Colitis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
"ulcerative colitis" AND "management"
I now have comprehensive, authoritative content from multiple major textbooks plus the latest evidence. Here is the full, detailed response:
Colitis
Colitis refers to inflammation of the colon. It is not a single disease but an umbrella term encompassing multiple distinct conditions with different causes, pathology, and management.
Classification: Types of Colitis
The major types, per Sleisenger & Fordtran's:
| Category | Examples |
|---|---|
| Inflammatory Bowel Disease (IBD) | Ulcerative colitis, Crohn's colitis, IBD-unclassified |
| Infectious | Clostridioides difficile, Campylobacter, Salmonella, Shigella, E. coli O157, CMV, Entamoeba histolytica, TB |
| Ischemic | Reversible, non-gangrenous, ischemic stricture, toxic megacolon |
| Microscopic | Collagenous colitis, lymphocytic colitis |
| Drug-induced | NSAIDs, gold, checkpoint inhibitors (anti-CTLA4, anti-PD1) |
| Radiation | Post-pelvic radiotherapy |
| Diversion | Following bowel diversion surgery |
| Other | Eosinophilic colitis, Behcet disease, GVHD, sarcoidosis, SCAD |
1. Ulcerative Colitis (UC)
Definition and Epidemiology
UC is a chronic idiopathic inflammatory disease of the colon, most commonly affecting adults in their 3rd to 4th decades of life. It is characterized by a lifelong relapsing-remitting course. Incidence has stabilized in Western Europe/North America but continues to rise in Eastern Europe, Asia, and the developing world.
