A 40 years old female presents with melasma from past 4 years
Reading File
Finding Sources
Searching PubMed
melasma treatment management
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information. Let me compose the full clinical answer.
Melasma - Clinical Overview
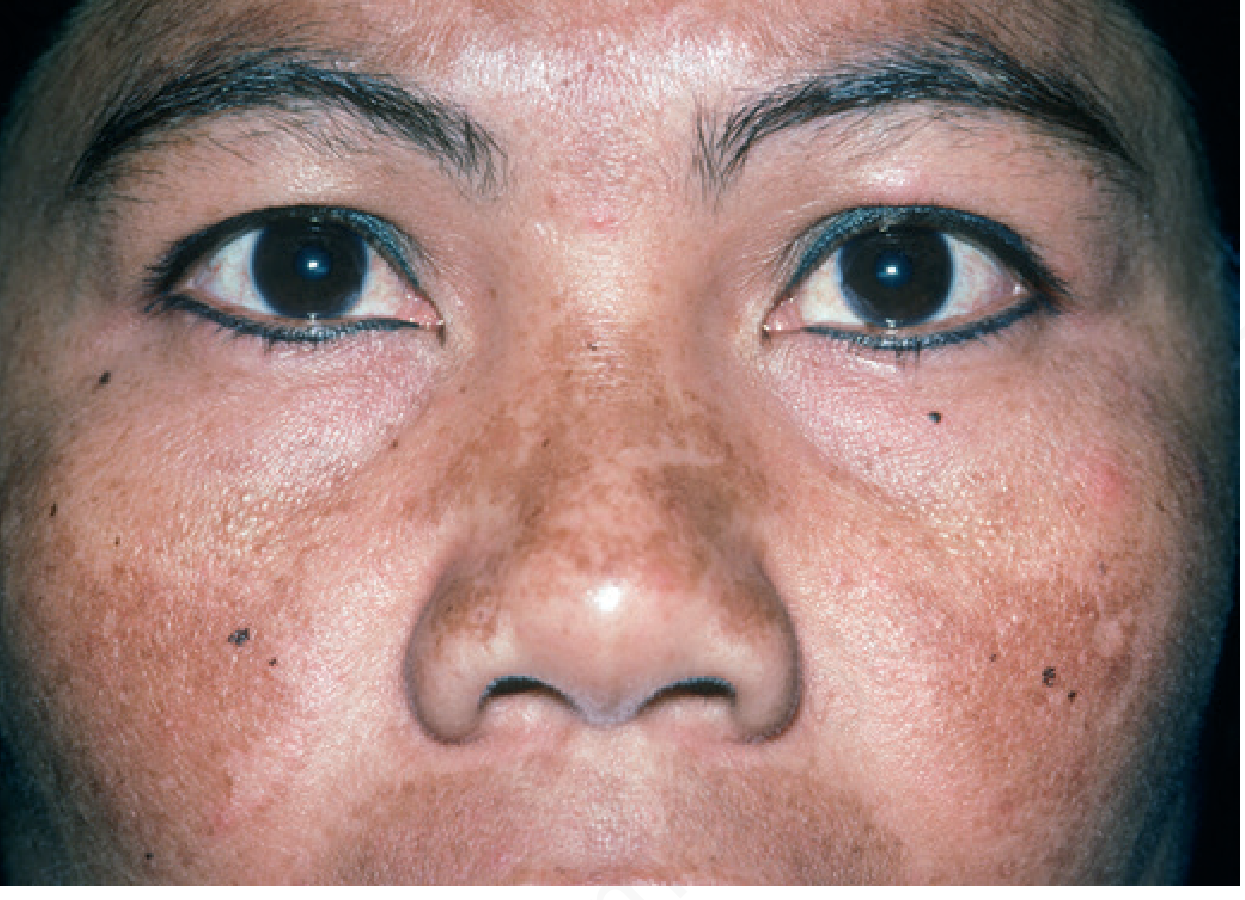
Classic melasma showing symmetric hyperpigmented patches over the malar prominences (Andrews' Diseases of the Skin)
Definition
Melasma (syn. chloasma, "mask of pregnancy") is a common acquired disorder of symmetric, hyperpigmented patches with irregular outlines, occurring most commonly on the face. It represents dysregulated melanogenesis driven by UV exposure and sex hormones, with a chronic relapsing course.
