bronchiectasis management
Reading File
Finding Sources
Searching PubMed
"bronchiectasis"[MeSH Terms] AND management
Finding Sources
Searching PubMed
"bronchiectasis"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough response. Here is the comprehensive guide:
Bronchiectasis: Management
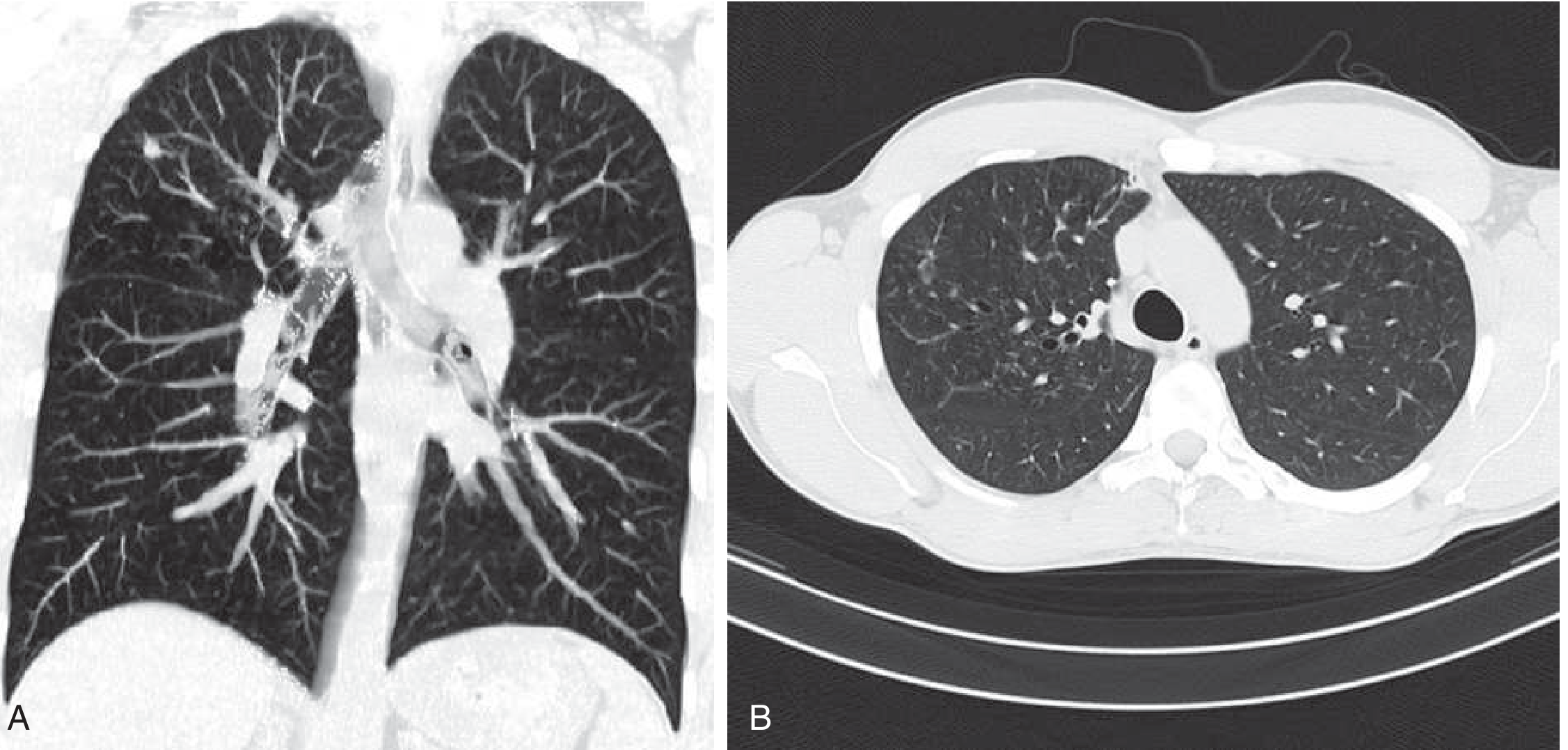
HRCT of bronchiectasis: (A) coronal view showing dilated, mucus-filled airways, (B) axial cross-section demonstrating the classic "signet ring" appearance of dilated bronchi alongside pulmonary vessels. - Goldman-Cecil Medicine
Overview
Bronchiectasis is abnormal, irreversible dilatation of the bronchi and bronchioles caused by a self-perpetuating cycle of infection and inflammation. There are no FDA-approved therapies specifically for non-cystic fibrosis (non-CF) bronchiectasis as of current guidelines, so management is multimodal and individualized. Treatment goals are to:
- Reduce exacerbation frequency
- Improve airway clearance and quality of life
- Slow lung function decline
- Treat the underlying cause when possible
1. Treat the Underlying Etiology
Identifying and treating the root cause is a first-line priority:
| Underlying Cause | Treatment |
|---|---|
| IgG/IgA/IgM deficiency | IV or subcutaneous immunoglobulin replacement |
| Alpha-1 antitrypsin deficiency | AAT replacement therapy |
| Allergic bronchopulmonary aspergillosis (ABPA) | Systemic corticosteroids + itraconazole |
| Autoimmune disease (RA, Sjogren's) | Disease-modifying therapy |
| NTM infection (MAC) | Macrolide + rifampin + ethambutol (see below) |
| Cystic fibrosis | CFTR modulators (e.g., elexacaftor/tezacaftor/ivacaftor) |
- Goldman-Cecil Medicine, p. 917; Harrison's Principles 22E, p. 2287
2. Airway Clearance (Cornerstone of Maintenance)
Airway clearance is the most important non-pharmacologic intervention. Cough is actually the most effective natural mechanism for clearing secretions in bronchiectasis.
