Write answer on steps in randomised controlled trial for psm exam university proff
Steps in a Randomised Controlled Trial (RCT)
Definition
Steps in Conducting an RCT
Step 1: Formulation of the Research Question (Hypothesis)
- Define a clear, specific, testable hypothesis.
- State the PICO framework: Population, Intervention, Comparison, Outcome.
- Example: "Does Drug X reduce blood pressure more than placebo in hypertensive adults?"
Step 2: Study Protocol and Ethical Approval
- Write a detailed study protocol specifying design, sample size, eligibility criteria, duration, endpoints, and statistical plan.
- Submit to an Institutional Ethics Committee (IEC) or Institutional Review Board (IRB) for approval.
- Register the trial in a public trial registry (e.g., CTRI in India, ClinicalTrials.gov).
- Obtain informed written consent from all participants.
Step 3: Selection of Study Population
- Define strict inclusion criteria (who qualifies).
- Define strict exclusion criteria (who is left out - e.g., pregnant women, severe comorbidities, children if not applicable).
- Participants must be eligible, willing, and able to comply with the protocol.
Step 4: Sample Size Calculation
- Calculate the minimum number of participants required to detect a clinically meaningful difference (effect size) with adequate:
- Power (usually 80% or 90%) - probability of detecting a true effect.
- Significance level (alpha = 0.05) - acceptable probability of false positive.
- Inadequate sample size leads to underpowered trials (false negatives).
Step 5: Randomisation (Allocation)
| Method | Description |
|---|---|
| Simple randomisation | Coin toss, random number table, computer-generated sequence |
| Block randomisation | Ensures equal group sizes at intervals; groups divided into blocks of fixed size (e.g., 4 or 6) |
| Stratified randomisation | Randomise separately within strata (e.g., age, sex, severity) to ensure balance on key variables |
| Cluster randomisation | Entire groups (e.g., villages, schools) are randomised rather than individuals |
Step 6: Allocation Concealment
- The randomisation sequence must be concealed from the person recruiting/enrolling participants until the moment of allocation.
- Prevents selection bias even when randomisation has occurred.
- Methods: Sequentially Numbered Opaque Sealed Envelopes (SNOSE), central telephone randomisation, web-based systems.
- Allocation concealment ≠ blinding; it occurs before allocation, blinding occurs after.
Step 7: Blinding (Masking)
| Level | Who is blinded |
|---|---|
| Single blind | Participant only |
| Double blind | Both participant and investigator/assessor |
| Triple blind | Participant, investigator, and data analyst/statistician |
| Open label | No blinding (used when blinding is impossible, e.g., surgical vs. medical) |
- Use of identical placebo (same appearance, taste, smell) is required for drug trials.
Step 8: Implementation of Intervention
- Administer the intervention (drug, vaccine, procedure) to the experimental group.
- Administer a placebo or standard treatment to the control group.
- Ensure protocol adherence and monitor for protocol deviations.
- Maintain a run-in period if needed (to exclude non-compliant participants before randomisation).
Step 9: Follow-up and Data Collection
- Follow all participants for a pre-specified duration.
- Collect outcome data at defined time points.
- Monitor for:
- Adverse events and side effects
- Drop-outs and withdrawals (document reasons)
- Cross-overs (control participants receiving intervention)
- Minimise loss to follow-up (should ideally be <20%).
Step 10: Outcome Assessment
- Measure primary outcomes (the main endpoint, e.g., mortality, cure rate).
- Measure secondary outcomes (additional endpoints, e.g., hospitalisations, quality of life).
- Use pre-defined, objective, validated outcome measures.
- Outcome assessors should be blinded to group assignment.
Step 11: Statistical Analysis
- Intention-to-treat (ITT) analysis - analyse all participants in the group they were originally randomised to, regardless of compliance. This preserves the benefit of randomisation and reflects real-world effectiveness.
