Explain me 10 common ecg change with reauly
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive textbook content and ECG images from Harrison's Principles of Internal Medicine. Here is the full, well-illustrated answer:
10 Common ECG Changes
Reference ECG - Normal 12-lead
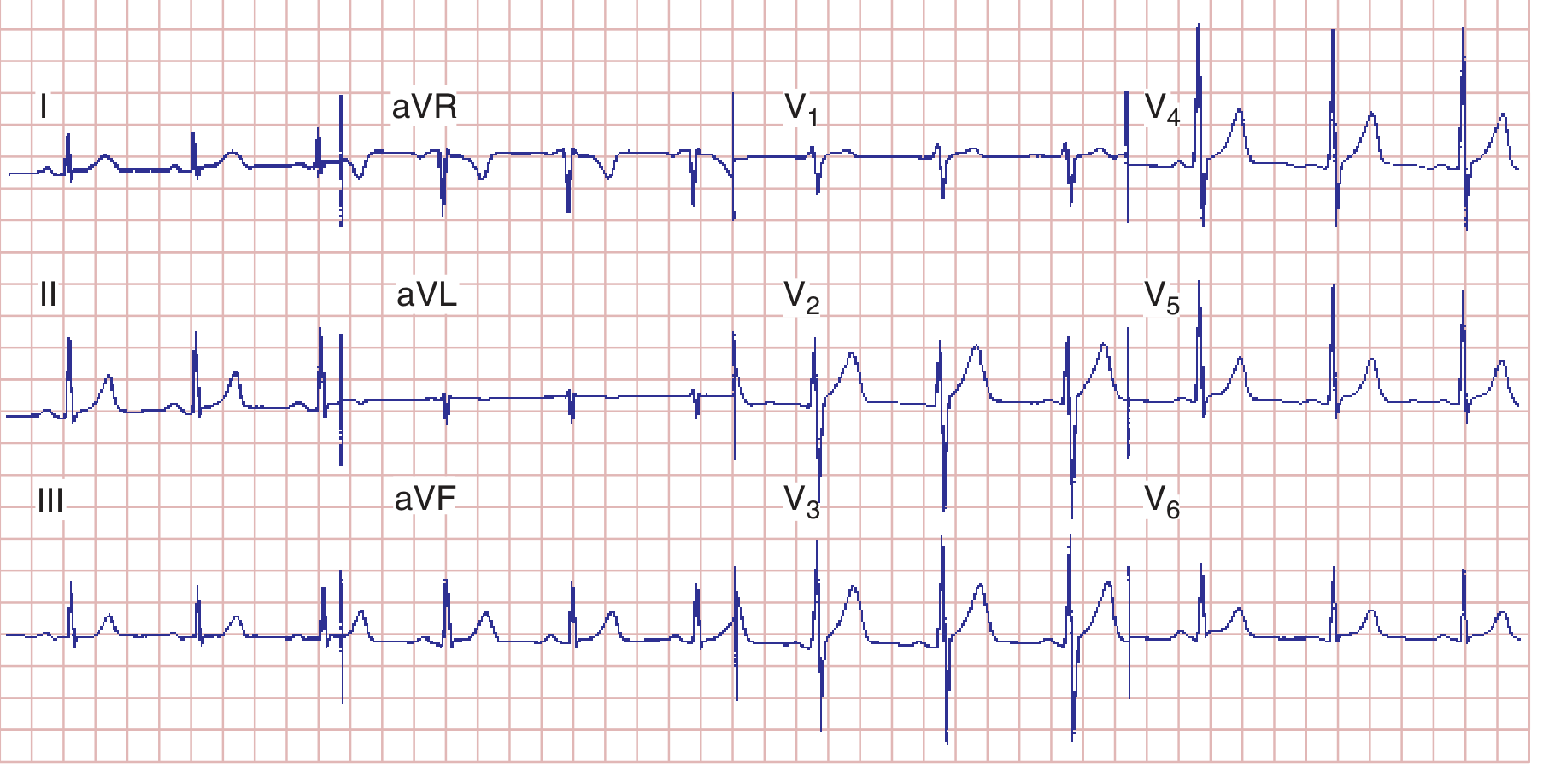
Normal sinus rhythm: HR 75 bpm, PR 160 ms, QRS 80 ms, QTc ~390 ms. This is your baseline for comparison.