- Andrews' Diseases of the Skin, p. 993
- Dermatology 2-Volume Set 5e, p. 1343
Epidemiology & Risk Factors
| Factor | Detail |
|---|---|
| Sex | >90% female; F:M ~9:1 |
| Age | Young to middle-aged adults (peak 30s-40s) |
| Skin type | Fitzpatrick IV-V most affected; Hispanics, East/Southeast/South Asians, Black, Middle Eastern |
| Triggers | Sun exposure (primary), pregnancy, oral contraceptives (OCP), HRT |
| Other | Phenytoin, finasteride therapy, endocrinologic disorders |
In this 40-year-old female, key questions include OCP use, pregnancy history, sun exposure history, and Fitzpatrick skin type.
Pathogenesis
- UV exposure is the primary trigger: melasma affects sun-exposed areas, worsens in summer, patients have lower MED (minimal erythema dose), and solar elastosis is more marked in melasma-affected skin
- Wnt signaling: Melasma skin has reduced WIF-1 (Wnt antagonist) expression → increased Wnt → stimulates melanogenesis
- Hormonal influence: OCP, HRT, and pregnancy exacerbate via estrogen/progesterone-driven melanocyte stimulation; OCP-induced melasma often persists even after discontinuation
- Genetic predisposition: Correlation with number of melanocytic nevi
Andrews' Diseases of the Skin, p. 993
Classification
By Location (Clinical Patterns)
- Centrofacial - forehead, nose, upper lip, chin (most common)
- Malar - cheeks, nose
- Mandibular - jaw line
By Histological Depth
| Type | Melanin Location | Wood's Lamp | Treatment Response |
|---|---|---|---|
| Epidermal | Basal & suprabasal epidermis | Enhanced (accentuated) | Better |
| Dermal | Within melanophages | Not enhanced | Poor |
| Mixed | Both layers | Variable | Intermediate |
Note: Most cases show both epidermal and dermal melanin on histology and confocal microscopy - pure classification is unreliable. Dermal deposits respond poorly to topical agents.
Investigations / Workup
- Wood's lamp examination - helps broadly categorize (though unreliable for definitive typing)
- Dermatoscopy - useful to assess depth and rule out other pigmented lesions
- Dermoscopy findings: pseudonetwork of hyperpigmentation, telangiectasias in sun-damaged skin
- History: OCP use, pregnancy, sun habits, topical agents used
- Consider: ANA, thyroid antibodies (associated autoimmune conditions occasionally reported)
- Biopsy: Rarely needed; if diagnosis uncertain or exogenous ochronosis suspected
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Drug-induced hyperpigmentation | Less patterned, less irregular outline; history of offending drug (doxycycline, amiodarone) |
| Post-inflammatory hyperpigmentation (PIH) | History of inflammation; may not follow facial distribution |
| Riehl melanosis (Pigmented contact dermatitis) | Sites of cosmetic contact; brown-grey, lichenoid on histology |
| Ota's nevus / Horii nevus | Asian women; grey-blue macules; dermal melanocytes on histology |
| Lichen planus pigmentosus | Temples/preauricular; coexistent LP lesions (~20%) |
| Erythema dyschromicum perstans | Slate-grey, involves sun-protected areas too |
| Exogenous ochronosis | Progressive darkening after HQ use; banana-shaped deposits on histology |
| Actinic lichen planus | Fine scale, violaceous, lichenoid infiltrate |
Treatment
All Patients (Foundation)
- Broad-spectrum sunscreen SPF ≥30 daily (with physical blockers: zinc oxide or titanium dioxide; iron oxide added to block visible light via makeup/sunscreen)
- Avoidance of sun exposure and tanning beds
- Sun-protective hats and clothing
- Discontinue OCP if possible
- Camouflage makeup with iron oxide
Dermatology 2-Volume Set 5e, p. 1343
First-Line Topical Therapy
Kligman's Formula (Triple Combination) - gold standard:
- Hydroquinone 4% + Tretinoin 0.05-0.1% + Mild topical corticosteroid (class 5-7)
- Applied at bedtime
- Used daily for 2-4 months, then reduced to 1-2x/week for maintenance
- Most effective topical regimen available
Alternatives/Adjuncts:
- Hydroquinone 4% alone (bedtime)
- Azelaic acid 15-20%
Cautions: Overuse of the triple combo → fixed erythema, telangiectasias, acneiform eruptions, hypertrichosis. Prolonged HQ use → exogenous ochronosis. Corticosteroid overuse → perioral dermatitis, atrophy.