- Per-protocol (PP) analysis - analyse only those who completed the trial per protocol. Gives a measure of efficacy under ideal conditions.
- Compare outcomes between groups using appropriate statistical tests (t-test, chi-square, log-rank, etc.).
- Calculate Relative Risk (RR), Relative Risk Reduction (RRR), Absolute Risk Reduction (ARR), and Number Needed to Treat (NNT).
Step 12: Reporting of Results
- Report results following the CONSORT (Consolidated Standards of Reporting Trials) checklist and flow diagram.
- The CONSORT flow diagram shows: enrolled -> randomised -> allocated -> followed-up -> analysed in each group, with reasons for exclusion at every step.
- Publish in a peer-reviewed journal with full disclosure of conflicts of interest and funding.
Summary Flowchart
Hypothesis → Protocol & Ethics Approval → Eligibility Criteria
→ Sample Size Calculation → Enrolment of Participants
→ RANDOMISATION
↙ ↘
Experimental Group Control Group
(Intervention) (Placebo/Standard Rx)
↓ ↓
Follow-up & Outcome Assessment (Blinded)
↓
Statistical Analysis (ITT)
↓
Reporting (CONSORT)
Common Biases in RCTs and How Steps Address Them
| Bias | Step that prevents it |
|---|---|
| Selection bias | Randomisation |
| Allocation bias | Allocation concealment |
| Performance bias | Blinding of participants |
| Detection/observer bias | Blinding of outcome assessors |
| Attrition bias | Intention-to-treat analysis |
| Reporting bias | Trial registration, CONSORT reporting |
Important Terminologies
- Phase I trial: Safety and dosage - small group of healthy volunteers.
- Phase II trial: Efficacy and side effects - small group of patients.
- Phase III trial: Definitive efficacy vs. control in large population - this is the classic RCT.
- Phase IV trial: Post-marketing surveillance after drug approval.
- Run-in period: Pre-randomisation period to check compliance and exclude non-responders.
- Wash-out period: Period between arms in crossover trials to eliminate carry-over effects.
- Cross-over RCT: Same participant receives both intervention and control in sequence (with wash-out in between); each participant is their own control.
Key Points for Exam
- Randomisation is the defining feature of an RCT - it eliminates confounding.
- Allocation concealment prevents selection bias at enrolment.
- Blinding prevents bias after allocation.
- Intention-to-treat analysis is the standard; it preserves the benefits of randomisation.
- CONSORT checklist is the reporting standard for RCTs.
- Phase III trials are the classic RCT used for drug/vaccine approval.
- RCT has highest internal validity among analytical study designs but may have limited external validity due to strict eligibility criteria.
Flow chart s
A clean professional medical flowchart showing Steps in a Randomised Controlled Trial (RCT) for PSM exam. The flowchart flows top to bottom with labeled boxes and arrows. Steps in order: 1. Formulate Research Question (PICO) → 2. Study Protocol and Ethics Approval (IEC/IRB, Trial Registration, Informed Consent) → 3. Define Eligibility Criteria (Inclusion and Exclusion) → 4. Sample Size Calculation (Power 80-90%, Alpha 0.05) → 5. Enrolment of Study Participants → 6. RANDOMISATION (central large highlighted box, with sub-note: Simple / Block / Stratified / Cluster) → then splits into two parallel boxes: LEFT: Experimental Group - Intervention (Drug/Vaccine/Procedure) and RIGHT: Control Group - Placebo or Standard Treatment → both arrows point down to: 7. Allocation Concealment (SNOSE / Central Randomisation) → 8. Blinding / Masking (Single / Double / Triple Blind) → 9. Implementation of Intervention → 10. Follow-up and Data Collection (Monitor AEs, Drop-outs, Compliance) → 11. Outcome Assessment (Primary and Secondary outcomes, Blinded assessors) → 12. Statistical Analysis - Intention-to-Treat (ITT) Analysis (Calculate RR, ARR, NNT) → 13. Reporting of Results - CONSORT Checklist and Flow Diagram. Use a white background, blue header boxes, green for the randomisation step, light yellow for the two parallel group boxes, and clean sans-serif fonts. Add small icons where appropriate. Professional medical textbook style.
