Deviated nasal septum
Reading File
Finding Sources
Searching PubMed
"deviated nasal septum" AND septoplasty
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material for a thorough answer. Let me compile the full response.
Deviated Nasal Septum (DNS)
Definition and Anatomy
The nasal septum is the midline partition of the nose composed of the quadrangular (septal) cartilage anteriorly, the perpendicular plate of the ethmoid bone superoposteriorly, and the vomer inferoposteriorly, all covered by mucoperichondrium/mucoperiosteum. A deviated nasal septum (DNS) is a displacement of this partition from the midline, representing one of the most common causes of unilateral nasal airway obstruction.
- Cummings Otolaryngology Head and Neck Surgery, p. 567
Etiology and Pathogenesis
DNS arises from two broad mechanisms:
1. Developmental / Congenital
- Overgrowth of the quadrangular cartilage may cause bowing or spur formation at the junction with the vomer and maxillary crest.
- Birth trauma (forceps delivery, passage through a narrow pelvic canal) can cause injury leading to early septal deviation or deviation that manifests only during the growth spurt of puberty.
- Minor trauma sustained early in life often causes microfractures of the septal cartilage; as these heal, the cartilage bends away from the side of injury. When this occurs early, it may lead to asymmetric growth of the entire nasal structure due to chondrocyte growth interruption.
2. Acquired / Traumatic
-
Nasal and midfacial trauma at any age.
-
Previously overlooked minor injuries frequently leave behind healed microfractures.
-
Cummings Otolaryngology, p. 567; Murray & Nadel's Respiratory Medicine
Classification
Deviations are classified by location and severity (Cottle's areas):
Location (Cottle's 5 Areas)
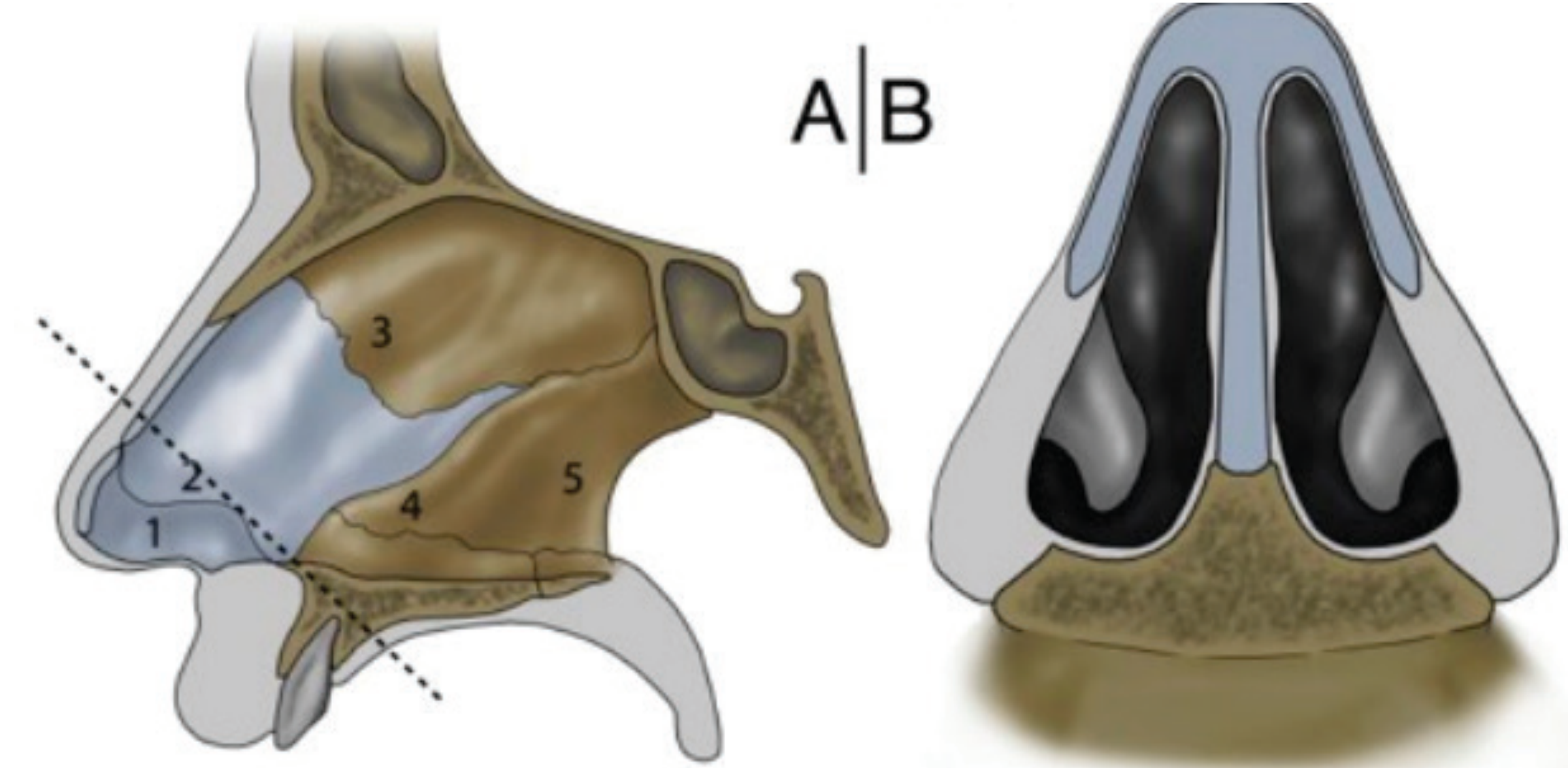
| Area | Location |
|---|---|
| 1 | Caudal septum (columellar/vestibular) |
| 2 | Internal nasal valve region |
| 3 | High mid septum |
| 4 | Low mid septum |
| 5 | Posterior septum |
Severity Grading
-
Grade 0 - No deviation
-
Grade 1 - Minimal
-
Grade 2 - Less than 50% lateralized
-
Grade 3 - More than 50% lateralized
-
Grade 4 - Fully lateralized (mucosal contact with lateral nasal wall)
-
Scott-Brown's Otorhinolaryngology, Vol. 1, Fig. 88.1
Morphological Types
- C-shaped (simple lateral deflection)
- S-shaped (sigmoid/double deflection - one side anteriorly, opposite side posteriorly)
- Septal spur - a sharp bony or cartilaginous projection, frequently at the bony-cartilaginous junction
- Caudal dislocation - displacement of the caudal septum off the maxillary crest
Symptoms
-
Unilateral nasal obstruction (most common) - typically on the concave side (side toward which septum is deviated)
-
Paradoxical nasal obstruction - the patient complains of obstruction on the contralateral (wider) side, possibly due to turbinate prominence in the wider passage; patients are often confused when told the side they feel airflow through is anatomically the more open side
-
Mouth breathing
-
Snoring and sleep-disordered breathing
-