1. ST Elevation (STEMI pattern)
What you see: ST segments raised ≥1 mm in two or more contiguous leads. The classic "tombstone" or convex upward shape indicates transmural ischemia/infarction.
Leads affected by territory:
- Anterior STEMI: V1-V4 (LAD)
- Inferior STEMI: II, III, aVF (RCA or LCx)
- Lateral STEMI: I, aVL, V5-V6
Key rule: Reciprocal ST depression appears in the "mirror" leads (e.g., inferior STEMI causes reciprocal depression in V1-V3).
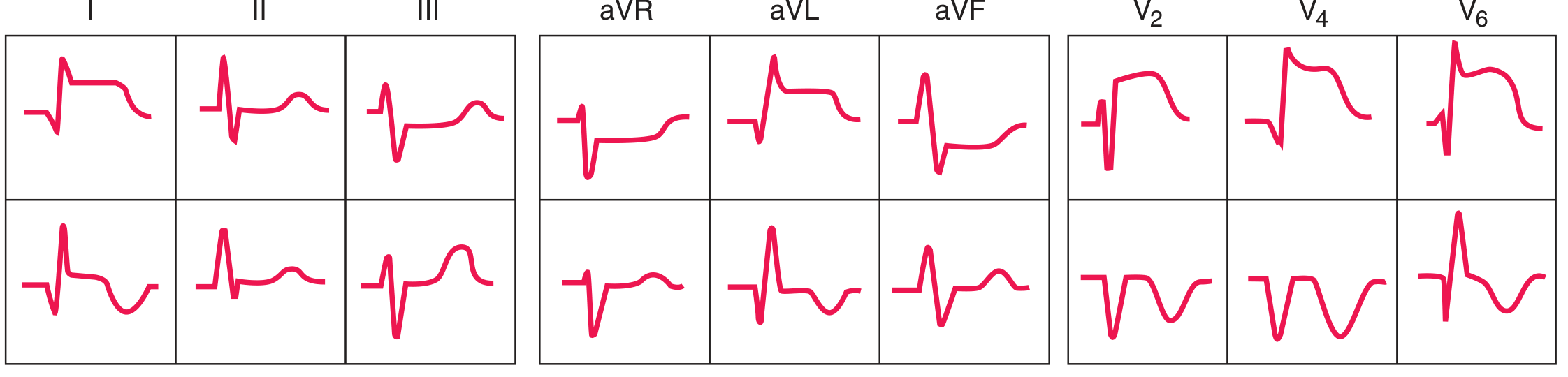
Top row = acute anterior STEMI; Bottom row = evolving inferior STEMI. Note ST elevation and subsequent Q-wave formation.
Other causes of ST elevation: Pericarditis (diffuse, saddle-shaped), Brugada pattern (right precordial, coved/saddle morphology), LVH strain, hypothermia (J/Osborn waves), hyperkalemia (V1-V3).
2. ST Depression
What you see: ST segment falls below the isoelectric line. Morphology matters:
- Horizontal or downsloping depression - strongly suggestive of ischemia or posterior STEMI
- Upsloping depression - less specific, can be a normal variant at high heart rates
Causes: Subendocardial ischemia/NSTEMI, posterior STEMI (depression in V1-V3 = "reciprocal" of posterior elevation), LVH strain pattern, digoxin effect ("scooped" or "reverse-tick"), hypokalemia, right ventricular hypertrophy.
3. Pathological Q Waves
What you see: Q wave ≥40 ms (1 small square) wide OR ≥25% the height of the following R wave, in two contiguous leads. These represent electrically dead (infarcted) myocardium that produces no depolarization signal.
Where they appear by territory:
- V1-V4: anterior infarct (LAD territory)
- II, III, aVF: inferior infarct
- I, aVL: high lateral infarct
Remember: Small q waves in I, aVL, V5-V6 are normal septal vectors; only qualify as "pathological" when they exceed the above criteria.