- Yamada's Textbook of Gastroenterology, 7th ed.
Pathogenesis
Multifactorial - involving genetic predisposition, environmental factors, epithelial barrier defects, dysregulated immune responses, and microbiological factors. Infectious enteritis may trigger mucosal immune activation in susceptible individuals. Unlike Crohn's disease, UC onset can be associated with smoking cessation (smoking provides partial symptomatic relief).
Distribution (Montreal Classification)
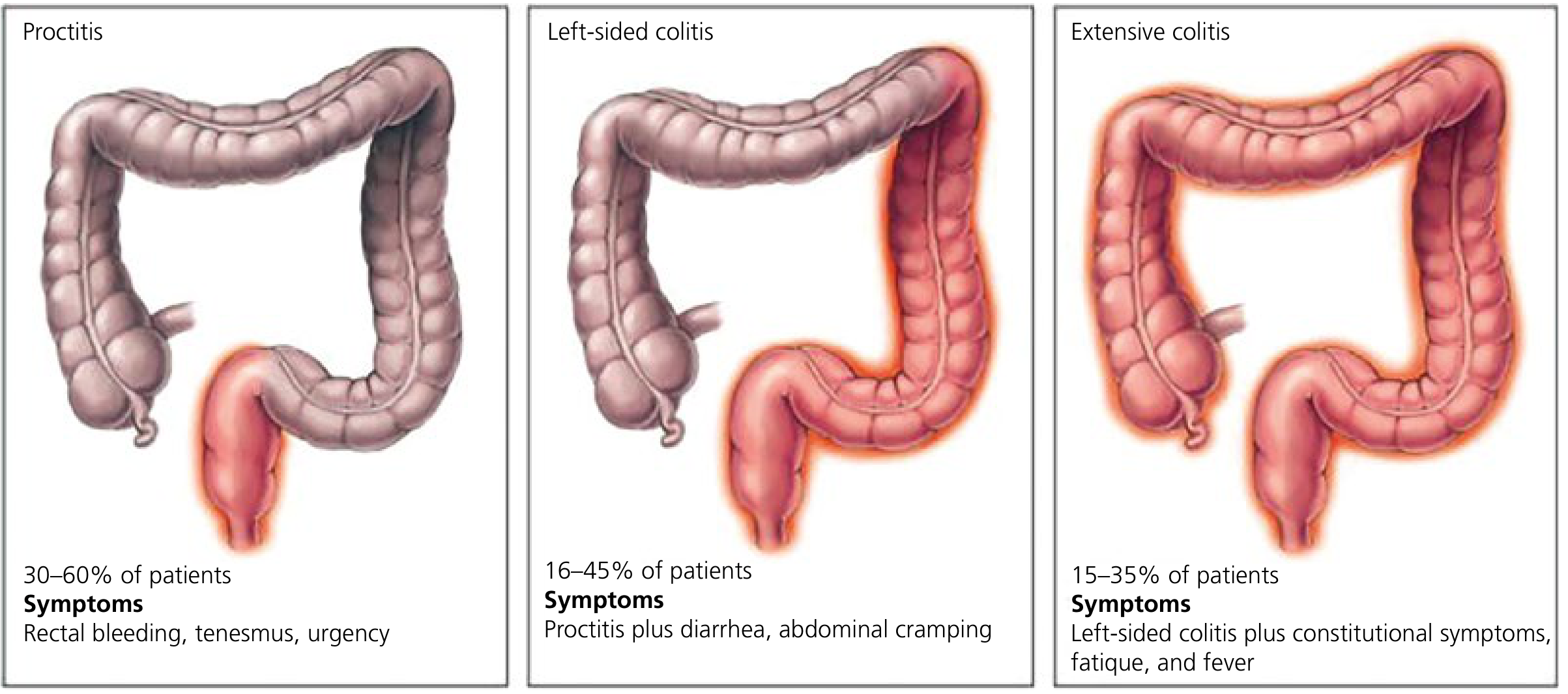
Inflammation begins in the rectum and extends proximally in a continuous, circumferential fashion:
- Proctitis (30-60% of patients): rectal bleeding, tenesmus, urgency
- Left-sided colitis (16-45%): above plus diarrhea, abdominal cramping
- Extensive/pancolitis (15-35%): all of the above plus constitutional symptoms, fatigue, fever
At diagnosis: left-sided colitis ~40%, extensive colitis ~30%, proctitis ~30%.
Symptoms
- Bloody diarrhea with mucopurulent discharge (most consistent feature)
- Rectal urgency, tenesmus, sensation of incomplete evacuation
- Colicky abdominal pain preceding bowel movements
- Up to 10% have paradoxical constipation (especially proctitis/left-sided)
- Severe/fulminant: fever, night sweats, weight loss
Extraintestinal Manifestations (7-17% of patients)