Adjunctive Topical Therapies
| Agent | Concentration | Mechanism |
|---|---|---|
| L-ascorbic acid (Vitamin C) | 10-15% | Inhibits tyrosinase, antioxidant |
| Kojic acid | 1-4% | Inhibits tyrosinase |
| Tranexamic acid | 2-5% | Inhibits plasminogen activator in keratinocytes → reduces prostaglandin-driven melanogenesis |
| Niacinamide | 4% | Inhibits melanosome transfer |
Adjunctive Oral Therapy
Tranexamic acid 250 mg BID for 8-12 weeks
- Screen patients for thromboembolism risk factors before prescribing
- Mechanism: inhibits UV-induced plasminogen activator activity in melanocytes and keratinocytes, reducing melanin synthesis
Recent meta-analyses confirm efficacy: a 2024 systematic review and a 2025 meta-analysis of intradermal tranexamic acid both support tranexamic acid (oral and intradermal) as effective for melasma management with good safety profiles. A 2025 meta-analysis also supports microneedling combined with tranexamic acid.
Second-Line (Procedural)
Chemical Peels (every 4-6 weeks):
- Glycolic acid (start 30%, increase as tolerated)
- Salicylic acid 20-30%
- Note: Peels alone have not reproducibly enhanced 4% HQ efficacy and risk PIH if irritation occurs
Third-Line (Light & Laser)
| Modality | Notes |
|---|---|
| Intense Pulsed Light (IPL) | Can improve melasma but high relapse rate |
| Non-ablative fractional laser | Best laser option; 60% of skin types III-V achieve 75-100% improvement; improves HQ penetration |
| Pulsed dye laser | May enhance topical combination therapy |
| Picosecond lasers | Emerging evidence |
| Q-switched Nd:YAG (low fluence) | Risk of increased pigmentation/punctate leukoderma - use cautiously |
| Er:YAG | Temporary improvement followed by PIH - generally avoided |
Light-based therapies carry risk of PIH, hypopigmentation, and scarring in darker skin types (Fitzpatrick IV-V). Always do a test site first.
Long-Term Maintenance
- Daily broad-spectrum sunscreen (non-negotiable)
- Topical retinoid (continues to suppress recurrence)
- Topical alpha-hydroxy acid (e.g. glycolic acid cream)
- L-ascorbic acid, azelaic acid, kojic acid, or topical tranexamic acid
Prognosis & Counselling Points
- Melasma is a chronic, relapsing condition - treatment suppresses but does not cure
- OCP-induced melasma often persists despite discontinuation (unlike melasma of pregnancy, which usually clears within months of delivery)
- Dermal melasma responds much more poorly than epidermal type
- Realistic expectations are essential - partial improvement is more common than complete clearance
- Even a Wood's lamp "epidermal" pattern often has some dermal component on histology
- Sun protection alone can modestly improve melasma and is indispensable for any treatment to work
Dermatology 2-Volume Set 5e, p. 2859 | Andrews' Diseases of the Skin, p. 993-994
Summary for this patient: A 40-year-old female with 4 years of melasma is a classic presentation. Assess Fitzpatrick type, OCP use, sun exposure, and prior treatments. Start with rigorous photoprotection, Kligman's formula (if tolerated), and consider adding oral tranexamic acid 250 mg BID for 8-12 weeks (screen for VTE risk). If inadequate response after 3-6 months, escalate to chemical peels or non-ablative fractional laser. Counsel on chronic relapsing nature and need for maintenance therapy.
This is a shared conversation. Sign in to Orris to start your own chat.