4. Right Bundle Branch Block (RBBB)
What you see:
- QRS ≥120 ms (wide complex)
- rSR' ("rabbit ears") in V1 - the R' is taller than the initial r
- Wide, slurred S wave in V6 and lead I
- T-wave inversion in V1-V3 (secondary repolarization change - discordant to the last QRS deflection)
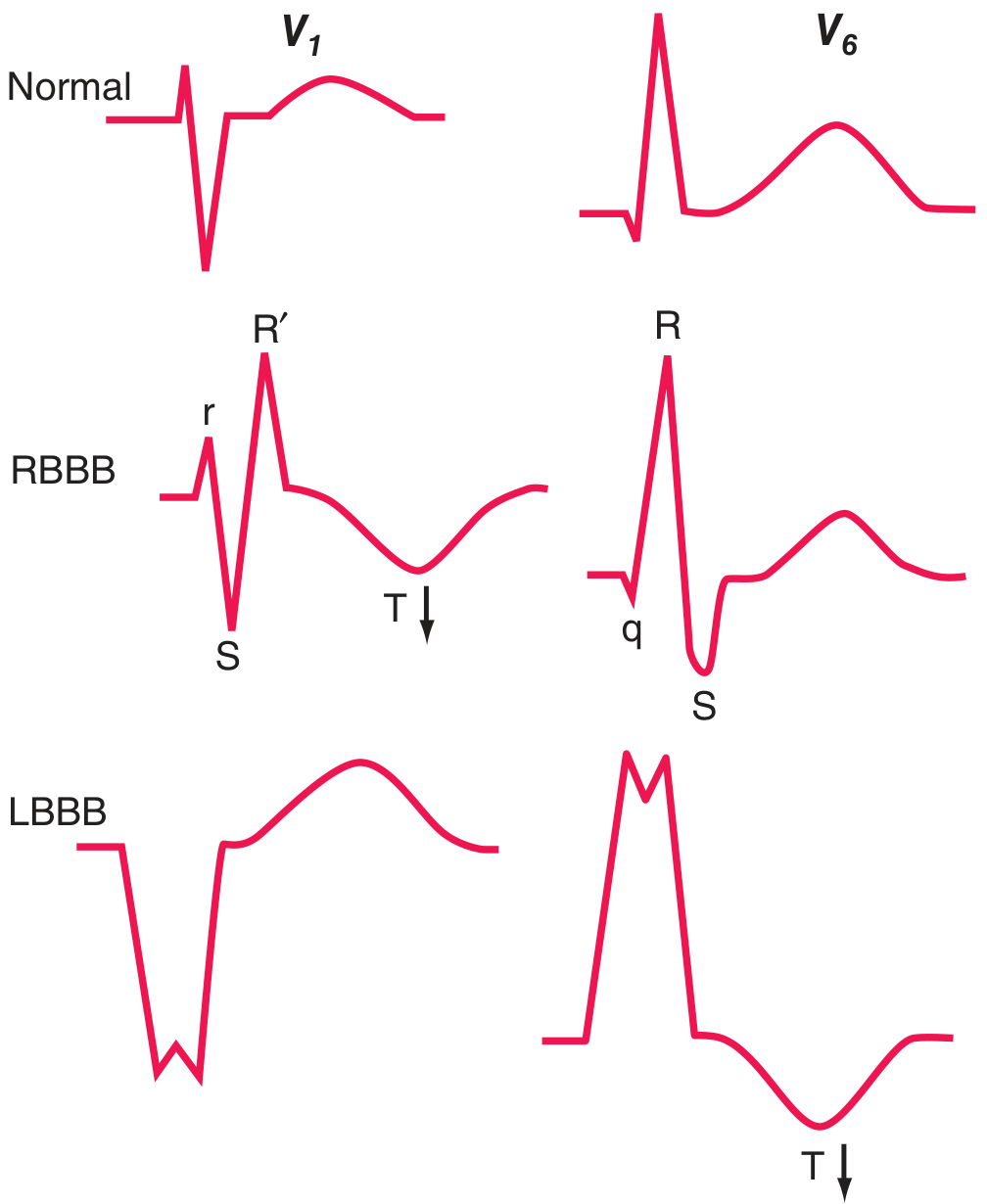
Top: Normal. Middle: RBBB - note rSR' in V1 and qRS in V6. Bottom: LBBB - note QS in V1 and wide R in V6.