- Arthritis (most common): peripheral pauciarticular (follows bowel activity) or axial spondyloarthropathy (independent of bowel activity; can be progressive)
- Dermatological: pyoderma gangrenosum (1-5%), erythema nodosum
- Ocular: uveitis, episcleritis
- Hepatobiliary: primary sclerosing cholangitis
Gross and Microscopic Pathology
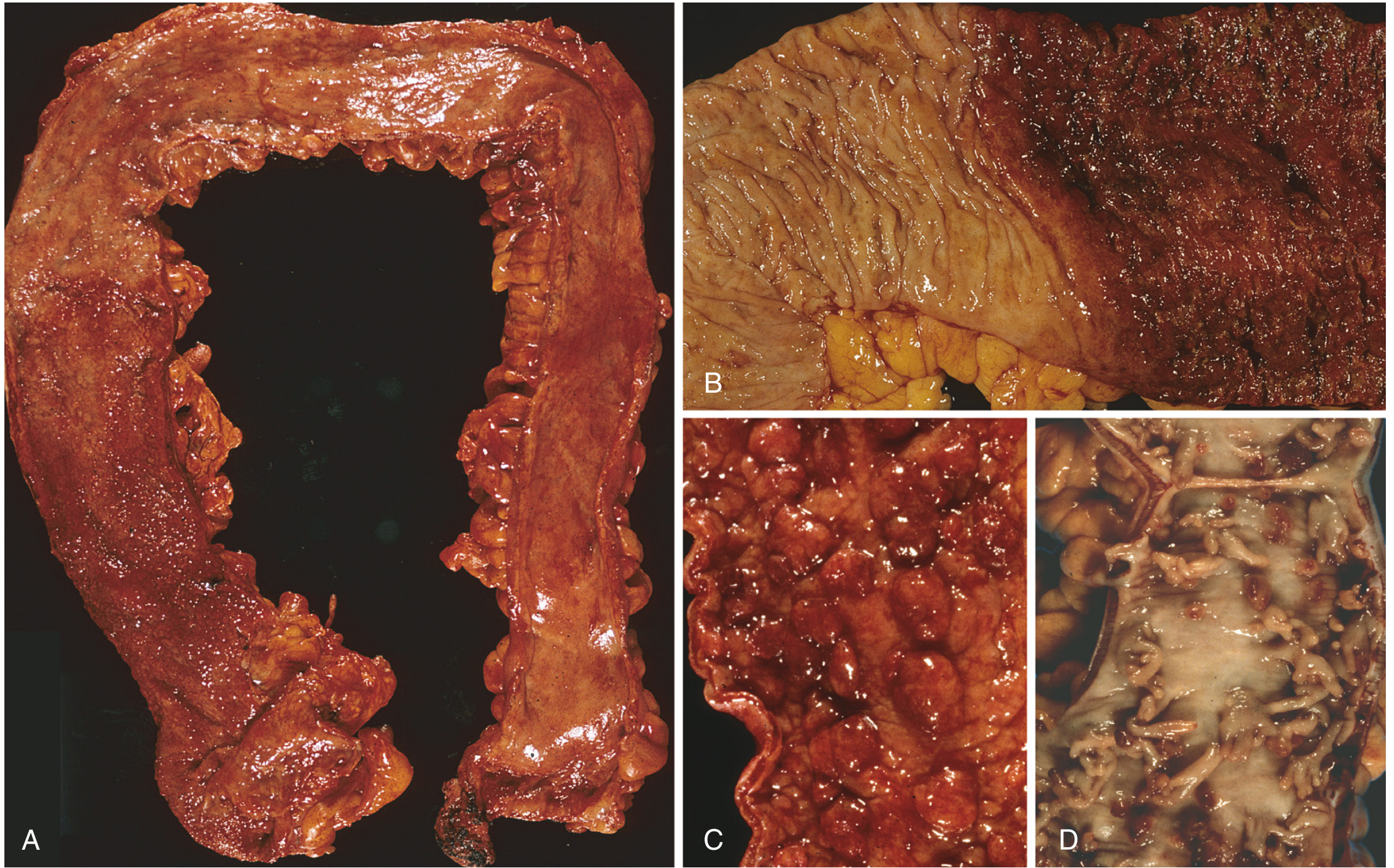
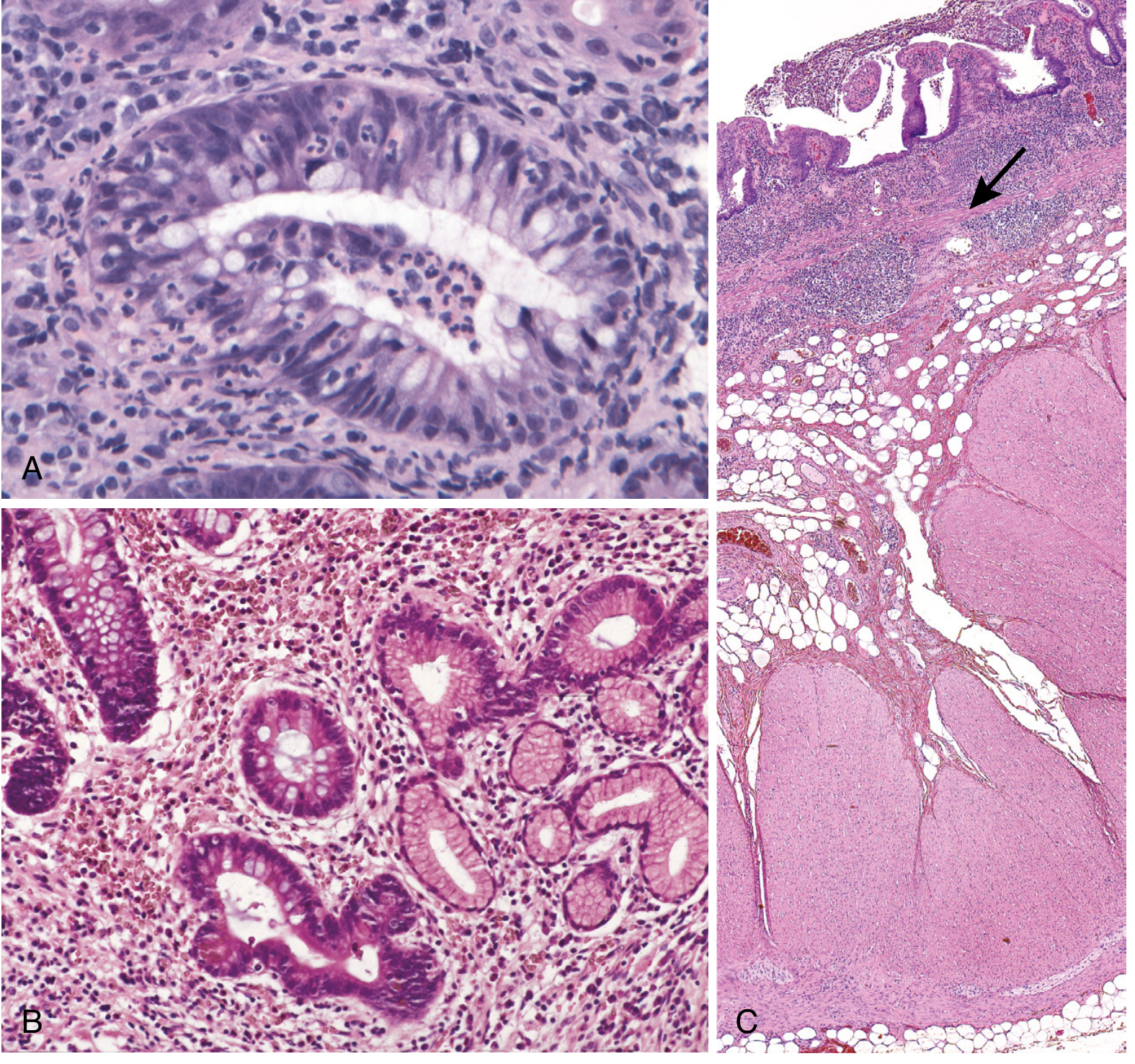
Key features:
- Diffuse, superficial (mucosal only) inflammation - does not extend beyond mucosa (key distinction from Crohn's)
- Red, granular mucosa; crypt abscesses; loss of goblet cells
- Crypt architectural distortion in chronic disease
- Inflammatory polyps (pseudopolyps); mucosal bridges
- Backwash ileitis in extensive colitis (distal ileum involved superficially)
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Diagnosis
- Colonoscopy with biopsy - contiguous inflammation from rectum; granularity, friability, pseudopolyps
- Histology confirms mucosal-limited disease
- Stool cultures to exclude infection
- Calprotectin (raised), CRP, ESR, CBC
Endoscopic distinction from Crohn's (Yamada's):
| Feature | UC | Crohn's |
|---|---|---|
| Distribution | Contiguous (+++), circumferential | Patchy (+) |
| Rectal involvement | +++ | + |
| Cobblestoning | + | +++ |
| Ileal involvement | - (backwash only) | ++++ |
| Deep/linear ulcers | + | +++ |
Disease Activity (Truelove-Witts / Mayo Score)