Devices and techniques:
- Oscillatory positive expiratory pressure (OPEP) devices (e.g., Acapella, Flutter valve) - twice-daily use improves sputum volume and quality of life
- High-frequency chest wall oscillation (HFCWO) vests
- Postural drainage with percussion
- Active cycle of breathing technique and autogenic drainage
- Pulmonary rehabilitation and regular exercise - improves exercise capacity, secretion clearance, and quality of life
Pharmacologic airway clearance:
- Nebulized hypertonic saline (3-7%) - enhances mucociliary clearance, decreases exacerbations, and may improve lung function
- Bronchodilators (inhaled beta-2 agonists) - useful in patients with airway reactivity to improve mucociliary clearance and reverse bronchoconstriction; not routinely indicated for all patients without demonstrated reversibility
- DNase (dornase alfa) - effective in CF bronchiectasis but should NOT be used in non-CF bronchiectasis (large clinical trial showed deleterious effects)
- Goldman-Cecil Medicine, p. 917; Harrison's 22E, p. 2287; Fishman's Pulmonary Diseases, p. 897
3. Antibiotic Therapy
Acute Exacerbations
Exacerbations are recognized by worsening cough, increased sputum volume/purulence, dyspnea, hemoptysis, or systemic symptoms (fever, malaise).
Common pathogens:
- Haemophilus influenzae (most common)
- Pseudomonas aeruginosa (associated with worse outcomes, higher mortality)
- Staphylococcus aureus, Moraxella catarrhalis, Streptococcus pneumoniae
- NTM (especially MAC in postmenopausal women, right middle lobe / lingula)
Antibiotic approach:
- Obtain sputum culture before starting antibiotics, ideally
- Empiric oral antibiotics for mild-moderate exacerbations: amoxicillin (without GNR), oral levofloxacin (comparable to IV ceftazidime in one trial)
- For Pseudomonas: anti-pseudomonal agents (e.g., ciprofloxacin, piperacillin-tazobactam, ceftazidime)
- IV antibiotics for: severe exacerbations, resistant organisms, poor response to oral therapy
- Duration: 10-14 days minimum (some guidelines say 7-10 days)
- Combination antibiotics are not recommended for oral treatment of acute exacerbations, even with Pseudomonas colonization; they are used for severe exacerbations with Pseudomonas or MRSA
- Fishman's Pulmonary Diseases, p. 896-897; Harrison's 22E, p. 2287
Long-Term / Suppressive Antibiotic Therapy
Indicated in patients with 2-3 or more exacerbations per year ("frequent exacerbator phenotype"). Options:
-
Oral macrolides (most evidence):
- Azithromycin 500 mg three times per week, or 250 mg daily
- Erythromycin ethylsuccinate 400 mg twice daily
- Reduces exacerbation frequency, mucus production, and lung function decline
- Caution: Screen for NTM infection first (macrolide monotherapy in NTM co-infection promotes resistance, making treatment far more difficult); check ECG for QTc prolongation risk
- Check for macrolide resistance in commensal flora - resistance does emerge with chronic use
-
Cyclic oral antibiotics: e.g., ciprofloxacin for 1-2 weeks per month; rotating schedules to minimize resistance
-
Inhaled antibiotics (for Pseudomonas-colonized patients):
- Nebulized gentamicin (80 mg twice daily) - 12-month trial showed 31% Pseudomonas eradication, more pathogens cleared, longer time to exacerbation, improved quality of life
- Inhaled tobramycin - significant microbiologic impact on Pseudomonas, but adverse airway effects (cough, dyspnea, chest tightness) limit use
- Inhaled colistin (1 million IU twice daily) - possibly effective in adherent patients with Pseudomonas (median time to exacerbation 168 vs. 103 days in adherent patients)
- Inhaled aztreonam - two large phase 3 trials did NOT show clinical benefit
- Inhaled/dry powder ciprofloxacin - mixed trial results
-
Intermittent IV antibiotics - for severe bronchiectasis with resistant organisms
- Goldman-Cecil Medicine, p. 917; Harrison's 22E, p. 2287-2288; Murray & Nadel, p. 875
4. Anti-Inflammatory Therapy
- Inhaled corticosteroids (ICS): Inhaled medium-dose budesonide combined with formoterol is safer and more effective than high-dose budesonide alone. ICS may reduce dyspnea and sputum production but have not shown significant benefit on lung function or exacerbation rates in most trials. Risks of immunosuppression must be weighed. Systemic glucocorticoids are NOT routinely used but may be needed for ABPA or active autoimmune disease.