Causes: Can be normal (no structural disease), atrial septal defect, pulmonary embolism, right heart strain, ischemic heart disease.
5. Left Bundle Branch Block (LBBB)
What you see:
- QRS ≥120 ms
- Broad, predominantly negative (QS) complex in V1 - no r wave
- Broad, monophasic R wave in V6 (no q, no s wave)
- Discordant T-wave inversion in leads with dominant R wave (V5-V6, I, aVL)
- Normal septal q waves are absent in lateral leads
Clinical importance: New LBBB in a patient with chest pain is treated as a STEMI equivalent until proven otherwise (Sgarbossa criteria apply). LBBB is frequently a marker of one of four underlying conditions: coronary artery disease, hypertensive heart disease, aortic valve disease, or cardiomyopathy.
6. Left Ventricular Hypertrophy (LVH)
What you see:
- Tall R waves in left lateral leads (R in aVL >20 mm in women, >28 mm in men)
- Deep S waves in right precordial leads (S in V1 + R in V5 or V6 >35 mm - Sokolov-Lyon criterion)
- LVH "strain" pattern: ST depression + T-wave inversion in leads with tall R waves (I, aVL, V5-V6)
- Left atrial abnormality is often coexistent (broad, notched P in II; biphasic P in V1)
Causes: Hypertension (most common), aortic stenosis, hypertrophic cardiomyopathy, athletic heart.
7. Right Ventricular Hypertrophy (RVH)
What you see:
- Tall R wave in V1 (R ≥ S in V1, or R >7 mm)
- Right axis deviation (QRS axis >+90°)
- Deep S waves in V5-V6 (prominent S in lateral leads)
- ST depression and T-wave inversion in right precordial leads (V1-V3) - "right ventricular strain"
- May also show qR pattern in V1 with severe pressure overload
Causes: Pulmonary hypertension, pulmonary stenosis, atrial septal defect (volume overload - associated with RBBB pattern), chronic lung disease.
8. Atrial Abnormalities (P-wave changes)
What you see:
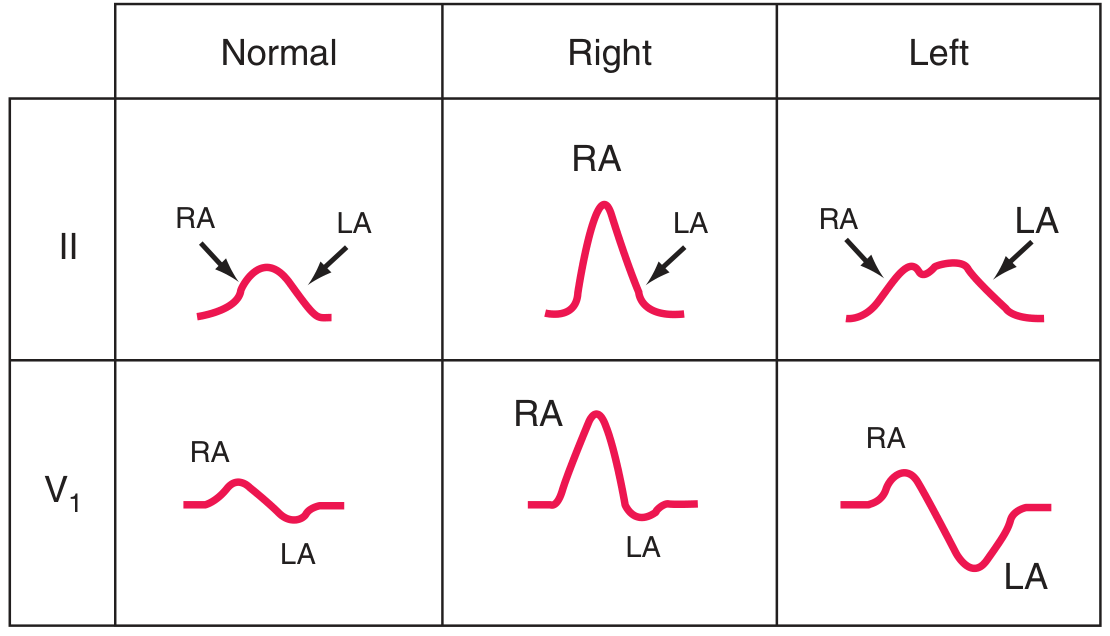
Left column: Normal P wave. Middle: Right atrial overload - tall, peaked P (≥2.5 mm) = "P-pulmonale." Right: Left atrial abnormality - broad, notched P in II; deep terminal negative deflection in V1 = "P-mitrale."