Headaches and facial pain (from turbinate or sinus contact)
-
Epistaxis (bleeding is not unusual on either side of a deviated septum)
-
Recurrent sinusitis (due to impaired mucociliary drainage)
-
Hyposmia
-
Cummings Otolaryngology, p. 567-568
Compensatory Changes
A septal deviation on one side causes compensatory hypertrophy of the inferior turbinate on the contralateral side (the more open side). The turbinate bone and mucosa enlarge into the more open nasal passage in pursuit of normalizing overall nasal airway resistance. Histological studies confirm this enlargement involves both an increase in conchal bone size and mucosal thickness.
This is clinically important: straightening the septum without addressing the hypertrophied turbinate will leave the patient obstructed on the side where they did not perceive obstruction preoperatively.
- Cummings Otolaryngology, p. 571; Scott-Brown's, p. 1213
Diagnosis and Evaluation
History
- Duration of symptoms, side, severity
- History of nasal trauma
- Failure of medical therapy (nasal steroids, decongestants)
Physical Examination
- Anterior rhinoscopy - the deviation is often readily apparent; important to inspect for posterior nasal spurs (a hypertrophic turbinate can obscure a posterior spur)
- Nasal endoscopy - rigid endoscopy provides full evaluation of the nasal cavity including polyps, masses, adenoid, and high septal deviations that impinge on the internal nasal valve
- Cottle maneuver - lateral traction on the cheek; a positive test suggests nasal valve compromise, but has many false-positives due to the large mass movement
- Modified Cottle (more specific) - gentle lateralization of the upper lateral cartilage with a cotton-tipped applicator specifically increases the internal nasal valve angle; improvement confirms valve compromise and the likely benefit of spreader grafts
- Nasal valve angle - normally 10-15 degrees in Caucasian patients; wider in non-Caucasians
Objective Measurement
-
Acoustic rhinometry - delivers sound waves, measures their reflection to generate a rhinogram; identifies the minimum cross-sectional area; the first dip = nasal valve, second dip = anterior turbinate tips. Testing before and after topical decongestion differentiates anatomic from physiologic obstruction.
-
Rhinomanometry - measures nasal airway resistance
-
NOSE scale / SNOT-22 - validated patient-reported outcome tools
-
Cummings Otolaryngology, p. 570
Management
Non-surgical (Conservative)
- Topical intranasal corticosteroids (reduce mucosal component and turbinate congestion)
- Intranasal decongestants (short-term)
- Saline irrigation
- Management of underlying allergic rhinitis
- Many insurance plans require documented failure of 6 weeks of nasal steroid therapy before approving surgery, despite anatomic obstruction that will clearly not be resolved medically.
Surgical - Septoplasty
The definitive treatment for symptomatic DNS is septoplasty (from the Greek - "to reshape or mold the septum"). The primary goals are mucosal preservation and submucosal correction of cartilaginous/bony abnormalities.