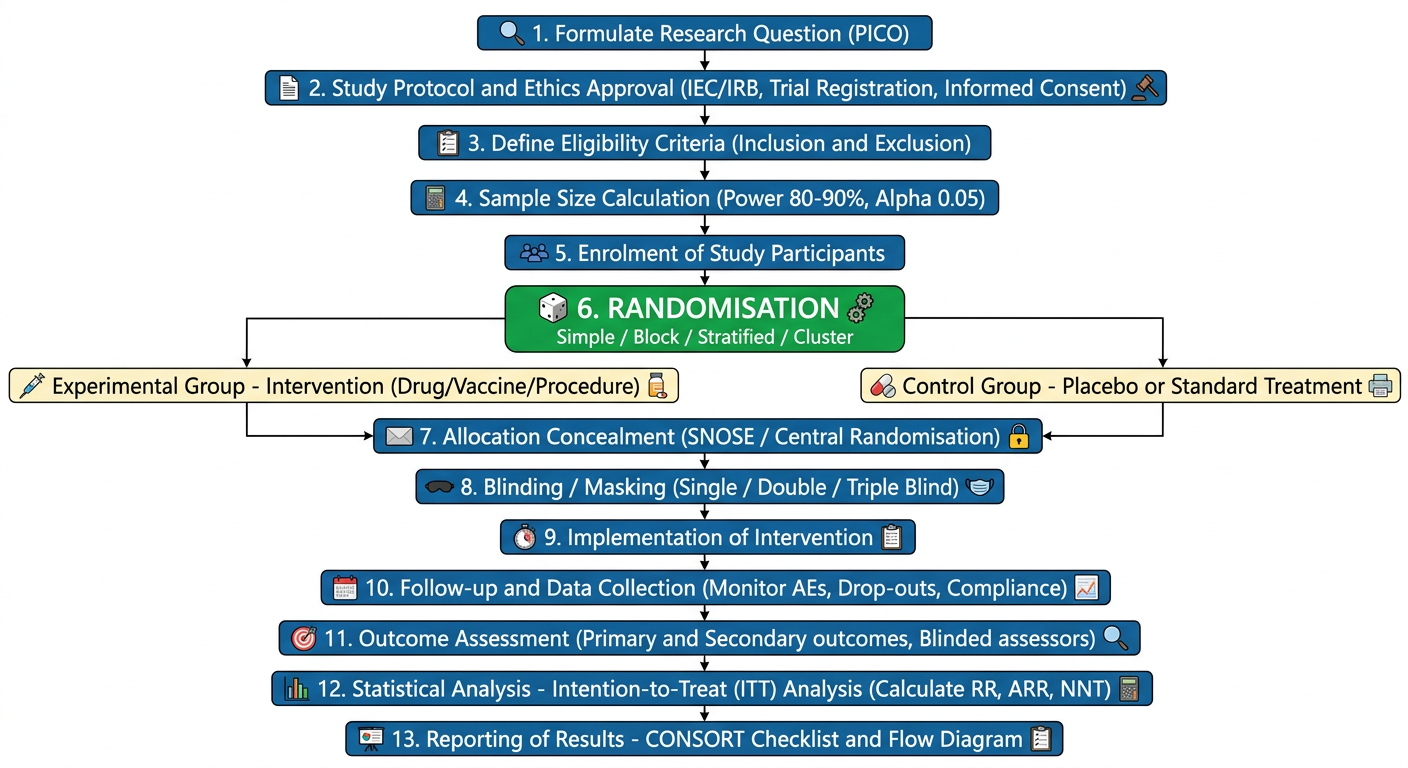
- The RANDOMISATION box is the central/highlighted step - examiners always look for this
- Show the split into two parallel arms (Experimental vs Control) clearly with branching arrows
- Write Intention-to-Treat (ITT) Analysis specifically in the analysis step - it's a common viva point
- End with CONSORT - shows awareness of reporting standards
- You can add a side note: "Allocation concealment prevents selection bias; Blinding prevents performance and detection bias"
Find recent RCT examples on vaccination or drug trials from PubMed
vaccine efficacy randomized controlled trial
drug trial randomized controlled placebo
Recent RCT Examples from PubMed
VACCINE TRIALS
- Reference: Wilson E et al., N Engl J Med, Dec 2023 - PMID: 38091530
- Design: Double-blind, placebo-controlled Phase II/III RCT
- Intervention: mRNA-based RSV PreF vaccine vs placebo in adults aged 60+
- Key finding: Significant reduction in RSV-associated lower respiratory tract disease
- PSM relevance: Classic example of vaccine RCT with blinding, Phase III design, and elderly population
- Reference: Tricou V et al., Lancet Global Health, Feb 2024 - PMID: 38245116
- Design: Phase III, randomised, double-blind, placebo-controlled, long-term follow-up
- Intervention: Tetravalent dengue vaccine TAK-003 vs placebo
- Key finding: Sustained efficacy over 4.5 years, good safety profile
- PSM relevance: Excellent example of long-term follow-up in an RCT; dengue is a major PSM topic in India
- Reference: Kallás EG et al., N Engl J Med, Feb 2024 - PMID: 38294972
- Design: Phase III RCT, live attenuated tetravalent vaccine
- Key finding: Efficacious in dengue-naive and pre-immune individuals
- PSM relevance: Shows stratified randomisation by serostatus; covers both adults and children
- Reference: Simões EAF et al., Obstet Gynecol, Feb 2025 - PMID: 39746212