| Finding | Morphology | Cause |
|---|---|---|
| Right atrial overload | Tall peaked P ≥2.5 mm in II, III, aVF | Pulmonary hypertension, tricuspid stenosis |
| Left atrial abnormality | Broad (≥120 ms), notched P in II; biphasic P in V1 with prominent negative terminal | Mitral stenosis/regurgitation, LVH, left heart failure |
| Absent P waves | No identifiable P waves, irregularly irregular rhythm | Atrial fibrillation |
9. Hyperkalemia ECG Changes (Electrolyte Changes)
What you see (in sequence with rising K+):
- Mild-moderate (K+ 5.5-6.5 mEq/L): Peaked, "tented" T waves (tall, narrow, symmetric) - earliest sign
- Moderate-severe (K+ 6.5-8.0 mEq/L): PR prolongation, P waves flatten and disappear, QRS widens
- Very severe (K+ >8.0 mEq/L): Wide QRS merges with T wave producing a sine-wave pattern - risk of VF/asystole
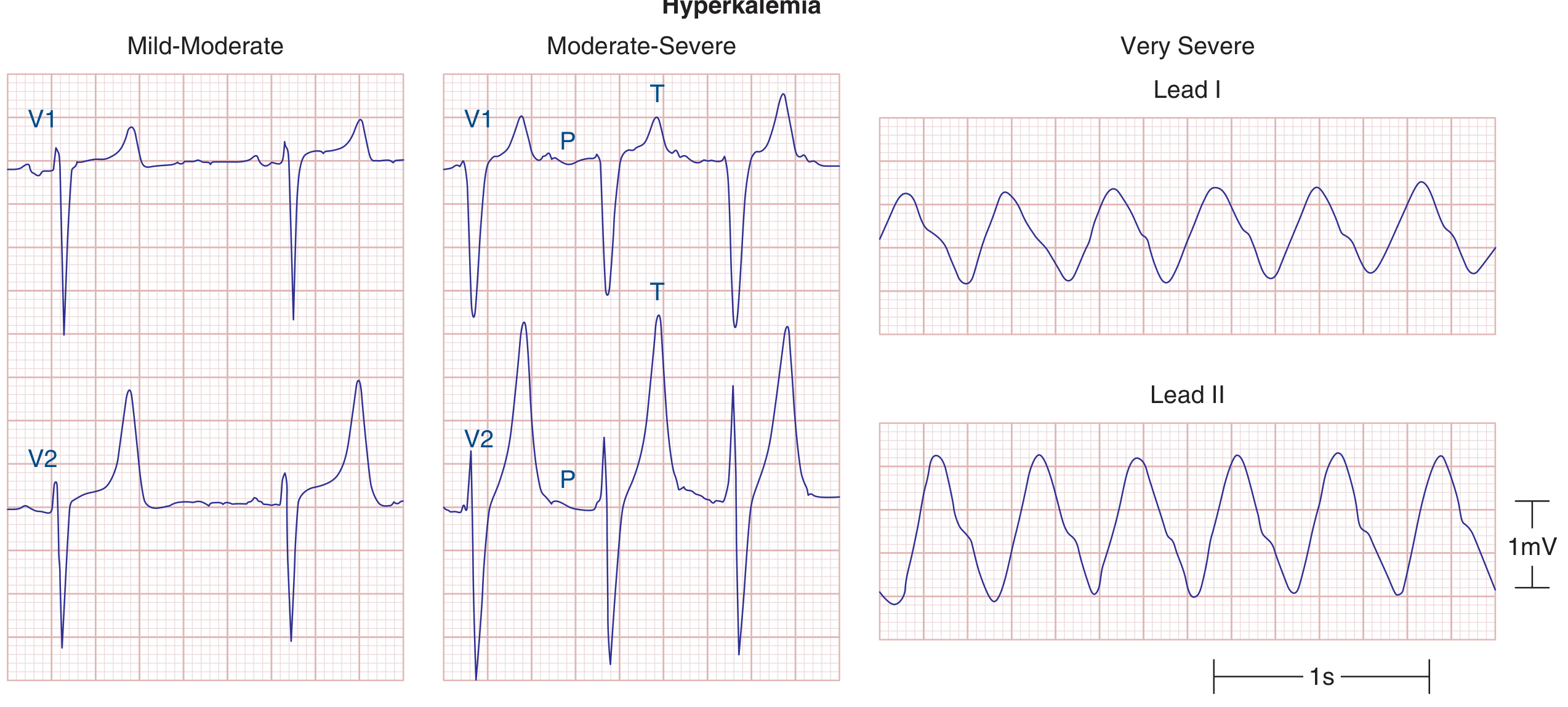
Mild-moderate (left): peaked T waves. Moderate-severe (middle): QRS widening, P waves still visible. Very severe (right): classic sine-wave pattern.