Indications
- Nasal obstruction refractory to medical management
- Recurrent epistaxis related to septal spur/deviation
- As part of endoscopic sinus surgery (to gain surgical access)
- Combined with rhinoplasty (septorhinoplasty) when external nasal deformity coexists
- CPAP non-compliance due to nasal obstruction in sleep apnea patients
Standard Septoplasty Technique
- Incision - hemitransfixion incision (between columellar skin and mucosa) or Killian incision (within the vestibule, 1 cm posterior to the caudal margin)
- Mucoperichondrial flap elevation - bilateral subperichondrial tunnels, preserving mucosa
- Cartilage and bone correction - resection, scoring, or repositioning of deviated segments
- L-strut preservation - a minimum 1-cm caudal and dorsal strut must be preserved to maintain tip and dorsal support; surgeons should limit resection to only the portions necessary to straighten the septum
- Spur removal - Becker scissors make cuts above and below bony spurs; the superior bony septum is never manipulated without a superior incision first (to prevent cribriform plate injury)
- Closure - quilting sutures to reapproximate the mucoperichondrial flaps; the Wright suture technique stabilizes fractured segments
Endoscopic Septoplasty
- Introduced in 1994 (Giles et al.)
- Incision just caudal to the deviation; circumferential mucoperichondrial elevation around it
- Best for limited deviations and isolated septal spurs, especially concurrent with endoscopic sinus surgery
- Not suitable for caudal deflections, maxillary crest irregularities, high dorsal deflections, or complex deviations - these require conventional open access
- Outcomes comparable to conventional septoplasty for limited deviations (Bothra & Mathur, n=80 RCT)
Extracorporeal Septoplasty
- For markedly deviated septum
- The entire cartilaginous septum is removed, straightened ex vivo, fixated, replanted, and stabilized with spreader grafts
- Risk: dorsal irregularities, tip de-projection and rotation from disruption of tip support mechanisms
Submucous Resection (SMR)
- Older technique - excises deformed septal cartilage while preserving a caudal and dorsal strut
- Risk: if too much cartilage is removed, loss of dorsal support results in a supra-tip depression or drooping nasal tip
Turbinate Surgery as Adjunct
-
Formal studies show a positive effect from submucous unilateral inferior turbinate reduction (assessed by acoustic rhinometry and patient self-assessment at 6 months)
-
However, most septal corrective surgery is performed without turbinate reduction and patients generally have satisfactory outcomes
-
Risks of adding turbinate surgery: increased intraoperative bleeding and postoperative adhesion formation
-
In sleep-disordered breathing: a conservative approach with mucosal preservation turbinate reduction is recommended; most studies support it as an adjunct for snoring, but none show a significant decrease in the apnea-hypopnea index
-
Cummings Otolaryngology, pp. 571-577; Scott-Brown's Otorhinolaryngology, p. 1213; Bailey & Love's Surgery, p. relevant section
Complications of Septal Surgery
| Complication | Detail |
|---|---|
| Septal perforation | Bilateral mucosal tears at the same level; inadequate healing leads to a through-and-through hole causing turbulent airflow, crusting, bleeding, whistling |
| Supra-tip depression / saddle nose | Excessive cartilage removal removing dorsal support |
| Nasal tip ptosis | Overaggressive caudal septal trimming |
| Synechiae (adhesions) | Mucosal apposition between raw surfaces; narrows the nasal valve |
| Epistaxis | Early postoperative |
| Infection / septal abscess | Rare; can progress to cartilage necrosis |
| Cribriform plate injury | From aggressive posterior/superior bone manipulation |
| Persistent obstruction | Reported in 20-30% of patients at long-term follow-up in the literature |
Prognosis
Septoplasty provides significant improvement in nasal airflow and symptom burden in most patients. A 2025 systematic review and meta-analysis by Taha et al. (PMID 39230606) demonstrated septoplasty's superiority over non-surgical management based on pooled RCT data. A 2024 meta-analysis by Wu et al. (PMID 39572690) confirmed that septoplasty also benefits patients with coexisting allergic rhinitis. In the literature, approximately 20-30% of patients report inadequate symptom correction with long-term follow-up, though outcomes improve when associated deformities (turbinate hypertrophy, nasal valve compromise) are also addressed.
Key Points Summary
- DNS is a very common anatomical finding; not all deviations are symptomatic
- Paradoxical obstruction (symptomatic on the wider side) is a real phenomenon
- Compensatory inferior turbinate hypertrophy on the contralateral side must be recognized
- Objective measurement (acoustic rhinometry) supplements clinical examination
- Septoplasty is the definitive treatment; the L-strut (1 cm caudal + 1 cm dorsal margin) must always be preserved
- Endoscopic septoplasty works well for limited deviations; complex deviations require conventional access
- Always address the nasal valve - high septal deviations can impinge on the internal nasal valve and are easily missed
Sources: Cummings Otolaryngology Head and Neck Surgery, pp. 567-577; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1; Bailey & Love's Short Practice of Surgery 28th Ed.; Murray & Nadel's Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.