| Mild | Moderate-severe | Fulminant | |
|---|---|---|---|
| Stools/day | <4 | >6 | >10 |
| Blood in stools | Small | Obvious | Continuous |
| Systemic signs | None | Present | Severe |
Management
Step-up approach (conventional) or risk-stratified (modern):
Mild-moderate:
- 5-ASA (mesalamine/sulfasalazine) - first-line for mild-moderate UC and maintenance. Rectal formulations (suppositories, enemas) for proctitis/left-sided; oral for extensive. Sulfasalazine is linked by azo-bond to sulfapyridine; the 5-ASA component acts locally in the colon.
- Combined oral + topical 5-ASA is superior to either alone
Moderate-severe:
- Corticosteroids (prednisolone, budesonide MMX) for induction - not for maintenance
- Biologics:
- Anti-TNF: infliximab, adalimumab, golimumab
- Anti-integrin: vedolizumab (gut-selective)
- Anti-IL-12/23: ustekinumab
- JAK inhibitors: tofacitinib, upadacitinib, filgotinib (oral; small molecule)
- Thiopurines (azathioprine, 6-MP): maintenance; often combined with biologics
Acute severe UC:
- IV hydrocortisone; if refractory: rescue therapy with infliximab or ciclosporin
- Colectomy if no response within 3-5 days ("rescue" threshold)
Surgery (~15% of patients): Proctocolectomy with ileal pouch-anal anastomosis (IPAA) - curative for intestinal disease; extraintestinal manifestations may persist. Historically up to 30% needed colectomy within 3 years, but this has fallen sharply with biologics.