Hypokalemia ECG changes:
- ST depression, T-wave flattening/inversion
- Prominent U waves (a positive deflection after the T wave, most visible in V2-V3)
- Apparent QT prolongation (actually QU prolongation)
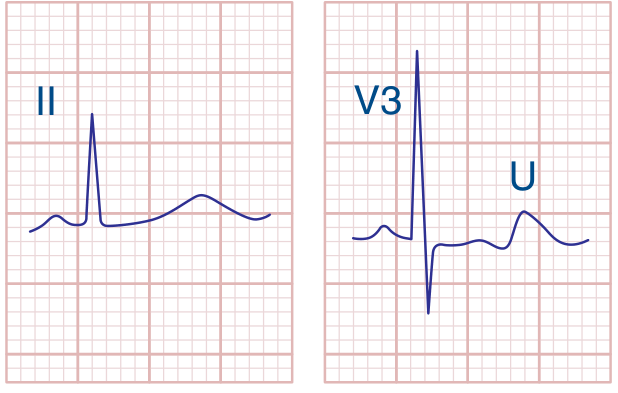
Hypokalemia: flat T wave with a distinct U wave in V3.
10. Prolonged QT Interval
What you see: The QT interval (from start of QRS to end of T wave) is prolonged when QTc (Bazett's formula: QT ÷ √RR) exceeds:
- >450 ms in men
- >460 ms in women (some sources use >470 ms)
Clinical significance: Prolonged QTc predisposes to torsades de pointes (TdP) - a polymorphic ventricular tachycardia that can degenerate into VF and cause sudden cardiac death.
Common causes:
| Category | Examples |
|---|---|
| Drugs | Class Ia/III antiarrhythmics (amiodarone, sotalol), antipsychotics (haloperidol, quetiapine), antibiotics (azithromycin, fluoroquinolones), methadone |
| Electrolytes | Hypokalemia, hypomagnesemia, hypocalcemia |
| Congenital | Romano-Ward syndrome (autosomal dominant), Jervell-Lange-Nielsen (with deafness) |
| Cardiac | Bradycardia, AV block, myocarditis |
| Other | Hypothyroidism, intracranial hypertension, hypothermia |
Quick Summary Table
| ECG Change | Key Feature | Common Cause |
|---|---|---|
| ST elevation | Raised ST in contiguous leads | STEMI, pericarditis, Brugada |
| ST depression | Depressed ST, horizontal/downsloping | NSTEMI, ischemia, LVH strain |
| Pathological Q waves | ≥40 ms wide or >25% R height | Prior MI |
| RBBB | rSR' in V1, wide S in V6, QRS ≥120 ms | Normal variant, PE, ASD |
| LBBB | QS in V1, broad R in V6, QRS ≥120 ms | CAD, HTN, cardiomyopathy |
| LVH | Tall R lateral + deep S right precordial | Hypertension, AS |
| RVH | Tall R in V1, right axis, S in V6 | Pulmonary HTN, PS |
| P-wave changes | Peaked (RA) or broad-notched (LA) | Lung disease, mitral disease |
| Hyperkalemia | Peaked T → wide QRS → sine wave | Renal failure, Addison's |
| Prolonged QT | QTc >450-460 ms | Drugs, electrolytes, congenital |
Sources: Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Harriet Lane Handbook, 23rd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.