- Design: Phase III, multicenter, randomised, double-blind
- Intervention: RSV PreF protein vaccine given during pregnancy (maternal immunisation)
- PSM relevance: Demonstrates special population RCT design (pregnant women), maternal-neonatal protection - links to MCH/immunisation programs
DRUG TRIALS
- Reference: Zhao L et al., JAMA, Aug 2024 - PMID: 38819983
- Design: Phase III, multicenter, randomised, placebo-controlled
- Intervention: Tirzepatide (GLP-1/GIP dual agonist) vs placebo in Chinese adults with obesity
- Key finding: Significant weight reduction
- PSM relevance: NCD prevention, obesity as a public health problem, drug trial example with dose-response arms
- Reference: Wharton S et al., N Engl J Med, 2025 - PMID: 40960239
- Design: Phase III, multicenter RCT
- Intervention: Oral small-molecule GLP-1 receptor agonist (no injection needed)
- PSM relevance: Very recent trial; shows evolution of drug delivery - relevant to NCD burden
- Reference: Piazza G et al., N Engl J Med, 2025 - PMID: 40888734
- Design: Phase IV RCT (post-marketing)
- PSM relevance: Perfect example of a Phase IV / post-marketing surveillance trial - a commonly asked exam distinction
How to Use These in Your Exam
| Trial | Best used to illustrate |
|---|---|
| RSV mRNA (PMID 38091530) | Phase II/III vaccine RCT, elderly population |
| Dengue TAK-003 (PMID 38245116) | Long-term RCT follow-up, tropical disease |
| MATISSE RSV (PMID 39746212) | Special population (pregnant women), maternal immunisation |
| Tirzepatide SURMOUNT (PMID 38819983) | Drug RCT, NCD, placebo control, dose-response |
| Apixaban VTE (PMID 40888734) | Phase IV / post-marketing trial |
Exam tip: When citing an example RCT, mention: trial name (if any), drug/vaccine, journal, year, phase, and key design feature (double-blind, placebo-controlled, multicenter). This impresses examiners and shows you read current literature.