A 2024 AGA network meta-analysis (PMID 39425738) compared advanced therapies for moderate-to-severe UC, providing updated evidence on relative efficacy ranking for biologic and small molecule agents.
Colorectal Cancer Risk
Risk begins after 8-10 years of extensive colitis. Surveillance colonoscopy is recommended. Colitis-associated dysplasia is flat and may be invisible, requiring systematic biopsies. Risk scales with extent and duration of disease.
2. Crohn's Colitis
Crohn's disease can affect any part of the GI tract from mouth to anus. When it involves the colon, it differs from UC in:
- Skip lesions (patchy, discontinuous)
- Transmural inflammation (vs. mucosal only in UC)
- Cobblestone mucosa from linear ulcers + submucosal edema
- Fistulae and abscesses (transmural fissures)
- Non-caseating granulomas (~35% of cases) - hallmark
- Creeping fat on serosa
- Rectal sparing possible; ileal involvement frequent
- Aphthous ulcers are the earliest lesion
- Submucosal fibrosis and muscular hypertrophy cause strictures
- Robbins, Cotran & Kumar Pathologic Basis of Disease
3. Microscopic Colitis
Encompasses collagenous colitis and lymphocytic colitis - considered variants of the same condition.
Key features:
- Chronic, watery, non-bloody diarrhea
- Normal colonoscopy (diagnosis requires biopsy)
- Primarily affects middle-aged and older women
- Associated with NSAIDs, PPIs, SSRIs, ranitidine
Histology:
- Collagenous colitis: thickened subepithelial collagen band (>10 µm) + surface epithelial damage + lamina propria lymphocytosis
- Lymphocytic colitis: increased intraepithelial lymphocytes (>20 per 100 epithelial cells) + lamina propria lymphocytosis; crypt architecture preserved
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Treatment: Stop offending drugs; budesonide (most effective); bismuth subsalicylate; cholestyramine
4. Ischemic Colitis
- Results from reduced blood flow to the colon (usually the splenic flexure or rectosigmoid - "watershed zones")
- Most common in the elderly with atherosclerosis; also post-aortic surgery, vasopressors, cocaine
- Presents with sudden-onset left-sided abdominal pain, bloody diarrhea
- Most cases are non-gangrenous and self-limiting
- CT shows thumbprinting (submucosal edema); colonoscopy shows segmental, non-specific inflammation
- Management: supportive (bowel rest, fluids); surgery for gangrene or stricture
5. Infectious Colitis
Major pathogens:
- C. difficile: post-antibiotic, pseudomembranous colitis; toxin-mediated; treat with fidaxomicin/vancomycin
- Campylobacter, Salmonella, Shigella: acute dysentery
- E. coli O157:H7: hemolytic uremic syndrome risk; do NOT use antibiotics
- Entamoeba histolytica: flask-shaped ulcers; treat with metronidazole + luminal agent
- CMV colitis: in immunocompromised; linear punched-out ulcers; treat with ganciclovir
6. Indeterminate Colitis
About 10% of IBD cases cannot be clearly classified as UC or Crohn's. No small bowel involvement; continuous colonic pattern like UC but with some Crohn's features (patchy histology, perianal lesions, family history). Medical management overlaps sufficiently with both conditions to allow effective treatment.
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Summary Comparison: UC vs. Crohn's Colitis
| Feature | Ulcerative Colitis | Crohn's Colitis |
|---|---|---|
| Location | Colon only (rectum always) | Any GI segment; may spare rectum |
| Pattern | Continuous, circumferential | Skip lesions, segmental |
| Depth | Mucosal only | Transmural |
| Granulomas | No | Yes (35%) |
| Fistulae/abscesses | Rare | Common |
| Strictures | Rare | Common |
| Smoking | Protective | Risk factor |
| Surgery | Colectomy = cure | Recurrence post-surgery |
| CRC risk | Yes (long-standing) | Yes (lower than UC) |
Sources: Yamada's Textbook of Gastroenterology, 7th ed. | Sleisenger & Fordtran's Gastrointestinal and Liver Disease | Robbins, Cotran & Kumar Pathologic Basis of Disease | Fischer's Mastery of Surgery, 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.