poorly controlled hypertension
- Mitral regurgitation or stenosis
- Less commonly: COPD, sleep apnea (can mimic PND)
Clinical Significance
- PND is a specific marker of heart failure - when present in its classic form, it almost always indicates significant left ventricular dysfunction
- It correlates with elevated pulmonary capillary wedge pressure and pulmonary congestion
- Associated with increased mortality in heart failure patients
- Its presence alongside orthopnea, fatigue, and edema forms the classic symptom cluster of congestive heart failure
Management
PND is treated by treating the underlying heart failure:
- Diuretics (e.g. furosemide) - reduce fluid overload
- ACE inhibitors / ARBs / ARNIs - reduce preload and afterload
- Beta-blockers - improve LV function over time
- Sodium and fluid restriction
- Elevating the head of the bed provides symptomatic relief
Sources: Goldman-Cecil Medicine, p. 2323; Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.