- Macrolides have anti-inflammatory as well as antimicrobial properties - they reduce gram-negative bacillary biofilms and modulate neutrophilic inflammation independent of their antibiotic effect.
- Novel agents:
- Brensocatib (DPP-1 inhibitor, 10-25 mg orally daily) - prolongs time to first exacerbation in non-CF bronchiectasis patients with ≥2 prior exacerbations/year. A Phase 2 trial showed positive results; meta-analysis of RCTs in 2025 confirmed efficacy and safety. [PMID 41299471]
- NSAIDs have been studied but definitive recommendations are not established.
- Goldman-Cecil Medicine, p. 917; Harrison's 22E; Murray & Nadel
5. Vaccination
Standard of care in all bronchiectasis patients:
- 23-valent pneumococcal vaccine (PPSV23)
- Annual influenza vaccine
- COVID-19 vaccine
- RSV vaccine (for eligible patients)
- Goldman-Cecil Medicine, p. 917; Harrison's 22E, p. 2288
6. Surgery and Transplantation
- Resectional surgery: Considered for focal, localized disease refractory to medical therapy; also for hemoptysis uncontrolled by bronchial artery embolization (BAE). May benefit some patients with NTM infection in localized disease.
- Bilateral lung transplantation: For diffuse, end-stage disease; outcomes parallel transplantation for other end-stage lung diseases.
- Goldman-Cecil Medicine, p. 917
7. Management of Massive Hemoptysis
A potentially life-threatening complication of severe bronchiectasis:
- Intubation to stabilize and protect the non-bleeding lung
- Identify the bleeding source (bronchoscopy)
- Bronchial artery embolization (BAE) - first-line intervention
- Surgery if embolization fails or is not feasible
8. NTM (Non-Tuberculous Mycobacteria) Co-Infection
NTM (especially MAC) is increasingly prevalent in bronchiectasis. Diagnostic criteria for true NTM infection (not just colonization):
- Two positive sputum cultures, OR
- One positive BAL culture, OR
- Biopsy with histopathologic evidence + one positive sputum culture
Treatment for macrolide-sensitive MAC (HIV-negative):
- Macrolide (azithromycin or clarithromycin) + rifampin + ethambutol
- Harrison's 22E, p. 2287
Severity and Phenotyping
The Bronchiectasis Severity Index (BSI) stratifies risk and guides therapeutic decisions. The "frequent exacerbator" phenotype (≥3 exacerbations/year) identifies patients at highest risk for hospitalization, worse quality of life, and increased mortality - this group derives the most benefit from long-term antibiotic therapy. Independent predictors of frequent exacerbations include P. aeruginosa or H. influenzae colonization, FEV1 <50% predicted, and coexisting COPD.
Summary Framework
BRONCHIECTASIS MANAGEMENT
Identify & treat underlying cause
↓
All patients:
- Airway clearance (OPEP device, postural drainage, exercise)
- Nebulized hypertonic saline
- Vaccinations (pneumococcal, influenza, COVID, RSV)
↓
Acute exacerbation:
- Sputum culture → empiric antibiotics (14 days)
- Oral (mild-moderate) or IV (severe/resistant)
↓
Frequent exacerbators (≥2-3/year):
- Long-term macrolide (rule out NTM/QTc first)
- Consider inhaled antibiotics if Pseudomonas-colonized
- Brensocatib (emerging option)
↓
Refractory / focal disease:
- Surgery (resection)
↓
End-stage diffuse disease:
- Bilateral lung transplantation
Recent evidence to note:
- A 2025 meta-analysis (PMID 41299471) confirmed DPP-1 inhibitor brensocatib reduces exacerbations in non-CF bronchiectasis - this represents the most promising new drug class for this condition.
- A 2025 meta-analysis (PMID 40339664) of inhaled tobramycin in non-CF bronchiectasis provides updated safety/efficacy data.
- A 2024 Lancet Respiratory Medicine review (PMID 38971168) proposes reframing bronchiectasis as a primarily inflammatory (not just infectious) disease, which may reshape how anti-inflammatory therapies are prioritized going forward.
Sources: Goldman-Cecil Medicine (26e), Harrison's Principles (22e), Fishman's Pulmonary Diseases (5e), Murray & Nadel's Textbook of Respiratory Medicine (7e)
This is a shared conversation. Sign in to Orris to start your own chat.